Download presentation
Presentation is loading. Please wait.

1
CUSP-Stop CAUTI-Learning Session #2
The ICU Environment and Urinary Drainage Devices Good ________________! I want to thank Laura and the group here in SC for the invitation to be with you today for Learning Session #2. I have been asked to talk with you today about CAUTI prevention in the ICU environment. So, let me start off by asking how many ICU staff we have in the room-raise your hand if you work in ICU at this time. How many of you in the room are Infection Preventionists? Of those that are Ips, how many of you have worked in ICU in your past life? I have worked in an Adult Medical ICU in a large teaching hospital. I have served as a transport nurse on a Pediatric Flight Team, moving critically ill children to the PICU at University of North Carolina Health Care. Tina Adams, RN, Clinical Content Development Lead August 22, 2012

2
Objectives: Discuss incidence of urinary drainage device use and CAUTI in ICUs State the HIPAC/CDC indications for urinary drainage device use List 3 insertion best practices List 3 maintenance best practices Describe systems to increase the earlier removal of urinary catheters (UC) in ICU These are the expectations for my talk today. We’ll discuss Incidence, indications, insertion, maintenance, and removal in relation to the ICU environment.
 in ICU. These are the expectations for my talk today. We’ll discuss Incidence, indications, insertion, maintenance, and removal in relation to the ICU environment.")
3
CAUTI rate=outcome data
# of CA-SUTIs in a unit in a month x1000 # of Catheter Days in a unit in a month Signs and Symptoms of UTI: + Urine culture with uro-pathogen Fever > 38 degrees C Urgency Frequency Dysuria, pyuria (> 10 WBC unspun), +LE or Nitrate Suprapubic tenderness Costovertebral angle pain or tenderness Let’s set a few ground rules to begin. We are going to compare apples to apples because all of our units will use the same definition for CAUTI. First off, how is a CAUTI defined? What is the CAUTI rate of your unit…who determines if a patient has a CAUTI ? What are the approved signs and symptoms of UTI according to the NHSN (National Healthcare Safety Network) CDC? Does your electronic medical record have the ideal spot for you to document such findings? The CAUTI rate is the number of CAUTI per the CDC definition (requires symptoms) divided by the number of catheter days in a unit per month times 1000. CAUTI by definition requires symptoms, I’ve listed them here as a reminder to staff about symptoms that should be communicated to MD and documented in the MR.
, +LE or Nitrate. Suprapubic tenderness. Costovertebral angle pain or tenderness. Let’s set a few ground rules to begin. We are going to compare apples to apples because all of our units will use the same definition for CAUTI. First off, how is a CAUTI defined What is the CAUTI rate of your unit…who determines if a patient has a CAUTI What are the approved signs and symptoms of UTI according to the NHSN (National Healthcare Safety Network) CDC Does your electronic medical record have the ideal spot for you to document such findings The CAUTI rate is the number of CAUTI per the CDC definition (requires symptoms) divided by the number of catheter days in a unit per month times CAUTI by definition requires symptoms, I’ve listed them here as a reminder to staff about symptoms that should be communicated to MD and documented in the MR.")
4
Rate of CAUTI in ICUs: ICU type: No. of location CA-UTI UC days Rate
Burn 23 115 24,324 4.7 MICU-teaching 67 470 192,002 2.4 Medical-All other 110 436 232,454 1.9 Neuro-ICU 12 84 27,681 3.0 Neuro-Surg ICU 45 446 110,797 4.0 SICU-teaching 59 471 157,384 SICU-All other 53 182 118,919 1.5 PICU-Medical/ Surgical 78 127 57,420 2.2

