Download presentation
Presentation is loading. Please wait.

1
Department of Medicine Manipal College of Medical Sciences
MEDIASTINAL DISEASES ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal

2
What is mediastinum ? Mediastinum is the space in the middle of the chest between the two pleurae Extends from the sternum to the spine Contains ALL the viscera in the thorax except the lungs

3
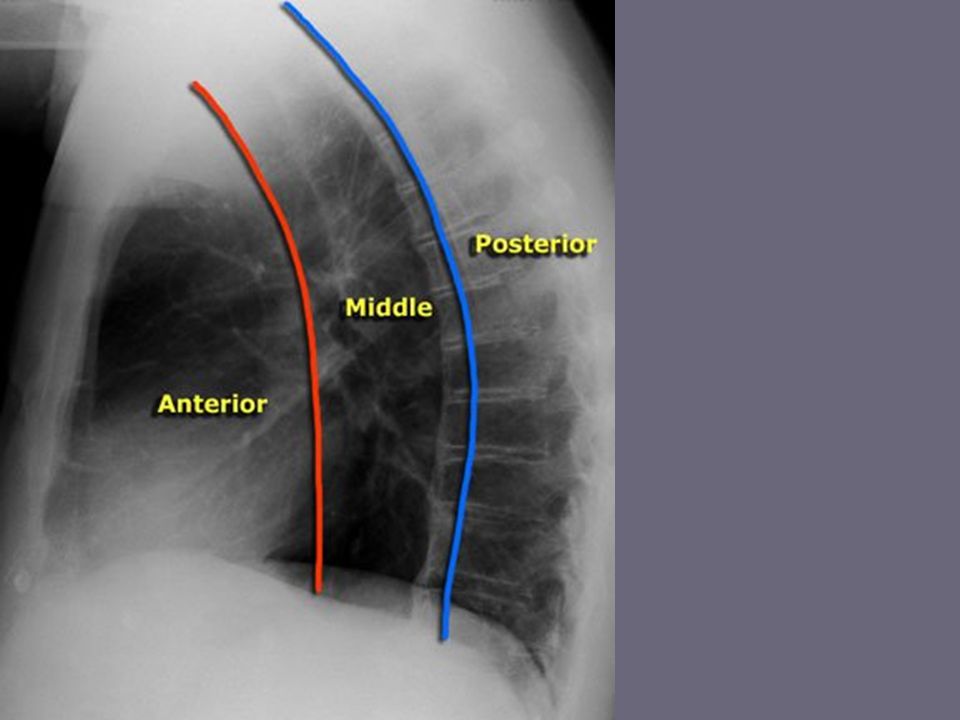
Divisions of Mediastinum
Posterior Superior Anterior Middle

4
Subdivision of mediastinum as seen on cross section
. Subdivision of mediastinum as seen on cross section anterior mediastinum (1) middle mediastinum (2) posterior mediastinum (3)
 middle mediastinum (2) posterior mediastinum (3)")
6
Superior mediastinum Boundary
Inferiorly: by the transverse thoracic plane – oblique plane passing posteriorly from sternal angle of Louis to the junction of the 4th and 5th thoracic vertebra Superiorly: line from sternum to T1 Laterally: by the pleurae

7
Contents Arteries Muscles AORTIC ARCH & its bracnches
Brachiocephalic artery Thoracic portions of the left common carotid and the left subclavian veins Innominate veins and Upper half of the superior vena cava Left highest intercostal vein Muscles origins of the Sternohyoid and Sternothyreoid

8
Nerves Trachea Esophagus Thoracic duct Remains of the thymus
phrenic nerve left recurrent laryngeal nerve vagus nerve cardiac nerve superficial and deep cardiac plexuses Trachea Esophagus Thoracic duct Remains of the thymus Some lymph glands

9
Anterior mediastinum-in front of the heart
Bounded in front by the sternum behind by the pericardium at the sides by the pleurae It contains remains of thymus gland origins of the sterno-hyoid, sterno-thyroid, and the triangularis sterni muscles internal mammary glands of the left side lymphatic vessels, and loose areolar tissue

10
Middle Mediastinum: Contains Heart & pericardium Ascending aorta
Lower half superior vena cava with vena azygos opening into it Bifurcation of trachea and two bronchi Pulmonary arteries and veins Phrenic nerves Some lymphatic glands

11
Posterior Mediastinum:
Bounded In front by pericardium and roots of lungs Behind by vertebral column At the sides by the pleurae Contains Descending aorta Oesophagus Azygos veins Vagus Splanchnic nerves Thoracic duct Some lymphatic glands

12
Mediastinal diseases 1. Mediastinitis 2. Pneumomediastinum
Infection or inflammation in the mediastinum acute Chronic 2. Pneumomediastinum Air in the mediastinum

13
3. Mediastinal mass Commonly caused by Tumor Cyst Vascular anomaly
Lymph nodes

14
SOME CAUSES OF A MEDIASTINAL MASS
Superior mediastinum Retrosternal goitre Thymic tumour Dermoid cyst Lymphoma Aortic aneurysm Anterior mediastinum Pericardial cyst Hiatus hernia through the diaphragmatic foramen of Morgagni

15
Posterior mediastinum
Neurogenic tumour Paravertebral abscess Oesophageal lesion Aortic aneurysm Foregut duplication Middle mediastinum Bronchial carcinoma Lymphoma Sarcoidosis Bronchogenic cyst Hiatus hernia

