Download presentation
Presentation is loading. Please wait.

1
UTI prevention: Implementing Best Practice
Theresa Murray RN, MSN, CCRN, CCNS Critical Care Clinical Nurse Specialist President, Critical Concepts, INC.

2
Catheter Related Urinary Tract Infections
700, ,000 UTI’s occur each year and make up 36%-40% of all hospital acquired infections 4% of those patients with a UTI will develop a blood infection, which increases risk of death Increases length of stay by 1-4 days Adds approximately $676 to the cost of hospitalization. If blood infection develops the cost increases to $2,836 Estimated to cause 1 death per 1000 episodes of catheterization and contribute to over 6,500 deaths per year in the United States

3
How Infections Happen Introduction of bacteria into the bladder at the time of catheter insertion Bacteria can travel from the peri-anal area into the bladder along the outer surface of the catheter Bacteria can travel into the bladder from the drainage bag along the inner surface of the catheter

4
Compliance With 2005 JCAHO Hospital National Patient Safety Goal
Reduce the risk of health care associated infections Comply with current Centers for Disease Control and Prevention (CDC) hand hygiene guidelines Manage as sentinel events all identified cases of unanticipated death or major permanent loss of function associated with a health care associated infection
 hand hygiene guidelines. Manage as sentinel events all identified cases of unanticipated death or major permanent loss of function associated with a health care associated infection.")
5
Sentinel Event (JCAHO Criteria)
An event that has resulted in an unanticipated death or major permanent loss of function, not related to the natural course of the patient’s illness or underlying condition

6
Sentinel Event Identified by an unnamed facility
The sentinel event was investigated using “Root Cause Analysis” Root Cause Analysis Focuses on the process and system, not individuals Looks for common and special causes by digging deeper by continuing to ask “Why” Identify changes to the process and system that reduce the risk of the event happening in the future.

7
Actual Root Cause Analysis
A patient was admitted for a surgical procedure, requiring a catheter for the duration of the surgery and the immediate post op period The patient suffered a stroke post operatively and the catheter remained in place the duration of the hospital stay. The patient was transferred to an ECF after the hospital stay with the catheter still in place and returned to a related hospital with urosepsis in less than 1 hour after discharge. The patient died two days later as a result of septic shock

8
Root Cause Analysis Results
Documentation related to foley catheters was often not complete or non existent. Policy for Insertion of Foley Catheters was not being followed. Identified inappropriate use of foley catheters for nursing convenience Absence of guidelines for insertion and removal of foley catheters throughout the facility

9
Actions/Policy Changes
Developed insertion and removal guidelines for foley catheters. Policy was appropriate but not being followed. The only change is the requirement to document why the catheter is still needed based on the insertion guidelines every 8 hours. Developed a new tab “Urinary Catheter Tab” in CIS to improve foley catheter documentation in computerized areas Areas without computerized documentation will continue to use the appropriate form for that unit

10
Insertion Guidelines Any patient requiring strict I and O and who is unable to cooperate with bathroom, bed pan, or urinal. (Assess daily for continued need for strict I and O) Any patient with an inability to void when intermittent catheterization is difficult Any patient requiring monitoring of acute renal insufficiency or failure unless anuric Any patient who is chemically paralyzed Any patient who is post prolonged cardiac procedure with femoral arterial sheath Any patient undergoing a urological procedure Unable to avoid contamination of incision and or femoral central line Remove catheter as soon as possible when the above issues are resolved
 Any patient with an inability to void when intermittent catheterization is difficult. Any patient requiring monitoring of acute renal insufficiency or failure unless anuric. Any patient who is chemically paralyzed. Any patient who is post prolonged cardiac procedure with femoral arterial sheath. Any patient undergoing a urological procedure. Unable to avoid contamination of incision and or femoral central line. Remove catheter as soon as possible when the above issues are resolved.")
11
The Best Way to Prevent Foley Catheter Related Infections
Use catheters ONLY when necessary and by removing them when no longer needed.

12
Methods For Reducing and Preventing Catheter Related UTI’s
Handwashing Sterile technique during insertion and handling of the catheter Adequate training/competency of all staff What staff interact with foley cath?? P T, nursing, medicine, the patient. Transporters etc Routinely use 14 fr to reduce trauma Keep the drainage bag below the level of the bladder at all times (including when moving the patient from the bed to cart).
.")
13
Do not put the bag on the bed or on top of patient’s legs or belly.
Antimicrobial catheters Bright sticker on the foley drainage bag that says do not…… Work with ED, cath lab, OR if foley placed and the patient is expected to have a stay in the ICU-Urometer… closed system

14
Methods for Reducing and Preventing Catheter Related UTI’s
Maintain a closed system Obtain specimens from port aseptically Keep tubing kink free Secure catheter to patients leg Cleanse perineal area daily Assess daily for continued need Remove as soon as need resolved MD order? Create protocol Use smallest catheter, if patient has leakage go to smaller cath…. Meatus will close down on it.