5
Uro-pathogen microorganisms:
Gram-negative bacilli Staphylococcus spp. yeasts beta-hemolytic Streptococcus spp. Enterococcus spp. G. vaginalis, Aerococcus urinae, Corynebacterium (urease positive) This is a list of the approved uro-pathogens. These are the organisms that cause infection of the Urinary Tract.
 This is a list of the approved uro-pathogens. These are the organisms that cause infection of the Urinary Tract.")
6
Device Utilization Ratio/DUR=process data
# of catheter days=catheter prevalence # of patient days ICU’s catheter utilization ratio: (50 catheter days ÷ 100 patient days)=0.5 50% of ICU’s patient days are days in which patients are at risk of CAUTI! Data elements required to calculate this number are 1.) Catheter days and 2.) Patient days Divide the number of urinary catheter days by the number of patient days and this gives you the DUR-device utilization ratio, we call it the catheter prevalence. Why is this an important number to know and pay attention to? How can the number of days that the patients in your unit are at risk for CAUTI be lowered? WAIT………………. Less catheters=less catheter days=less risk for infection
=0.5 50% of ICU’s patient days are days in which patients are at risk of CAUTI! Data elements required to calculate this number are 1.) Catheter days and 2.) Patient days. Divide the number of urinary catheter days by the number of patient days and this gives you the DUR-device utilization ratio, we call it the catheter prevalence. Why is this an important number to know and pay attention to How can the number of days that the patients in your unit are at risk for CAUTI be lowered WAIT………………. Less catheters=less catheter days=less risk for infection.")
7
Rate of UC use in ICU: ICU type: No. of locations
Mean UC utilization ratio: Burn 23 0.51 MICU-teaching 67 0.73 Medical-All other 110 0.65 Neuro-ICU 12 0.82 Neuro-Surg ICU 45 0.74 SICU-teaching 59 0.76 SICU-All other 53 0.78 Peds-Med/ Surg. ICU 77 0.26

8
CAUTI Prevalence, Incidence
Most common site of HAI, ~ 30-40% Estimated >560,000 per year 80% of HAI-UTI attributable to catheter 15-20% patients in hospitals have urethral catheter Most catheterized for 2-4 days, longer Incidence of bacteriuria associated with indwelling cath is 3-8% per day These facts you have heard before, remember UC disturbs the host defense mechanisms and provides easier access of uro-pathogens to the bladder and kidneys. Because the kidneys are blood filtering organs…it is not far for the organisms to travel to get into the bloodstream once they get to the kidney. Remember bateriuria associated with indwelling urinary catheter will cause death in ____________% of our patients. This information covers all patients in the hospital, not just ICUs. CDC:

9
What’s the problem? 15% of HAI of the bloodstream are attributable to UTI 13,000 attributable deaths per year Increased length of stay by 2-4 days Increased cost $ billion annually in the US We have all thought that the UC was a given in the ICU! Just like we believed the central line was required for all ICU patients! We have been lulled into thinking UCs pose very little risk if any. But look at the fallout from those innocuous catheters! CDC:

10
CMS- payment rule changes:
Hospital-Acquired Conditions (HAC) HAI-CAUTI not reimbursed as of October 2008 Present on Admission (POA): Does your unit routinely order/obtain urine cultures when UC’d patients admitted? Do not obtain an admission urine culture UNLESS the patient has signs and symptoms of UTI Antibiotic stewardship Because CAUTI is so common and therefore costly, the payors have stopped paying hospitals for the care patients receive related to this hospital-acquired infection. As some attempt to document that patients have urinary tract infection Present on Admission, they have gone to sending urine cultures on admission. The NPT does not recommend this practice as it results in the treatment of bacteria in the urine which may not be an infection per se. Present on Admission- Does your unit routinely perform urine culture at admission or immediately when a UC is placed? National Project Team does not support this action as it is related to increased antibiotic usage-due to bacteriuria is treated more often. MORE CULTURES=More antibiotics
 HAI-CAUTI not reimbursed as of October Present on Admission (POA): Does your unit routinely order/obtain urine cultures when UC’d patients admitted Do not obtain an admission urine culture UNLESS the patient has signs and symptoms of UTI. Antibiotic stewardship. Because CAUTI is so common and therefore costly, the payors have stopped paying hospitals for the care patients receive related to this hospital-acquired infection. As some attempt to document that patients have urinary tract infection Present on Admission, they have gone to sending urine cultures on admission. The NPT does not recommend this practice as it results in the treatment of bacteria in the urine which may not be an infection per se. Present on Admission- Does your unit routinely perform urine culture at admission or immediately when a UC is placed National Project Team does not support this action as it is related to increased antibiotic usage-due to bacteriuria is treated more often. MORE CULTURES=More antibiotics.")
11
Complications related to UC:
Infection: Urinary tract infection (bladder) Acute pyelonephritis (kidney) Secondary bacteremia/sepsis(blood) Late onset: osteomyelitis (bone) and meningitis (brain) Infection may spread from the bladder to the kidneys, from there to the blood and bones and finally to the brain. Once the infection reaches the blood, sepsis and shock may ensue.
 Acute pyelonephritis (kidney) Secondary bacteremia/sepsis(blood) Late onset: osteomyelitis (bone) and meningitis (brain) Infection may spread from the bladder to the kidneys, from there to the blood and bones and finally to the brain. Once the infection reaches the blood, sepsis and shock may ensue.")
12
Complications related to UC con’t:
Adverse outcomes: Increased mortality Obstructions form to urine flow Selection for multi-drug resistant organisms Prostatitis and orchitis

