Download presentation
Presentation is loading. Please wait.

1
NURSE DRIVEN FOLEY CATHETER PROTOCOL

2
BACKGROUND There are over 1.7 million hospital-acquired infections in US hospitals annually, 40% of which are urinary tract infections. 80% of hospital-acquired UTIs are attributable to indwelling urethral catheters. Between 12% and 25% of all hospitalized patients in the US will have a urinary catheter during their hospital stay, almost half of which are not placed for an appropriate indication. The duration of catheterization is directly related to risk for developing a UTI. The daily risk of developing a catheter-associated UTI (CA-UTI) ranges from 3-7%. TJUH began working on reducing CA-UTIs in 2008. NDFP is the next step in this process
 ranges from 3-7%. TJUH began working on reducing CA-UTIs in NDFP is the next step in this process.")
3
Centers for Medicare and Medicaid Services estimates that the cost of CA-UTI is between $424 and $451 million annually. Beginning on October 1, 2008 CMS no longer pays for “preventable hospital-acquired complications” including CA-UTI. CA-UTI received a high priority because of its high cost, high volume, and because it can be reasonably prevented through application of accepted evidence-based prevention guidelines.

4
GOALS Reduce the number of catheter associate urinary tract infections (CA-UTIs), as well as reduce catheter days. Improve patient care and outcomes at TJUH. Reduce length of stay (LOS) and increase cost- effectiveness.
 and increase cost- effectiveness.")
5
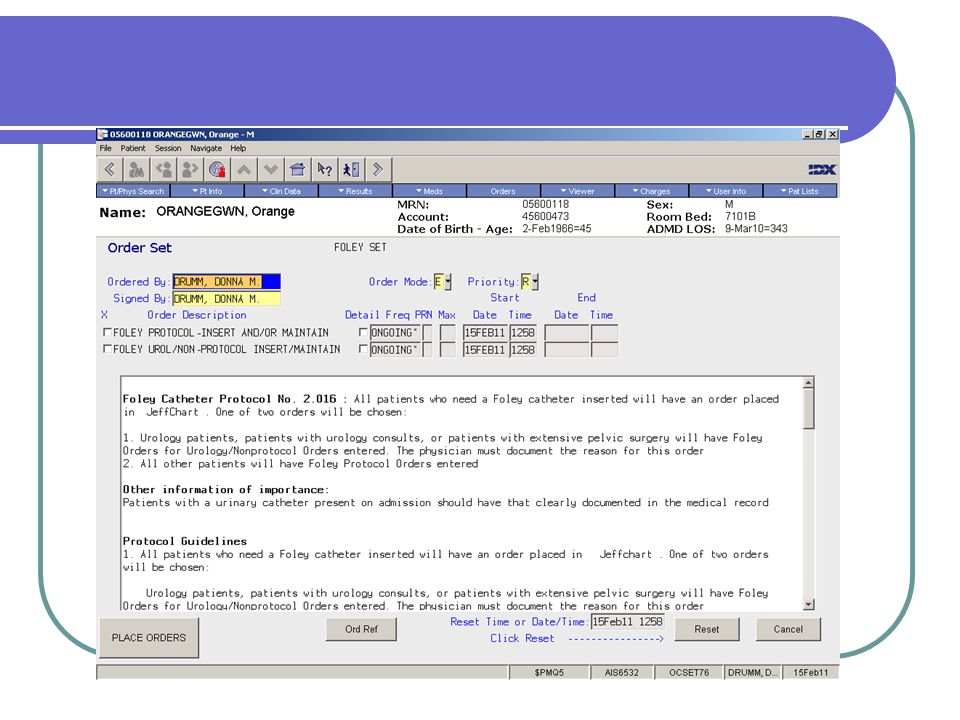
IMPLEMENTATION All inpatients admitted to Jefferson who have or may require indwelling urinary catheters, excluding those with NDFP protocol exceptions , will have Nurse Driven Foley Protocol orders.

6
Several components of care can be uniformly recommended for all patients to prevent or reduce risk of CA-UTI. These components are: Avoid unnecessary urinary catheters, Insert using aseptic technique Maintain catheters based on recommended guidelines, Review urinary catheter necessity daily and remove promptly.

7
INSERT WHEN APPROPRIATE
Appropriate indications include: Urinary retention/obstruction Close monitoring of urinary output Pre/Peri/Post Operative Management (epidural in place; femoral sheath in place.) Bladder Training Unstable Hip or Spinal Injury Incontinence with Stage III or IV skin breakdown (perineal or sacral) Palliative Care/End of Life Care Urology Service patients
 Bladder Training. Unstable Hip or Spinal Injury. Incontinence with Stage III or IV skin breakdown (perineal or sacral) Palliative Care/End of Life Care. Urology Service patients.")
8
ALTERNATIVES TO FOLEYS
Intermittent straight catheterization with the aid of bladder scanning Use of external catheters for male patients.

