Download presentation
Presentation is loading. Please wait.

1
BIOE 301 Lecture Three

2
Review of Lecture Two Developing world Developed world
Perinatal conditions Lower respiratory infections Diarrheal diseases Malaria Developed world Congenital anomalies Unintentional injuries

3
Leading Causes of Mortality Ages 15-44
Developing World HIV/AIDS Unintentional injuries Cardiovascular diseases Tuberculosis Developed World Cancer Self-inflicted injuries

4
Burden of HIV/AIDS Worldwide
40 million people are living with HIV/AIDS 20 million people have been killed by the disease 2003: 3 million deaths 5 million new HIV infections 2/3 of those with AIDS are in Africa 1 in 12 African adults has HIV/ AIDS

5
AIDS has Reduced Life Expectancy

6
Burden of HIV/AIDS United States
million people have HIV/AIDS (prevalence) 30,000-40,000 new HIV infections per year (incidence) Annual cost to treat: $15 billion
 30,000-40,000 new HIV infections per year (incidence) Annual cost to treat: $15 billion.")
7
Clinical Course of HIV/AIDS
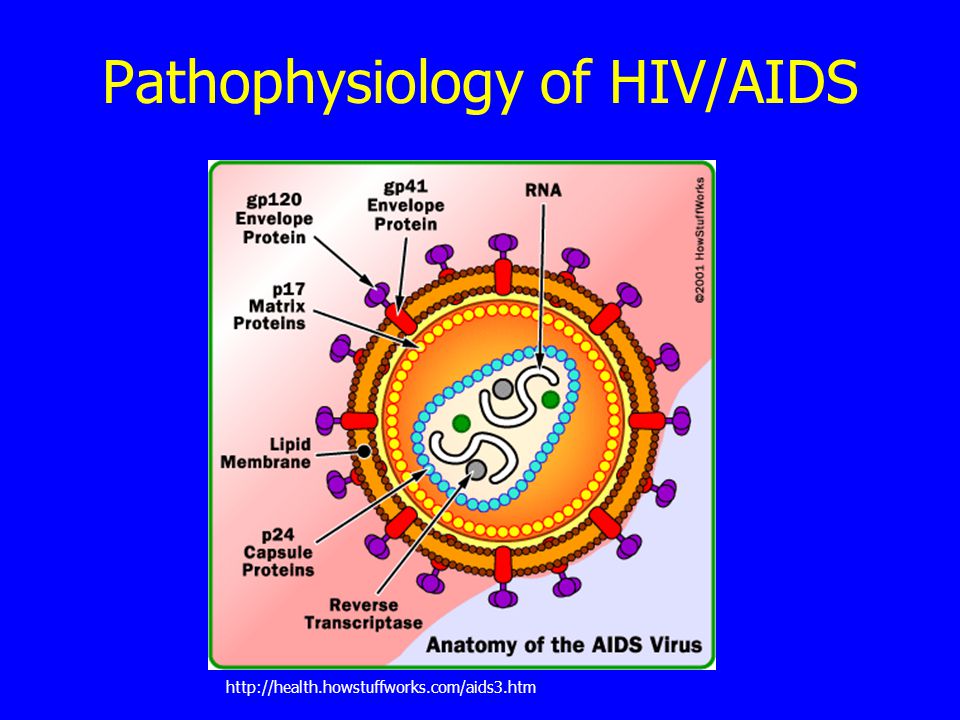
HIV Infection Spread by sexual contact with infected person or sharing needles with infected person or by transmission from mother to child Virus deposited on mucosal surface Acute infection (flu like symptoms) Viral dissemination HIV-specific immune response Replication of virus Destruction of CD4+ lymphocytes Rate of progression is correlated with viral load Latent Period
 Viral dissemination. HIV-specific immune response. Replication of virus. Destruction of CD4+ lymphocytes. Rate of progression is correlated with viral load. Latent Period.")
8
Clinical Course of HIV/AIDS