13
Organisms that cause CAUTIs:
Short-term urinary catheterization causing bacteriuria is usually from a single organism: Bacteria: E. coli is most frequent GNR: Klebsiella spp, Serratia spp, Citrobacter spp, and Enterobacter spp, Pseudomonas aeruginosa, Proteus GPC: Enterococcus Fungi: Candida is most frequent Short term UC is about a week long and the bacteriuria caused is usually from a single organism whereas long term catheterization results in multiple organisms at one time. Where does the E. coli and Candida come from? Let’s examine the nearby flora.

14
Movement of organisms into urinary tract:
Extraluminal-Outside of catheter Intraluminal-Inside the catheter

15
This photo is a Staph aureus biofilm on an indwelling catheter.

16
Biofilm---what’s up with that?
Free floating microorganisms attach themselves to a surface Secrete extracellular polymers that provide a structural matrix and facilitate adhesion Biofilms protect the bacteria, they are often more resistant to traditional antimicrobial treatment A million cases of catheter-associated urinary tract infections (CAUTI) reported each year, many of which can be attributed to biofilm-associated bacteria Maki, D. and Tambyah, P. "Engineering Out the Risk for Infection with Urinary Catheters." Emerging Infectious Diseases 7.2 (2001)
 reported each year, many of which can be attributed to biofilm-associated bacteria. Maki, D. and Tambyah, P. Engineering Out the Risk for Infection with Urinary Catheters. Emerging Infectious Diseases 7.2 (2001)")
17
Normal flora of the Urethra:
CoN Staph Diphtheriods Streptococci (various species) Mycobacterium spp Bacteroides and Fusobacterium spp Peptostreptococcus spp Where do they come from? Not from the urethra!
 Mycobacterium spp. Bacteroides and Fusobacterium spp. Peptostreptococcus spp. Where do they come from Not from the urethra!")
18
Normal Flora of the GI Tract:
Small intestine: Lactobacillus spp Bacteroides spp Clostridium spp Mycobacterium spp Enterococci Enterobacteriaceae (e.g.,Klebsiella, Enterobacter) Small intestine content? Maybe…does you patient have a ileostomy that leaks?
 Small intestine content Maybe…does you patient have a ileostomy that leaks")
19
GI tract normal flora continued:
Large Intestine: E. coli Klebsiella spp Pseudomonas spp Acinetobacter spp Staph aureus Did our patient with CAUTI have a recent bout of diarrhea? Do you routinely give ICU patients stool softeners? Bowel programs? Fecal drainage systems?