15
Documentation Requirements
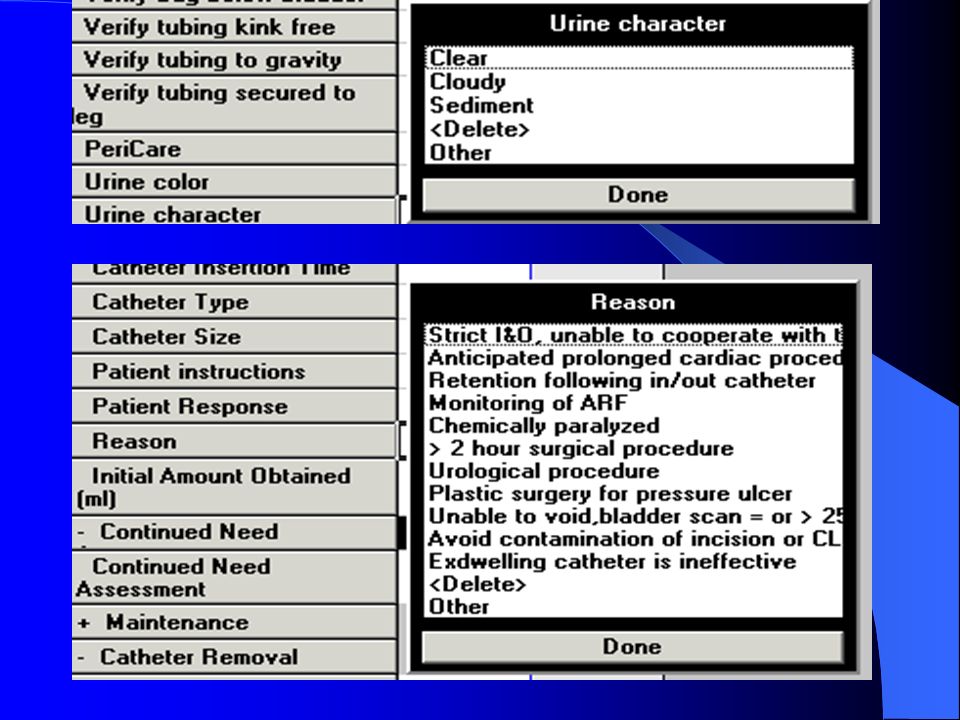
Insertion Performance of procedure Reason for catheterization based on insertion guidelines Size of catheter and balloon Amount, character, and color of urine Patient’s response Instruction given to patient and patient response

16
Documentation Requirements
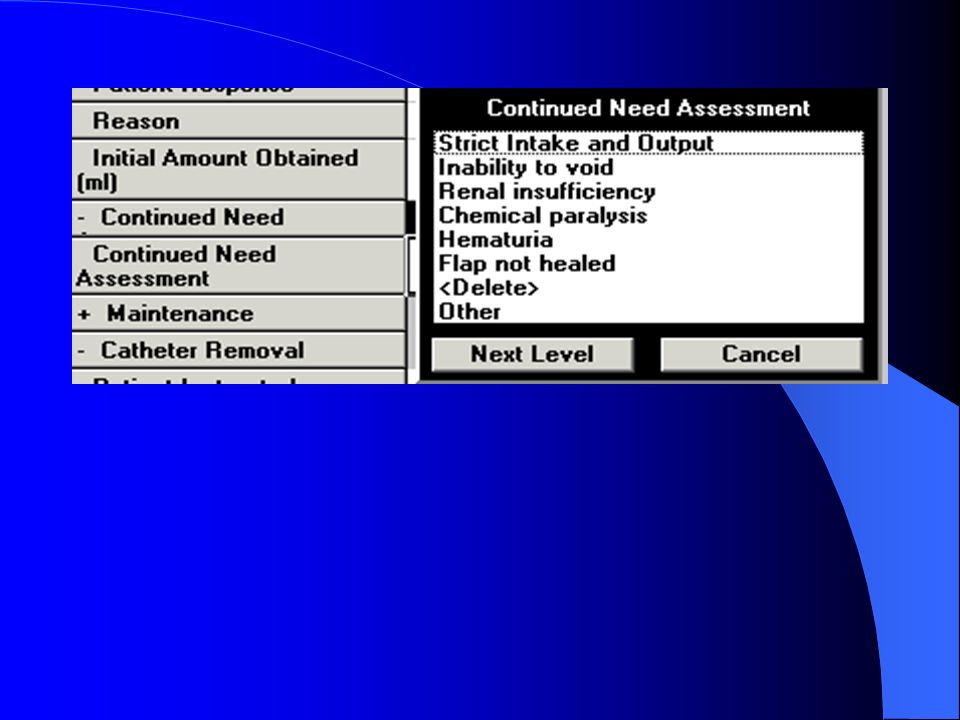
Maintenance of Catheter Continued need for catheter based on insertion criteria Amount, character, and color of urine Every 8 hours

17
Documentation Requirements
Discontinuation Performance of procedure Amount, character, color of urine Patient ’s response Instruction given and patient’s response If patient can ambulate take it out…. Don’t train the PT staff to keep it below the waist

18
Documentation Requirements For Those Areas With Computerized Documentation
Documentation requirements are the same as those without computerized documentation. Documentation will be required on the “Urinary Tab” on the CIS Flowsheet See following “snapshots” of the new flowsheet

19
New Urinary Catheter Tab

22
So What? Significant Reduction in all ICU’s
All units below 10th in NNIS Compliance with documentation remains a challenge

23
Questions comments pushback?
Thank you! Theresa Murray RN MSN, CCRN CCNS, EIEIO President, Critical Concepts, INC. Critical Care Clinical Nurse Specialist Community Health Network, Indianapolis

Similar presentations




 CATHETER RELATED URINARY TRACT INFECTIN (CR-UTI)>")
>")