9
Clinical Course of HIV/AIDS
Immunologic dysregulation Opportunistic infections and cancers Risk of infections is correlated with number of CD4+ lymphocytes Average patient with AIDS dies in 1-3 years Within 10 years of infection (w/o Rx): 50% of patients develop AIDS 40% develop illness associated with HIV 5-10% remain asymptomatic
: 50% of patients develop AIDS. 40% develop illness associated with HIV. 5-10% remain asymptomatic.")
10
HIV/AIDS Historical Perspective
1981 CDC reported unexplained PCP in 5 previously health, homosexual men CDC reported Kaposi’s sarcoma in 26 previously healthy, homosexual men Increased association with IV drug use, recipients of blood transfusions, hemophiliacs 1983 Virus isolated

11
HIV/AIDS Historical Perspective
1984 Virus shown to be causative agent 1985 ELISA test developed 1996: HAART developed Today: Broad spectrum of disease Asymptomatic infection Clinical latency Advanced disease (AIDS) Clearly sexually transmitted, and transmitted through blood products
 Clearly sexually transmitted, and transmitted through blood products.")
12
Pathophysiology of HIV/AIDS
13
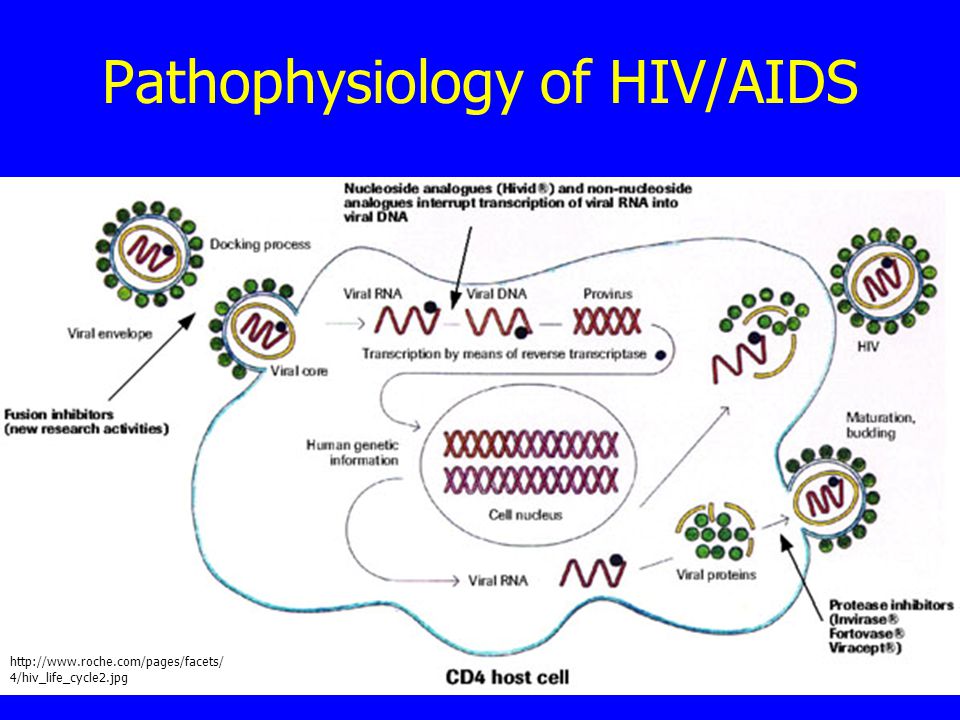
Pathophysiology of HIV/AIDS
14
HAART Treatments for HIV/AIDS
Inhibit reverse transcriptase enzymes (1987) Enzyme is specific to HIV Combinations of RTIs appear effective Inhibitors of HIV protease (1995) HIV proteases are distinct from mammalian proteases Most significant advance in HIV therapy yet Highly Active Antiretroviral Therapy (HAART) Combination of three or more drugs Fusion inhibitors (2003) Subject of new research
 Enzyme is specific to HIV. Combinations of RTIs appear effective. Inhibitors of HIV protease (1995) HIV proteases are distinct from mammalian proteases. Most significant advance in HIV therapy yet. Highly Active Antiretroviral Therapy (HAART) Combination of three or more drugs. Fusion inhibitors (2003) Subject of new research.")
15
HAART HIV can rapidly mutate to quickly develop resistance to a single drug Resistance develops much more slowly to drug combinations Goal of HAART: Reduce viral levels to undetectable levels Has reduced death rate in US and Europe by 80%