20
Normal Flora of the Skin:
CoN Staph Diphtheroids Staph aureus Streptococci (various species) Bacillus spp Malassezia furfur Candida spp Where do the organisms that cause CATUI come from?
 Bacillus spp. Malassezia furfur. Candida spp. Where do the organisms that cause CATUI come from")
21
Normal Flora of the Vagina:
Lactobacillus spp Peptostreptococcus spp Diphtheroids Streptococci (various) Clostridium spp Bacteriodes spp Candida spp Gardnerella vaginalis Remember that when we give patients antibiotics, the normal bacterial flora will be killed off and the Candida will be therfore selected and overgrow!
 Clostridium spp. Bacteriodes spp. Candida spp. Gardnerella vaginalis. Remember that when we give patients antibiotics, the normal bacterial flora will be killed off and the Candida will be therfore selected and overgrow!")
22
Evidence-based Risk Factors:
Symptomatic UTI Bacteriuria Prolonged catheterization* Disconnection of drainage system* Female sex Lower professional training of inserter* Impaired immunity Placement of catheter outside of OR Older age Diabetes Meatal colonization Renal dysfunction Orthopedic/neurology services Some of these risk factors are modifiable and some are not. Let’s talk about the ones that we can work on. Who is the person at your hospital that places the UC? Do your patients come with a UC from OR, ED, LTCF? Ask you peers in your ED what level training staff are allowed to insert ? Ask your peers in the OR what level training staff are allowed to insert? How many of your patients with UC are receiving antibiotics? What do antibiotics do to the UG and perineal flora? How many of your patients are colonized with an MDRO If a patient is colonized with VRE, what percentage of this patient group will acquired a CAUTI with VRE? *Main modifiable risk factors

23
Lifecycle of the urinary catheter:
This is Dr. Meddings slide. Lifecycle of the urinary catheter. This conceptual model illustrates 4 stages of the urinary catheter lifecycle as targets for intervention to decrease catheter use and subsequent catheter-associated urinary tract infection. Meddings J , Saint S Clin Infect Dis. 2011;52:

24
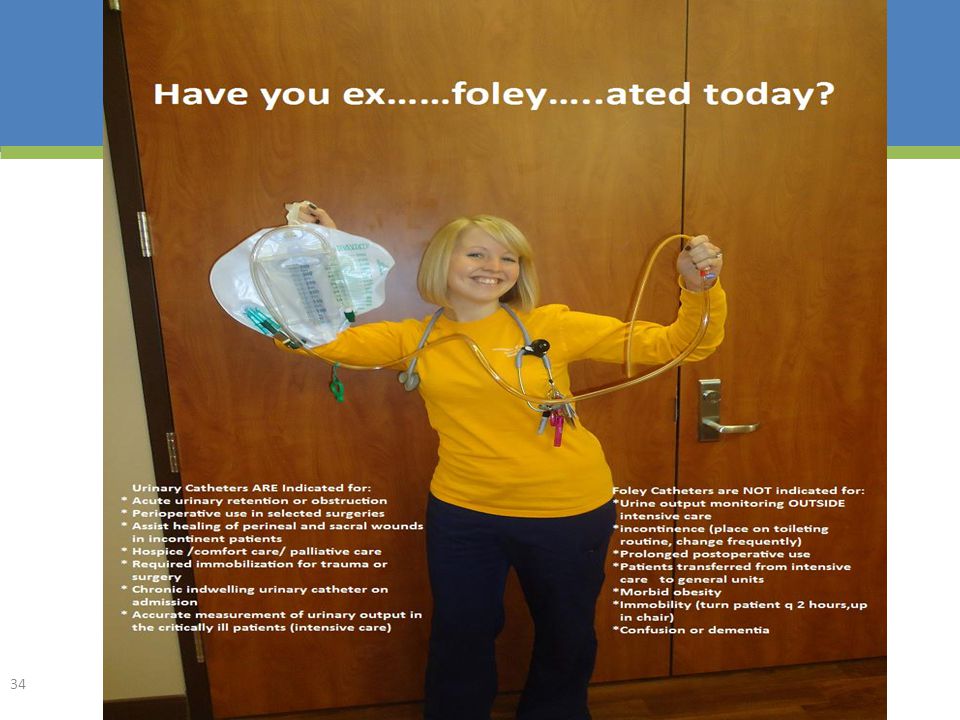
CDC’s INDICATIONS FOR UC:
Urinary retention/bladder obstruction Accurate measurement of urine output in critically ill patients (usually in an ICU) To assist with healing open sacral/ perineal wounds in the incontinent You noticed that these indications include a critically ill patient usually housed in the ICU. On any given day…how many patients get transferred out? Are those patient “critically ill” at that point? Do they meet any of the other indications to have a UC? Take it out! CDC:
 To assist with healing open sacral/ perineal wounds in the incontinent. You noticed that these indications include a critically ill patient usually housed in the ICU. On any given day…how many patients get transferred out Are those patient critically ill at that point Do they meet any of the other indications to have a UC Take it out! CDC:")
25
Indications continued:
4. Perioperative use-selected surgery: Urological surgery (or on contiguous structures of GU tract) Patient anticipated to receive large volume infusions or diuretics in OR Need for intraoperative monitoring of urine output (should be removed in PACU) Prolonged duration of surgery Does every surgery patient in your unit automatically have a UC placed? Do they ALL meet one of these 4 indications during surgical inpatient admissions? CDC:
 Patient anticipated to receive large volume infusions or diuretics in OR. Need for intraoperative monitoring of urine output (should be removed in PACU) Prolonged duration of surgery. Does every surgery patient in your unit automatically have a UC placed Do they ALL meet one of these 4 indications during surgical inpatient admissions CDC:")
26
4 RULES to Prevent CAUTI:
What can I do? 4 RULES to Prevent CAUTI: Prevent indwelling catheter use when another urinary care system would work! Optimize aseptic insertion technique Optimize aseptic maintenance care Remove the UC as soon as possible! You can begin the change process in your ICU by becoming a patient advocate and take an active role in the prevention of UC use whenever another urinary care system would work. Ok, we are going to talk about RULE #1 AND RULE#4 first and then come back to discuss RULE #2 and #3.