10
ASEPTIC INSERTION Wash hands thoroughly before and after insertion
Use barrier precautions during insertion Use smallest catheter possible to help prevent trauma Follow insertion procedure

11
CATHETER MAINTENANCE Assess need for Foley daily and document in JeffChart and/or progress note. Daily AM Care: Cleanse around catheter and meatus with soap and water daily and prn. Limiting manipulation of the catheter reduces infection. Secure the catheter with a leg band: Leg bands help keep the catheter in place and decrease pulling and twisting. Avoid bladder irrigation unless obstruction has occurred. Keep Drainage Bag BELOW the Bladder: This prevents retention and reflux back into the bladder, which can increase infection

12
Keep Drainage bag OFF the Floor: To avoid contaminating the spout.
Use individual graduated container for EACH Patient/label with name EMPTY the drainage bag before transport to avoid reflux Maintain a Closed System: Take urine samples through the port Always scrub the hub first before taking a sample If a urimeter is needed, change just the bag. It is better to disconnect in this case rather than insert a new catheter

14
REVIEW AND REMOVE SHEA/IDSA compendium October 2008: “The duration of catheterization is the most important risk factor for development of infection.” The necessity of a bladder catheter should be addressed by physicians daily as a part of rounds, and by nursing as part of their assessment. Nursing is empowered to remove catheters when protocol patients no longer meet the appropriate indications

15
FOLEY CARE BUNDLE The Foley Bundle incorporates the elements of Foley catheter insertion and maintenance, and should be referred to each shift to help decide whether or not a Foley is indicated.

16
Nurse Driven Foley Catheter Protocol
Criteria for Inserting/Continuing a Foley Catheter All patients who need a Foley catheter inserted will have an order placed in Jeffchart . One of two orders will be chosen: Urologic patients and some surgical patients with special needs will have Foley Orders for Urology/Nonprotocol Orders entered. All other patients will have Foley Protocol Orders entered. Thereafter, the RN is responsible to continually assess the need for the catheter and properly monitor catheter use. If any of the following criteria is met, the foley catheter will remain in place: Urinary retention/obstruction Close monitoring of urinary output required Pre/Peri/Post Operative Management (epidural in place; femoral sheath in place.) Bladder Training Unstable Hip or Spinal Injury Incontinence with Stage III or IV skin breakdown (perineal or sacral) Palliative Care/End of Life Care Urology service Patients (as ordered) Physician order to remain
 Bladder Training. Unstable Hip or Spinal Injury. Incontinence with Stage III or IV skin breakdown (perineal or sacral) Palliative Care/End of Life Care. Urology service Patients (as ordered) Physician order to remain.")
20
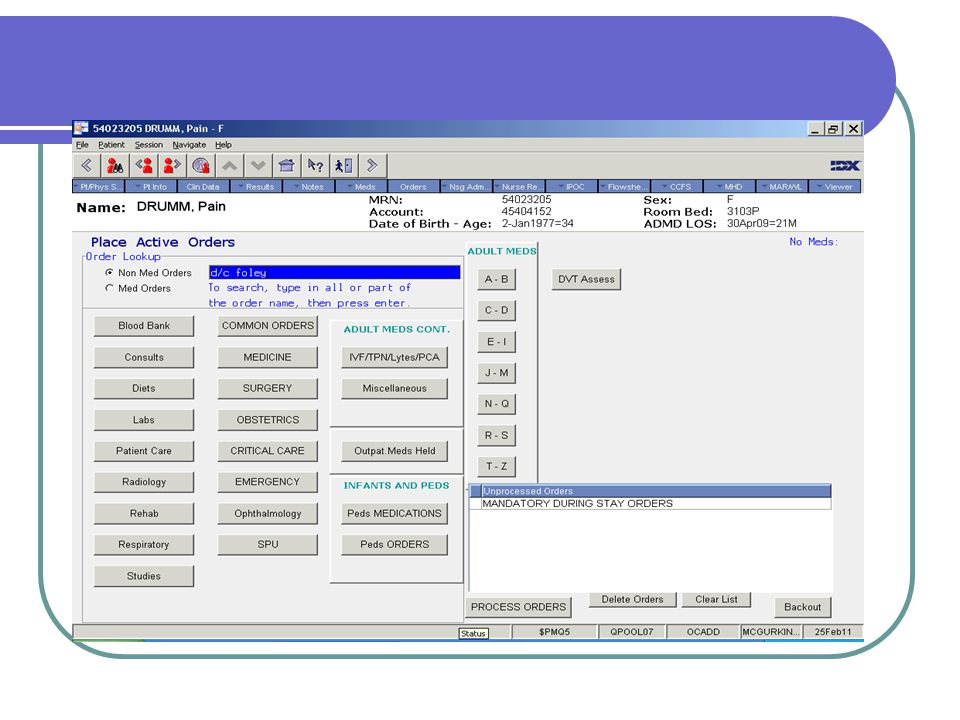
Criteria for Removal by RN without a separate Physician order
If the patient does not meet any of the above criteria, the RN may discontinue the foley catheter when the following criteria are met:

