Download presentation
Presentation is loading. Please wait.

1
ناهنجاریهای قامتی توراکولومبر
دکتر احمد باقری مقدم متخصص پزشکی ورزشی

2
What is Body Posture? Medical Dictionaries :
Body Posture = Body Alignment. Body Posture = The position of the body Body Posture = Relative alignment of body segments Body Alignment =The alignment of the various body parts to each other // How the torso, limbs, spine, shoulders are all in proper arrangement. . Posture = Posture is the position in which you hold your body upright against gravity while standing, sitting or lying down.

3
In medicine, the concept of good posture is referred to as "neutral spine".
In its natural alignment, the spine is not straight in side view . slight forward curve in the lumbar region(lordosis) slight backward curve in the thorasic region (kyphosis) slight extension in the tiny cervical vertebra at the top of the spine. In addition, the ears, shoulders, hips, knees and ankles are aligned properly.
 slight backward curve in the thorasic region (kyphosis) slight extension in the tiny cervical vertebra at the top of the spine. In addition, the ears, shoulders, hips, knees and ankles are aligned properly.")
4
Normal Spine Curvature
Posterior (Back) Spinal Column Lateral Spinal Column A non-neutral spine leads to "improper posture " increased stress on spine and causes pain, discomfort and damage. Normal Spine Curvature
 Spinal Column. Lateral. Spinal Column. A non-neutral spine leads to improper posture increased stress on spine and causes pain, discomfort and damage. Normal Spine Curvature.")
5
Static & Dynamic Posture:
In static postures the body and its segments are aligned and maintained in certain positions e.g. – Standing, kneeling, lying , sitting , … A dynamic posture refers to postures in which the body or its segments are moving e.g. – Walking, running, jumping, throwing, lifting , …

6
What holds the bodies in proper body alignment?
The muscles. When all muscles get the proper amount of stimulus & work, bodies naturally conform to this proper body alignment. Movement is easy and painless . We can run , jump , climb , throw, ….

7
What is proper body posture?
Proper Body Posture or Alignment is a balanced position in which the body's load-bearing joints are aligned It occurs when all the muscles are in well balanced position - front to back, side to side, top to bottom. Stress to the joints, muscles, vertebrae and tissue is minimized.

8
When the body is in this state, the musculoskeletal system functions optimally in its strongest.
The body bears the force of gravity with minimal effort. The body can move freely.

9
Correct or Optimal Posture
“…the state of muscular and skeletal balance which protects the structures of the body against injury or progressive deformity .” Maximal biomechanical efficiency. Minimal stress on the joints, the ligaments and the muscles. -

10
Increased strain on body and less efficient
Poor Posture “…faulty relationship of the various parts of the body which produces increased stress on the structures and in which there is less efficient balance of the body over its base of support.” Increased strain on body and less efficient Cause of various physiological and anatomical impairments AAOS: American Academy of Orthopaedic Surgeons

11
Causes of Poor Posture :
Structural Causes Permanent anatomical deformities not amenable to correction by conservative treatments. Positional Causes Poor postural habit - The individual does not maintain a correct posture. Psychological factors, especially depression & loss of self-esteem & … . General muscle weakness. Loss of the ability to perceive the position of your body. Loss of flexibility …. مثل ایمبالانس عضلانی Amenable تابع ،قابل جوابگويى

12
Muscle Imbalance When one of the muscles is either too strong or too weak, it becomes difficult to hold the joint in natural place. E.g. : One who only does sit-ups ,but doesn’t exercise the lower back muscles. This leads to very strong muscles in the front of the tummy area but relatively weaker back muscles. This lead to a slightly hunched forward posture.

13
Muscle Imbalances Imbalance between an agonist muscle & its antagonist : Disrupting the normal force couple relationship between the agonist & antagonist muscles Create kinetic dysfunction, Improper joint alignment, Muscle Imbalances often due to : Muscle tightness Muscle hyperactivity Muscle weakness Muscle hypoactivity

14
Some Causes of Muscle Imbalances:
Bad posture Muscle stretch or weakness Stretch – weakness may be defined as the effect on muscle of remaining in a lengthened condition behind its physiologic position. Muscle shortness & loss of flexibility Pain Sports & repetitive movment : That emphasize anterior muscles Unilateral activities Joint abnormalities & injuries Trauma Inactivity ……..