27
Alternative urinary care:
All Patients: Unconscious=Incontinence garment Conscious=Scheduled toileting-Q 4 hours The 3 B’s: Bedpan Bedside commode Bathroom Rule #1: What other options are available to provide urinary care for the ICU patient? Well, it depends on their level of consciousness-right? Obviously the higher the LOC the more actively involved the patient can be. If your pt is unconscious, there are fewer options-Depends. Once they are awake and able to communicate-it’s time for the 3B’s. Bedpan, Bedside Commode and the Bathroom! Do any of you have a scheduled toileting program in your unit? I am aware that for some of your patients this is a difficult proposition! Getting ICU patients up to the BR is a major event! But, by using a combination of these three assisted toileting processes, we are helping the patient avoid HAI and getting closer to graduation from ICU!

28
Alternatives continued:
Male Patients: Urinal-Q 4 hours while awake Condom catheter Size matters!-5 different sizes Materials matter!-old latex, new silicone If you believe that a condom catheter won’t stay on or that they leak, you haven’t used on recently! There are new manufacturers, new sizing and made from newer substances!

29
Paradigm shift: Remember Rule #1! Prevent urinary catheterization!
All ICU patients do not require a UC because they are in ICU! All ICU patients admitted via OR/PACU do not automatically need a UC! All ICU patients admitted via ED do not automatically need a UC! Ok, what do we know is the best way to prevent CAUTI? No Catheter! How are we going to begin to move our units in that direction? It’s going to require a new way of thinking, a new belief, a new rule!

30
Admission to ICU: Report: ask about urinary needs UC in place?
UC arrived presentation to hospital? UC placed in ED/OR-what indication? History: ask patient/family for indication and length of UC use? Assessment: consider removal to review for need