21
The patient is awake, alert and oriented and/or can verbally express that they had no trouble voiding before the catheter was placed. Patient is able to resume their normal voiding position, or at least one that is presently comfortable. A physician order for strict I&O is discontinued or the patient is able to cooperate with strict I&O monitoring If a foley is present post invasive cardiac or radiological procedure, confer with physician to remove foley unless there is a clear reason for not discontinuing the foley. Epidural catheter is removed.

22
NOTE: A physician order is required for discontinuing the foley for patients who have had recent urologic surgery, bladder injury, pelvic surgery (i.e. GYN, colorectal surgery) and/or recent surgery involving structures contiguous with the bladder or urinary tract. These patients should NOT have Foley Protocol orders but rather Foley Orders for Urology/Non-protocol Patients.
 and/or recent surgery involving structures contiguous with the bladder or urinary tract. These patients should NOT have Foley Protocol orders but rather Foley Orders for Urology/Non-protocol Patients.")
23
The staff nurse will then need to discontinue the present order by putting “Protocol user” in the “ordered by” and “signed by” fields, and changing the Order Mode to Protocol order or Written order. The patient will subsequently be monitored according to the “ Post Foley Removal Assessment and Care” guidelines listed below.

26
Post Foley Removal Assessment and Care Guidelines
After removal of the foley catheter, the patient will be continually assessed by the RN for the following Patient is spontaneously voiding. Patient is not voiding however is comfortable and expresses no need to void

27
A bladder scan should be done for any of the following:
If the patient is uncomfortable at anytime, whether voiding or not If the patient has an urge to void but is unable to do so The patient has not voided for 6 hours post foley removal If the patient is incontinent at anytime

28
If the bladder scan volume is >400cc, the RN will notify the MD and obtain an order for straight catheterization q6 hours and prn The volume of each bladder scan and output with catheterization must be recorded in the I and O record.

29
NOTE: If the patient once again meets the criteria for foley placement, a new physician order is required.

30
QUESTIONS? Feel free to ask your CNS/Educator for guidance as we implement this new protocol

31
MONITORING Infection Control will provide monthly CAUTI rates and catheter utilization rates to the patient care units. These rates will be used to monitor success with the implementation of this protocol. CNSs/Educators will continue monthly Point Prevalence collection on Foley Bundle compliance.

32
We want YOU…….. To get the foley out!

33
References CDC Guideline. (1981). Prevention of Catheter-Associated Urinary Tract Infections, CDC website Hansen, B. (2006). Reducing Nosocomial Urinary Tract Infections through Process Improvement, Journal of Healthcare Quality, Web Exclusive, 28(2), p.2-7. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36: Klevens RM, Edwards JR, Richards CL Jr, et al. Estimating health care-associated infections and deaths in U.S. hospitals, Public Health Rep Mar-Apr;122(2): Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med Jul 8;113 Suppl 1A:5S-13S. Centers for Medicare & Medicaid Services. Medicare program: changes to the hospital Inpatient Prospective Payment Systems and fiscal year 2008 rates. Fed Regist. 2007;72(162): Lo E, Nicolle L, Classen D, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals. Infect Control Hosp Epidemiol Oct;29 Suppl 1:S
. Reducing Nosocomial Urinary Tract Infections through Process Improvement, Journal of Healthcare Quality, Web Exclusive, 28(2), p.2-7. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36: Klevens RM, Edwards JR, Richards CL Jr, et al. Estimating health care-associated infections and deaths in U.S. hospitals, Public Health Rep Mar-Apr;122(2): Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med Jul 8;113 Suppl 1A:5S-13S. Centers for Medicare & Medicaid Services. Medicare program: changes to the hospital Inpatient Prospective Payment Systems and fiscal year 2008 rates. Fed Regist. 2007;72(162): Lo E, Nicolle L, Classen D, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals. Infect Control Hosp Epidemiol Oct;29 Suppl 1:S")
Similar presentations






>")



: A Prevention Plan>")