15
Soft Tissue Imbalance Faulty posture can alter the position of joints, causing an increase in stress on different portions of the joint capsule and surrounding ligaments Joint’s capsule and surrounding ligaments undergo adaptive changes from prolonged overstressing or understressing of structure.

16
Structural imbalance Structural Balance refers to the optimal positioning of bones and joints. Structural imbalance is simply when bones and joints are not in their optimal position when weight is applied on them.

17
Faulty posture: Deviates from ideal posture Requires an increased amount of muscular activity Places an increased amount of stress on the joints and surrounding tissues Restrictions in normal movement patterns may cause compensatory postures Overtime can result in muscle imbalances and soft tissue dysfunction

18
Pain related to postural deviations is a common clinical occurrence
Many do not seek help until pain is experienced Postural assessment is used to determine if postural deviations are contributing factors in patient’s pain or dysfunction Posture must be evaluated in functional and nonfunctional positions

19
Postural Syndromes As a result of the muscle imbalances that develop in our musculoskeletal system, postural deviations occur. Janda describes predictable patterns of these postural syndromes. Three typical postural syndromes: Upper Crossed Syndrome Lower Crossed Syndrome Layer Syndrome

20
Upper Crossed Syndrome
Affects the neck-shoulder girdle region Functionally, upper crossed syndrome alters the dynamic stability of the cervical spine Characterized by: Forward head with upper cervical extension and lower cervical flexion Elevation and protraction of the shoulders Winging of the scapula

21
Lower Crossed Syndrome
Affects the lumbopelvic region Characterized by: Anterior pelvic tilt Increased lumbar lordosis Weakness of abdomen muscles Resulting in an increased load placed on the lumbar facet joints (L4-5 and L5-S1)
")
22
Layer Syndrome Chronic postural distortion resulting
from a combination of the upper crossed syndrome and the lower crossed syndrome.

24
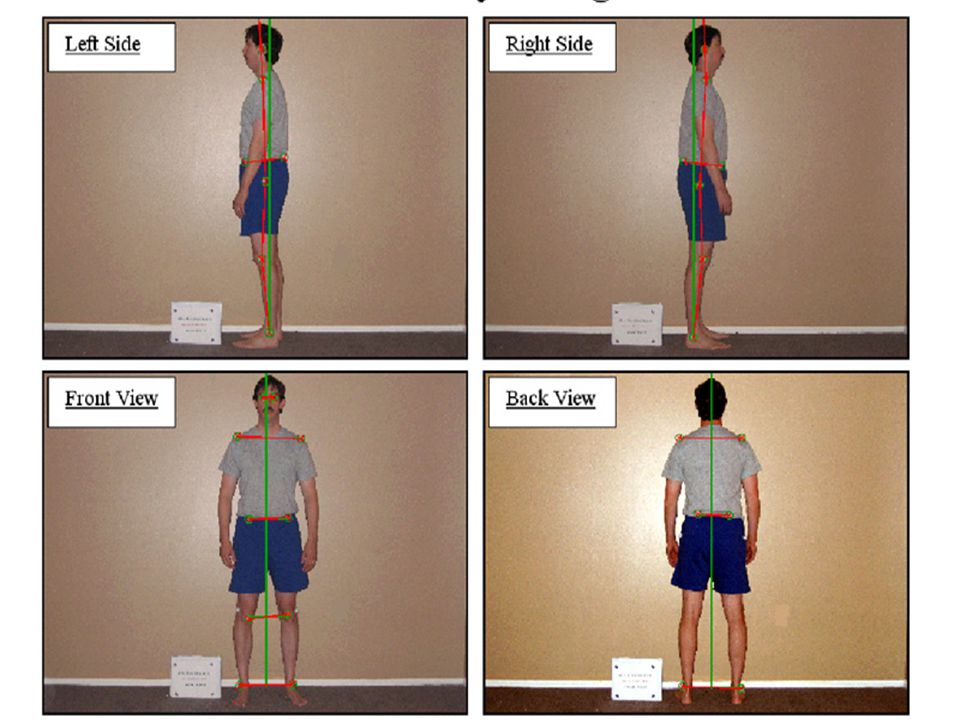
Standard Posture An evaluation of postural faults needs a standard by which individuals postures can be judged. The standing position may be regarded as a reference alignment of a subject from 4 view: Front Back Right side Left side