31
Asepsis during insertion:
Competency of inserter assessed? Assess patient’s anatomy! Look first, with adequate assistance! Wash perineum with soap and water before procedure, chose smallest catheter The Right Stuff? Use hand hygiene, sterile gloves, drape, sponges, an appropriate antiseptic or sterile solution for periurethral cleaning, and a single-use packet of lubricant jelly for insertion (ICU, ED, OR?) What does aseptic technique mean? In the acute care hospital setting, aseptic technique and sterile equipment is used for this procedure. Use the smallest bore UC possible, consistent with good drainage, to minimize bladder neck and urethral trauma Have all HCWs doing this sterile procedure been competency tested? How are those who do this procedure in ED, OR? Can Med. Students, Interns, Residents, Fellows do this without check off? Can Nursing Students, Nursing Assistants , Care technicians, Surgical Techs, etc…
 What does aseptic technique mean In the acute care hospital setting, aseptic technique and sterile equipment is used for this procedure. Use the smallest bore UC possible, consistent with good drainage, to minimize bladder neck and urethral trauma. Have all HCWs doing this sterile procedure been competency tested How. are those who do this procedure in ED, OR Can Med. Students, Interns, Residents, Fellows do this without check off Can Nursing Students, Nursing Assistants , Care technicians, Surgical Techs, etc…")
32
Paradigm shift continued:
Remember RULE #4: Remove the catheters sooner! All ICU patients that did have an indication for a UC may not need it the entire ICU stay. Check daily! Goal: Remove as soon as possible and before transfer out of ICU! Information Tech – automatic notification to MD Nurse-driven removal protocol? ICU Goals Sheet use contains device use check-in. What can be removed today? Fluid status stabilized? Urine output WNL? Inotropes D/C’d? Diuretics D/C’d? If patient is stable enough to be transferred-meaning no longer critically ill, then no longer meets that indication.

33
Urinary Catheter Removal Protocol:
Meet indication today? If not, obtain catheter removal order Remove catheter Assessment for and encourage voiding Up and walking, using commode, privacy If not spontaneously voiding-comfortable? Bladder scan, if >400cc, contact MD for straight catheterization order, continue intermittent x 24hr Website has an example nurse driven catheter removal protocol.

35
Asepsis during maintenance care:
Hand hygiene, standard precautions to clean the perineum daily with soap and water during bath, contamination from feces/drainage, & emptying bag Clean the catheter daily wiping crusting away from the urinary meatus and 4 inches down the catheter Maintain clean securement of catheter to prevent movement and traction. Tape vs. Stat-Loc® Once the UC is in place we must be vigilent to protect the patient’s urinary tract from microbes!

36
Maintenance continued:
Bag maintained below bladder: never laid on the bed/stretcher (patient transportation) never on the floor (radiology, PT/OT) Bag emptying technique: staff emptying many urinary drainage bags to total I/O require hand hygiene and clean gloves before touching each patient’s urine bag I know all of you know these steps for prevention of contamination of the drainage system. This is what to do, can you be sure you have the system to do this every time? Illinois hospital obtain hooks for IV poles to make this more consistently practiced. The end of shift I/O practices of some units have been observed to be so bad that they had to never assign the nursing staff to more than one patient with a UC/drainage bag.
 never on the floor (radiology, PT/OT) Bag emptying technique: staff emptying many urinary drainage bags to total I/O require hand hygiene and clean gloves before touching each patient’s urine bag. I know all of you know these steps for prevention of contamination of the drainage system. This is what to do, can you be sure you have the system to do this every time Illinois hospital obtain hooks for IV poles to make this more consistently practiced. The end of shift I/O practices of some units have been observed to be so bad that they had to never assign the nursing staff to more than one patient with a UC/drainage bag.")
37
Not found to decreases CAUTI:
Routine change of UC or bag Washing the perineum with harsh antiseptics Placing antiseptics into the collection bag Routine bladder irrigations Antiseptic or silver-impregnated catheter

38
Objective #1: Can you review your unit’s data to discuss the
incidence of urinary drainage device use and CAUTI in your ICU?

39
Objective #2: Can you state the HIPAC/CDC indications for
urinary drainage device use?

40
Objective #3: What 3 insertion best practices are you going to
validate (by observation) consistently take place in your ICU?
 consistently take place in. your ICU")
41
Objective #4: What 3 maintenance best practices are you going to
validate (by observation) consistently take place in your ICU?
 consistently take place in. your ICU")
42
Objective #5: Describe one system you can institute to increase the
earlier removal of urinary catheters (UC) in your ICU?
 in your ICU")
43
Thank you for your participation in today’s discussion!
Questions or Comments? Thank you for your participation in today’s discussion!

44
Contact Information: Tina Adams, RN American Hospital Association Health Research & Education Trust

Similar presentations


 CATHETER RELATED URINARY TRACT INFECTIN (CR-UTI)>")
>")