17
Unintentional Injuries
More than 1.25 million people aged die as a result of unintentional injuries each year Major cause of disability Leading cause is road traffic injuries: 500,000 deaths per year in his age group 90% of these deaths occur in developing countries

18
US Burden of Disease: Road Accidents
Rates declining steadily Leading cause of potential years of life lost 2004: 42,636 Americans killed 2,788,000 Americans injured Fatal accident rates >4X higher for males than for females Motorcycles: 40X higher death rate per mile traveled 39% of fatalities related to alcohol use

19
Prevention: Road Accidents
Legislation: Speed Seat belts, Car seats, Air Bags Alcohol use Motorcycle helmets Engineering: Restraints Safety standards Education:

20
Accident Physics Newton’s 2nd Law: In a crash:
F = m a a = dv/dt a = initial velocity/time to come to rest In a crash: Velocity slows to zero in a very short time Generates large forces How can we reduce these forces? Reduce initial velocity of impact Extend time that it takes passengers to come to rest

21
Reducing Initial Velocity
Excessive speed contributes to: 30% of deaths in developed countries 50% of deaths in developing countries

22
Physics of Accidents/Restraints

23
Slowed Driver Reaction Time
When drivers anticipate a crash, they have time to brake and reduce initial velocity Factors which slow driver reaction time: Alcohol use Cell phone use Poor visibility

24
Alcohol Use Alcohol impaired drivers have 17X increased risk of being in fatal crash Alcohol use increases risk more in younger drivers

25
Mobile Phone Use At any given daylight moment in US: Cell phone use:
10% of drivers are using a cell phone Cell phone use: Increases driver reaction time by sections Risk of crash is 4X higher when using a mobile phone Same as driving with a BAC of 0.09 g/ dl 3 states have banned use of hand held phones while driving

26
Alcohol Related Deaths

27
Extending Time to Come to Rest
Crumple zones Allow passengers additional time to decelerate Seat belts Keep occupants in the passenger compartment Stretch during impact Reduce risk of death in crash by 40-60% Air bags When combined with seat belts, reduce risk of serious and fatal injuries by 40-65% Child restraints: Reduce risk of infant death by 71% and toddler death by 54$

28
Helmet Laws

29
Cardiovascular Diseases
768,000 people aged die as a result of cardiovascular disease every Most common causes: Ischemic heart disease (286,000 deaths) Cerebrovascular disease (159,000 deaths)
 Cerebrovascular disease (159,000 deaths)")
30
Ischemic Heart Disease: Epidemiology
United States 11 million people have coronary artery disease Causes more deaths, disability and economic cost than any other illness Risk factors Positive family history Diabetes Hyperlipidemia Hypertension Smoking