26
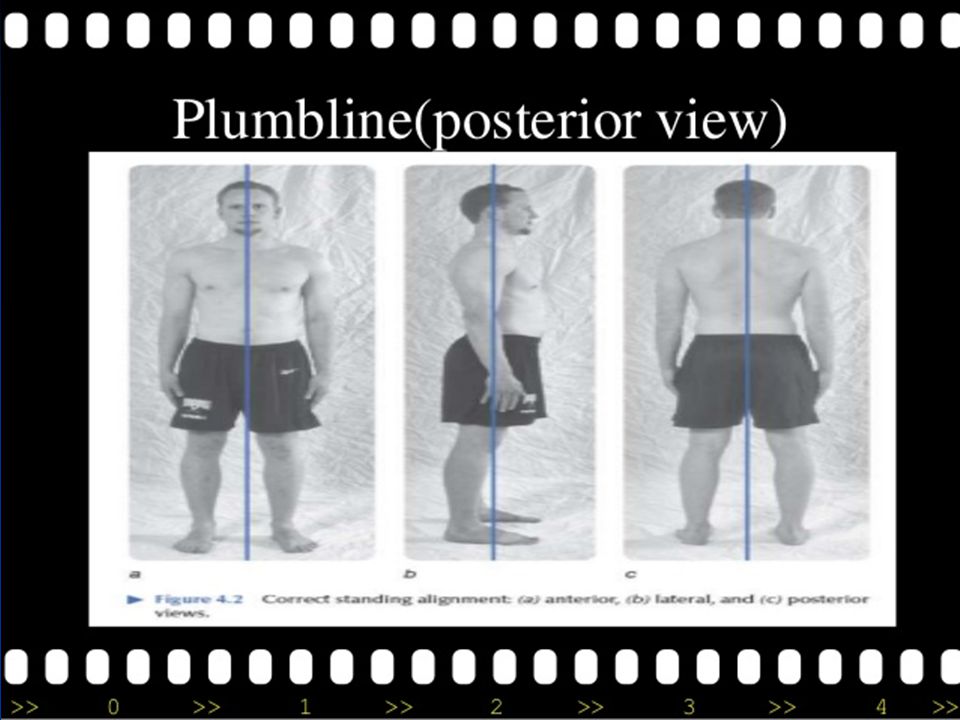
Standard Posture A plumb line is used to determine whether
the points of reference of the body are in the same alignment as standard posture. The amount of deviation of the various point of reference from the plumb line reveal the extend of body malalignment. The amount of deviation from plumb line are described as slight , moderate , sever (marked).
.")
28
Ideal Posture (side view)
Surface landmarks which coincide with the plumb line. Plumb Line is passed: Through lobe of the ear Through shoulder joint ( arms hang in normal alignment beside the trunk ) Midway through the trunk. Through the greater trochanter of femur Slightly anterior to a midline through the knee Slightly anterior to lateral malleolus The Line of reference hypothetically is a projection of the gravity line in the coronal plane, meaning it divides the body into front and back portions of equal weight. The portions are not symmetrical Pelvis is in neutral position: anterior-superior iliac spines and the symphysis pubis are in same vertical planes 28
 Midway through the trunk. Through the greater trochanter of femur. Slightly anterior to a midline through the knee. Slightly anterior to lateral malleolus. The Line of reference hypothetically is a projection of the gravity line in the coronal plane, meaning it divides the body into front and back portions of equal weight. The portions are not symmetrical. Pelvis is in neutral position: anterior-superior iliac spines and the symphysis pubis are in same vertical planes. 28.")
29
Ideal Posture (side view)
Anatomical structures which coincide with the plumb line. Slightly posterior to the apex of coronal suture. Through external auditory meatus . Through the odontoid process of axis. Through the bodies of cervical vertebrae. Through the bodies of lumbar vertebrae . Through the sacral promontory. Slightly posterior to the centre of the hip joint. Slightly anterior to the centre of the knee joint. Through the calcaneo-cuboid joint.