16
Trachea and main bronchi
SYMPTOMS AND SIGNS - MALIGNANT INVASION OF THE STRUCTURES OF THE MEDIASTINUM Trachea and main bronchi Stridor Breathlessness Cough Pulmonary collapse Oesophagus Dysphagia Phrenic nerve Diaphragmatic paralysis Left recurrent laryngeal nerve Paralysis of left vocal cord giving rise to hoarseness and 'bovine' cough Body_ID: B019082

17
Sympathetic trunk Superior vena cava Pericardium
Horner's syndrome Ptosis Meiosis enopthalmos anhydrosis Superior vena cava Non-pulsatile distension of neck veins Subconjunctival oedema Oedema and cyanosis of head, neck, hands & arms Dilated anastomotic veins on chest wall Pericardium Pericarditis and/or pericardial effusion

20
Which one is “invasion” and which is “compression” ?

21
Benign tumours and cysts:
Frequently diagnosed on unrelated X ray of the chest Do not invade vital structures May cause symptoms by compressing Trachea Superior vena cava

22
Malignant mediastinal tumours: Can be due to
invade as well as compress bronchi & lungs Can be due to Mediastinal lymph node metastases Lymphomas & leukaemia Malignant thymic tumours Aortic and innominate aneurysms have destructive features resembling those of malignant mediastinal tumours

23
INVESTIGATIONS !

24
1. Radiological examination
Benign mediastinal tumour sharply circumscribed opacity situated mainly in mediastinum often encroaching on one or both lung fields Malignant mediastinal tumour no clearly defined margin general broadening of the mediastinal shadow CT (or MRI) is the investigation of choice for mediastinal tumours
 is the investigation of choice for mediastinal tumours.")
25
Liposarcoma

28
2. Endoscopic investigation:
Bronchoscopy may reveal a primary bronchial carcinoma causing mediastinal tumour by secondary lymphatic spread

29
Posterior mediastinum can be imaged by
3. Ultrasonography Posterior mediastinum can be imaged by Transoesophageal ultrasound Needle biopsies of lymph node masses may be obtained under USG through endoscope

30
4. Surgical exploration 1. Mediastinoscopy: tissue from enlarged lymph nodes in ant. mediastinum can be removed for histological examination 2. surgical exploration of the chest with removal of part or all of the tumour often required to obtain a histological diagnosis

31
Management Benign mediastinal tumours removed surgically because
Most produce symptom sooner or later Cysts may become infected Neural tumours may undergo malignant transformation Low operative mortality in absence of Coexisting cardiovascular disease COPD Extreme age

32
MEDIASTINAL INFECTIONS

33
Acute Mediastinitis Most cases are due to: 1. Oesophageal perforation
spontaneously (Mallory weiss syndrome) complication of esophagoscopy Acutely ill with chest pain and dyspnea Treatment is surgical exploration of the mediastinum with primary repair of the esophageal tear and drainage of the pleural space and the mediastinum
 complication of esophagoscopy. Acutely ill with chest pain and dyspnea. Treatment is surgical. exploration of the mediastinum with primary repair of the esophageal tear and drainage of the pleural space and the mediastinum.")
34
2. After median sternotomy for cardiac surgery
Presentations with sepsis or widened mediastinum Treatment includes immediate drainage & debridement parenteral antibiotic therapy mortality still exceeds 20%.

35
Chronic Mediastinitis
Ranges from Granulomatous inflammation of lymph nodes to Fibrosing mediastinitis Due to TB Histoplasmosis & other fungal infections Sarcoidosis Silicosis

36
Patients with fibrosing mediastinitis usually have compression of
superior vena cava large airways phrenic or recurrent laryngeal nerve paralysis pulmonary artery or proximal pulmonary veins Other than antituberculous therapy for tuberculous mediastinitis, no medical or surgical therapy has been demonstrated to be effective for mediastinal fibrosis

37
Pneumomediastinum

38
Gas in the interstices of the mediastinum Causes are:
(1) alveolar rupture with dissection of air into the mediastinum (2) perforation or rupture of the esophagus, trachea, or main bronchi (3) dissection of air from the neck or the abdomen into the mediastinum
 alveolar rupture with dissection of air into the mediastinum. (2) perforation or rupture of the esophagus, trachea, or main bronchi. (3) dissection of air from the neck or the abdomen into the mediastinum.")
39
Excessive coughing Repeated bearing down to increase abdominal pressure (such as pushing during childbirth or a bowel movement) Sneezing Vomiting Rapid rises in altitude, SCUBA diving Tearing of the esophagus Tracheal tear Use of vevtilator Using inhaled recreational drugs such as crack cocaine

40
Symptom Severe substernal chest pain
With radiation into the neck and arms Pain may worsen on breathing or swallowing With which disease it is likely to be confused ?

41
Physical examination reveals
Subcutaneous emphysema in suprasternal notch small bubbles of air is felt under the skin of the chest, arms, or neck Hamman's sign (crunching or clicking noise synchronous with the heartbeat and best heard in the left lateral decubitus position) Diagnosis is confirmed with chest X ray
 Diagnosis is confirmed with chest X ray.")
42
Pneumomediastinum

44
A previously healthy 18 year old male had chest pain of sudden onset.
Heart sounds were normal but crunching and clicking sounds were heard over the left sternal border An ECG was normal

48
Usually no treatment is required
Mediastinal air will be absorbed faster if the patient inspires high concentrations of oxygen Compression can be relieved with needle aspiration Surgery for tracheal or esophageal tear

Similar presentations