30
Ideal Segmental Alignment : side view
In lateral view , the anterior and posterior muscles attached to pelvis maintain it in ideal alignment. Ant : Abdominal muscles pull pelvis upward. Hip flexors pull downward. Post: Back muscles pull pelvis upward Hip extensors pull downward

31
Head Forward Posture An anterior positioning of the cervical spine is caracteristic of forward head posture. Evaluate neck position (since elevating head too high ) with additional pillows. Very Common (specially in the elderly stage ) Often with dorsal hump
 with additional pillows. Very Common (specially in the elderly stage ) Often with dorsal hump.")
32
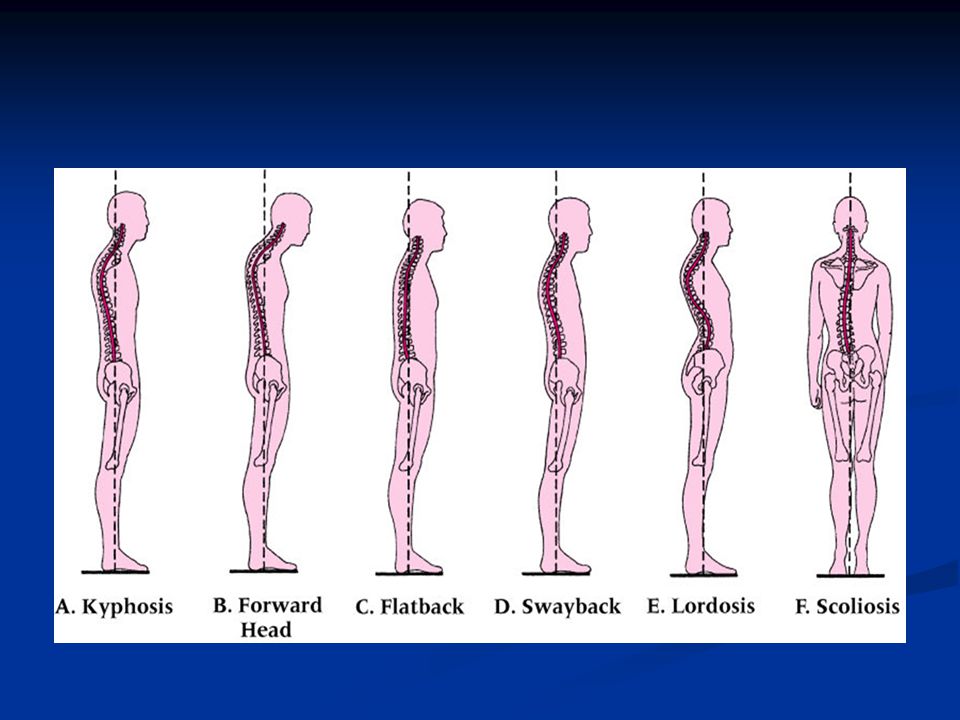
Kyphosis A spine affected by kyphosis shows evidence of a forward curvature of the vertebrae in the upper back area, giving a "humpback" appearance

34
Causes Metabolic problems Neuromuscular conditions
Osteogenesis imperfecta Spina bifida Scheuermann's disease

36
Lordosis Posture Hip flexors , erector spinae are short.
Abdominal, hamstrings, gluteus maximus muscles may be weak. The degree of tilt and lordosis is often associated with marked shortness of iliopsoas.

38
Kyphosis-Lordosis Posture:
This is a common posture where the head is forward and the upper back is excessively rounded.

39
Kyphosis-Lordosis Posture:
The neck flexors (ant. muscles ) are generally weak the neck extensors are short and tight. The muscles in the chest are tightened with forward-rounded shoulders (pectorals) the upper back muscles are lengthened and weak. The pelvis is often rotated forward, with excessive curvature in the lumbar spine. The hip flexors are shortened . The lower abdominal muscle and gluteal muscles are weak and the hamstrings are slightly stretched. -
 are generally weak. the neck extensors are short and tight. The muscles in the chest are tightened with forward-rounded shoulders (pectorals) the upper back muscles are lengthened and weak. The pelvis is often rotated forward, with excessive curvature in the lumbar spine. The hip flexors are shortened . The lower abdominal muscle and gluteal muscles are weak and the hamstrings are slightly stretched. -")
40
Kyphosis- Lordosis Posture:
Head- Forward Cervical Spine- Hyperextended Scapulae – Abducted Thoracic Vertebrate- Increased flexion (Kyphosis ) Lumbar Vertebrate- Hyperextended ( Lordosis ) Pelvis- Anterior tilt (forward and down) Knees- Slightly hyperextended Legs - behind plumb line Ankle - Slightly plantar flexed, This posture can be a result of elongation and weakness neck flexors, muscles that straighten the back, external obliques, and hamstrings. The Neck extensor, hip flexors, and sometimes lower back are stronger.
 Lumbar Vertebrate- Hyperextended ( Lordosis ) Pelvis- Anterior tilt (forward and down) Knees- Slightly hyperextended. Legs - behind plumb line. Ankle - Slightly plantar flexed, This posture can be a result of elongation and weakness neck flexors, muscles that straighten the back, external obliques, and hamstrings. The Neck extensor, hip flexors, and sometimes lower back are stronger.")
41
Kypholordotic Posture
Possible causes: Poor postural sense Muscle imbalance: Tightened/shortened hip flexors Weakened or elongated hip extensors or trunk flexors Adverse effects: Anterior pelvic tilt Hip joint flexion ↑ lumbar lordosis ↑ thoracic kyphosis

42
Military-Type Posture
In military-type posture the back is exaggeratedly straight with the lower back arched, like a soldier standing at attention. A-Moezy

43
Military-Type Posture
Head- Slightly posterior Cervical Spine- Normal curve / slightly anterior Thoracic Vertebrate- Normal curve / slightly posterior Lumbar Vertebrate- Hyperextended ( Lordosis ) Pelvis- Anterior tilt Knees- Slightly hyperextended Ankles - Slightly plantar flexed,
 Pelvis- Anterior tilt. Knees- Slightly hyperextended. Ankles - Slightly plantar flexed,")
44
Sway Back Posture Head: Forward Cervical spine –Slightly extended
Thoracic spine- Increased flexion ( long kyphosis ) with posterior displacement of upper trunk. Lumbar Vertebrate –Increased flexion with flatting of lumbar area curve Pelvis-posterior tilt and anterior to midline Hips- Hyper extended Knees- Hyper extended Ankles – Neutral. A-Moezy A-Moezy
 with posterior displacement of upper trunk. Lumbar Vertebrate –Increased flexion with flatting of lumbar area curve. Pelvis-posterior tilt and anterior to midline. Hips- Hyper extended. Knees- Hyper extended. Ankles – Neutral. A-Moezy. A-Moezy.")
45
Sway Back Posture Anterior hip ligaments – Stretch position
Iliopsoas - Stretch position ( weakness ) External oblique abdominal - Stretch position ( weakness ) Hamestrings – Shortness ( strong) Upper back muscles- Stretch position (weakness ) Upper abdominal muscles - Shortness (strong)
 External oblique abdominal - Stretch position ( weakness ) Hamestrings – Shortness ( strong) Upper back muscles- Stretch position (weakness ) Upper abdominal muscles - Shortness (strong)")
46
Swayback Posture Possible causes:
Ectomorph body: hypomobility of joints Poor postural sense Tightened/shortened hip extensors Weakened or elongated hip flexors or lower abdominals ↓ general muscular strength

47
Swayback Posture Adverse Effects: Genu recurvatum Hip joint extension
Posterior pelvic tilt Lumbar spine in neutral or minimal flexed position ↑ in lower thoracic, thoracolumbar curvature

48
Flat-Back Posture Head- Forward Cervical Spine- Slightly extended
Upper part of Thoracic Spine- Increased flexion Lower part of Thoracic Spine- Straight & reduced curvature Lumbar Spine – straight (flexed) Pelvis- posterior tilt (backward and down) Hips- Extended Knees- Extended Ankle joints- Slightly plantar flexed Can be the result of Weakness and elongation of hip flexors.
 Pelvis- posterior tilt (backward and down) Hips- Extended. Knees- Extended. Ankle joints- Slightly plantar flexed. Can be the result of Weakness and elongation of hip flexors.")
49
Flat-Back Posture Muscle findings in flat back posture are less constant. The most constant finding is a tightness of hamstrings which pulls pelvis into posterior tilt & weakness of hip flexors. Back muscles are in a slightly elongated position and in flexible. Abdominal muscles may / may not be strong.

50
Flat Back Posture

51
Ideal Alignment : Posterior View
Head- Neutral position , not tilted nor rotated. Cervical Spine-Straight. Shoulders – Level, not elevated nor depressed. Scapula - Neutral position ,medial borders parallel & 7.5 – 10 cm (3-4 inches) apart. Thoracic Spine- Straight. Lumbar Spine- Straight.
 apart. Thoracic Spine- Straight. Lumbar Spine- Straight.")
52
Pelvis- Level, PSIS s in the same transverse plane.
Hip joints- Neutral position , neither abd nor add. Knees- Neutral position , neither valgus nor varus. LE – Straight , neither bowed nor knock kneed. Feet – Parallel & slightly toe out. Achilles tendon – Vertical, neither sup. nor pron.

54
Scoliosis Lateral curve in the spine in AP view
AIS is more common among girls and a scoliotic curve is more likely to progress in females than in males. Curves in the thoracic region or curves where the apex is more caudal (closer to the head), are more likely to progress than other types of curves. Curves between 60 to 100 degrees and greater can cause respiratory problems and numerous other health problems. The main goal of treatment of AIS is to prevent progression of the curve magnitude. It is important to monitor AIS especially during puberty 54
, are more likely to progress than other types of curves. Curves between 60 to 100 degrees and greater can cause respiratory problems and numerous other health problems. The main goal of treatment of AIS is to prevent progression of the curve magnitude. It is important to monitor AIS especially during puberty. 54.")
55
Scoliosis Types of Scoliosis:
Congenital (caused by vertebral anomalies present at birth), Idiopathic (cause unknown, sub-classified as infantile, juvenile, adolescent, or adult according to when onset occurred) Neuromuscular ( secondary symptom of another condition, such as spina bifida, cerebral palsy, spinal muscular atrophy or physical trauma).
, Idiopathic (cause unknown, sub-classified as infantile, juvenile, adolescent, or adult according to when onset occurred) Neuromuscular ( secondary symptom of another condition, such as spina bifida, cerebral palsy, spinal muscular atrophy or physical trauma).")
56
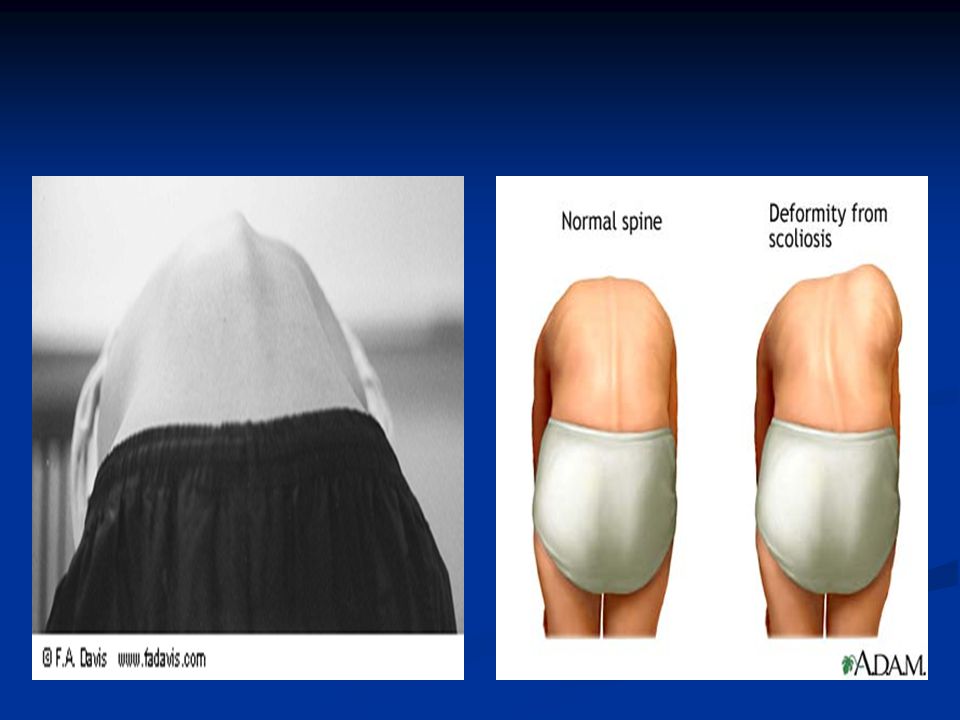
Scoliosis Posture in Scoliosis
Shoulders not level, prominent or uneven scapulas Uneven gap between arm and body Elevated or uneven hip Head not centered Bending test reveals uneven portions of back

57
The common patterns of scoliosis
Thoracic scoliosis. lumbar scoliosis. Thoracolumbar scoliosis. Cervico-Thoracic Scoliosis is depending upon the site of the primary

58
Scoliosis Implications:
Lateral curvature of spinal column Functional: spine attempts to compensate to maintain the head in a neutral position and keep eyes level Muscular imbalance, pelvic obliquity, limb-length discrepancy Structural: defect or congenital bony abnormality of vertebrae Implications: Functional scoliosis: scoliosis present when patient stands straight, disappears during flexion Structural scoliosis: present during both standing and with flexion

59
General Inspection: Scoliosis
Signs and symptoms: Uneven shoulders One shoulder blade appears more prominent Uneven waist / 1 hip higher vs. other Leaning to one side Back pain and difficulty breathing (severe scoliosis) Causes: Idiopathic (85% of cases) Underlying neuromuscular disease, leg-length discrepancy, birth defect, fetal development (congenital) Not caused by poor posture, diet, exercise, or the use of backpacks
 Causes: Idiopathic (85% of cases) Underlying neuromuscular disease, leg-length discrepancy, birth defect, fetal development (congenital) Not caused by poor posture, diet, exercise, or the use of backpacks.")
60
Diagnosis: Angle: X-ray Complications: (severe scoliosis)
Normal Spine (0 degrees) Scoliosis: (> 10 degrees) Complications: (severe scoliosis) Lung and heart damage: compression of rib cage against heart, lungs > 70 degrees Back problems
 Scoliosis: (> 10 degrees) Complications: (severe scoliosis) Lung and heart damage: compression of rib cage against heart, lungs. > 70 degrees. Back problems.")
61
Measure spinal curvature using Cobb method :
Choose the most tilted verterbrae above & below apex of the curve. - Angle b/t intersecting lines drawn perpendicular to the top of the superior vertebrae and bottom of the inferior vertebrae is the Cobb angle.

63
General Inspection: Scoliosis Test: Adam’s Forward Bend Test
Patient Position: Standing with hands held in front (arms straight) Evaluation Procedure: Patient bends forward, sliding hands down the front of each leg Positive Test: Asymmetrical hump along lateral aspect of thoracolumbar spine One shoulder blade appears more prominent Uneven hips
 Evaluation Procedure: Patient bends forward, sliding hands down the front of each leg. Positive Test: Asymmetrical hump along lateral aspect of thoracolumbar spine. One shoulder blade appears more prominent. Uneven hips.")
65
Treatment of scoliosis
In mild cases: Physical Therapy Intervention In moderate cases: Brace treatment & Physical Therapy Intervention In severe cases: Surgical treatment (correction & fusion)
")
66
Brace Treatment for Scoliosis
Most common is Boston brace (aka Thoraco-lumbar-sacral orthosis) Braces have 74% success rate at halting curve progression (while worn) Bracing does not correct scoliosis, but may prevent serious progression Usually worn until patient reaches Risser grade 4 or 5
 Braces have 74% success rate at halting curve progression (while worn) Bracing does not correct scoliosis, but may prevent serious progression. Usually worn until patient reaches Risser grade 4 or 5.")
67
Brace Treatment for Scoliosis
Of patients with 20 º - 29 º curves, only 40% of those wearing braces ultimately required surgery, compared to 68% of those not wearing back braces Length of wearing time correlates with outcome (At least 16 hrs per day leads to best chance of preventing curve progression)
")
68
Pre/ Post Brace Comparison
In Brace X- Ray Pre Brace X-Ray

69
Treatment Guidelines Precautions: Contraindications: Osteoporosis
Post- Surgery Juvenile Hypermobility Syndrome (JHS) Osteogenesis Imperfecta Spondylolisthesis Contraindications: Reactive Scoliosis (tumor, disease, etc) Inflammatory diseases- during active phase Psychiatric Issues
 Osteogenesis Imperfecta. Spondylolisthesis. Contraindications: Reactive Scoliosis (tumor, disease, etc) Inflammatory diseases- during active phase. Psychiatric Issues.")
70
Exercises An effective regimen of exercises for scoliosis must follow careful diagnosis of which muscle groups in a patient's body are too weak, and which are overdeveloped and tight. Then the therapist designs a program to restore normal balance. Each person's scoliosis deformity is somewhat unique, so a therapist tailors the scoliosis exercises individually

71
They are shortened (blue), less elastic and less freely movable compared to the other side, which are lengthened (red). Deformation of the skeleton causing nerves to become trapped and eventually causing pain

72
The regimen of muscle-strengthening and stretching exercises aims to derotate and elongate the spine back into its normal position. The patient must do the scoliosis exercises for about 1/2 hour daily. Patient compliance is extremely important, and it's hard work The Schroth method gives a patient the knowledge and tools to control her or his own postural health, lifelong

74
Schroth scoliosis exercises
The goal of Schroth scoliosis exercises is to practice moving the body out of its unbalanced state past the longitudinal axis towards the opposite side, until the brain is correctly reprogrammed and the patient is able to sit and stand straight upright..

75
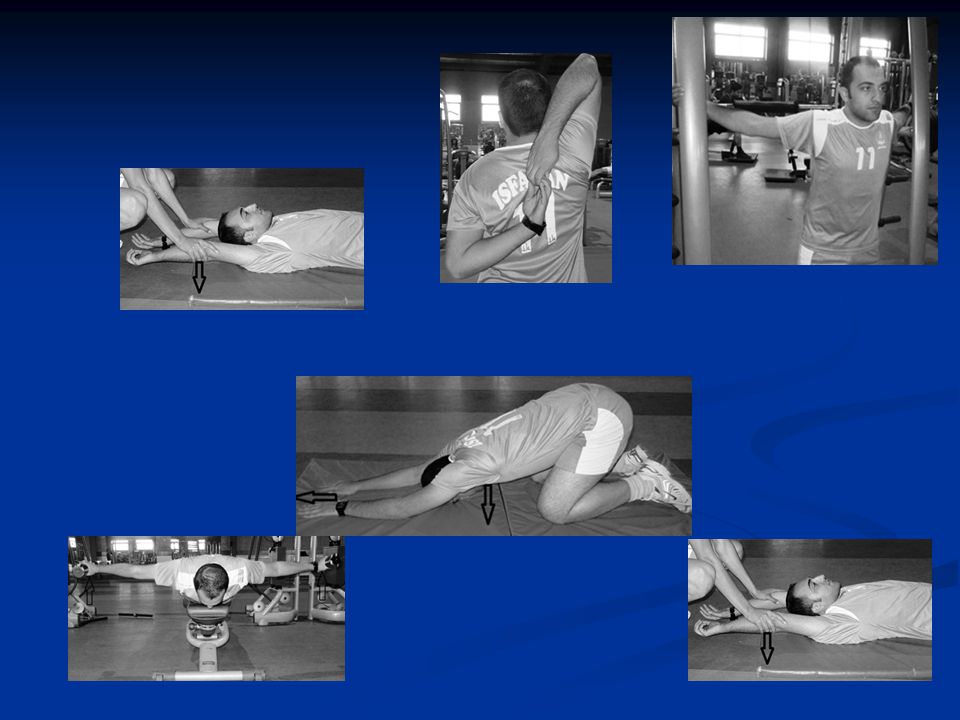
Semi-Hanging Sagittal Plane
Schroth Exercises Semi-Hanging Sagittal Plane Prone on Knees-Transverse Plane Anterior Gravity Assisted

76
Schroth Exercise Supine Gravity Assisted- Transverse Plane
Standing 3D Correction Supine Gravity Assisted- Transverse Plane

77
Sagittal Plane Correction
Visit 1 Visit 3 Important to Sagittal Plane Correction first, then Elongation followed Translation moving Rside Thorax to the Left and Deflection. Notice Pre- Post the head is balanced over the thorax, the shoulders are back, the abdominals can now engage do to the decrease in excessive lordosis.

78
Exercises Using Schroth Principles
Traction with AutoCorrection and Elongation- Seated in Corrected Posture

79
Exercises Using Schroth Principles
Visit 1 - Uncorrected Visit 3 - Corrected Posture Standing AutoCorrection with Elongation and Deflection- Doing Standing Breathe Work

80
Exercises – Sport Specific and In-Brace
Long Hang Tx, opposite of curve- Elite Gymnast Standing AutoCorrection –In Brace with RSC

81
Sport Specific Training In Corrected Posture
Right Thoracic Left Lumbar non –corrected. Doing Sport Specific Training in Over Correction – For Bball and Softball

82
Visit 2 Sagittal Plane Correction
Sagittal Correction Psoas Stretch

83
Stretching- Stabilization
Supine Hamstring Stretch Scapular / Core Stability

85
Sagittal Correction Visit 1 Visit month follow up

86
Surgical Treatment for Scoliosis
Curves in growing children greater than 40 º require a spinal fusion (Risser grade 0 to 1 in girls and Risser 2 or 3 in boys) Skeletally mature patients can be observed until their curves reach 50 º Posterior spinal fusion is best choice for thoracic curves Anterior spinal fusion is best treatment for thoracolumbar and lumbar curves
 Skeletally mature patients can be observed until their curves reach 50 º. Posterior spinal fusion is best choice for thoracic curves. Anterior spinal fusion is best treatment for thoracolumbar and lumbar curves.")
87
Thank you

Similar presentations