31
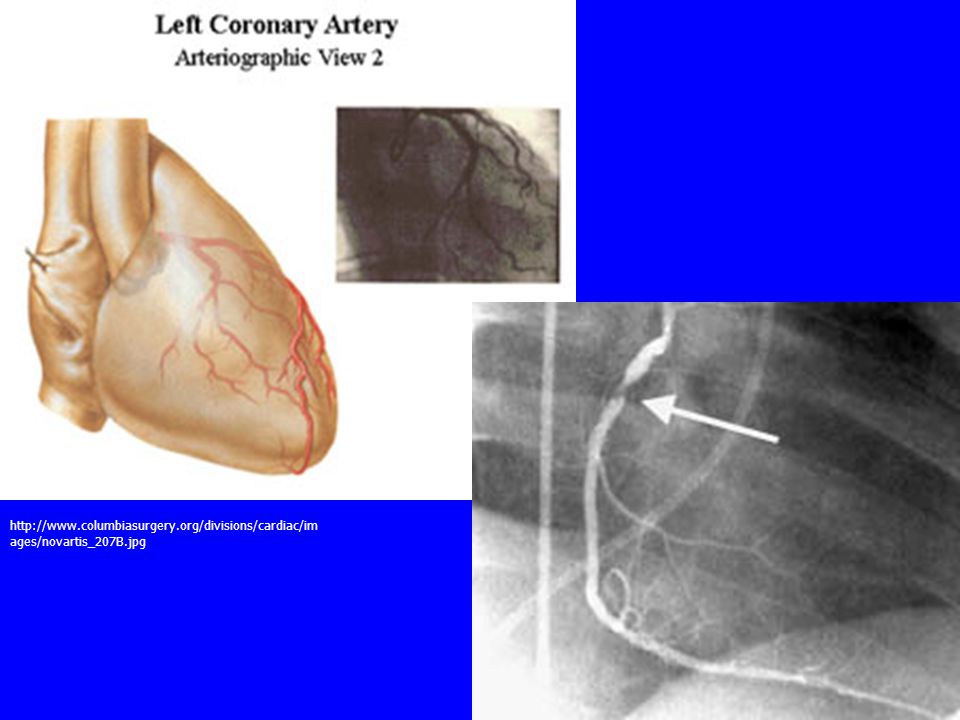
Ischemic Heart Disease: Pathogenesis
Atherosclerosis Causes a decrease in myocardial perfusion Stable angina Typically a yo man or yo woman Heaviness, pressure, squeezing, smothering or choking Localized to chest Lasts 1-5 minutes Radiates to left shoulder and both arms Unstable angina Patients with angina that is: New onset and severe and frequent Accelerating Angina at rest

33
Ischemic Heart Disease: Diagnosis
Usually made by history Physical exam may reveal other disorders Lipid disorders Hypertension Diabetes Testing EKG Stress Testing Coronary arteriography

35
Ischemic Heart Disease: Treatment
Medical management Nitrates Increase myocardial oxygen supply, systemic vasodilation Beta blockers Inhibit increases in heart rate and contractility Decrease myocardial oxygen demand Calcium channel agonists Coronary vasodilators CABG PTCA

36
CABG PTCA

37
Cerebrovascular Disease: Epidemiology
Third leading cause of death in the US Most prevalent neurologic disorder Morbidity Mortality

38
Cerebrovascular Disease: Stroke
Abrupt onset with focal neurologic deficit Usually mini-event or warning signs 5-20% transient ischemic attacks Reversible ischemia Some lasting hours Completed stroke Maximal deficit within hours Often patient awakens with completed stroke Usually preceded by TIA Progressive stroke Ischemia worsens min. to min. or hour to hour

39
Cerebrovascular Disease: Pathogenesis
Causes of stroke: Blood vessel supplying the brain is blocked Thrombosis (clot in vessel) Embolism (clot breaks off and lodges in blood vessel in brain) Vasoconstriction or spasm Venous collapse
 Embolism (clot breaks off and lodges in blood vessel in brain) Vasoconstriction or spasm. Venous collapse.")
40
Cerebrovascular Disease: Diagnosis
History Exam Imaging CT Scan MRI CT/MR Angiography

41
Cerebrovascular Disease: Treatment
Thrombolysis Rehabilitation Experimental Angioplasty Heparin Coumarin Aspirin

42
Tuberculosis 600,000 people ages 15-44 die each year from TB 2003:
8.8 million new cases Growing 1%/year 1.5 million deaths 98% of deaths occur in developing world Estimated that TB will kill 35 million people in next 20 years if situation does not change

43
Tuberculosis Bacterial infection of the lungs caused by mycobacterium tuberculosis Drugs which cure TB were discovered in 1940s If untreated, results in death in 5 years in half of all cases

45
Tuberculosis 1/3 of world’s population is infected with TB
Not all have active TB Most have latent TB - Immune system has walled off bacilli with waxy coat 5-10% of people with normal immune systems will go on to develop active TB Higher in people with compromised immune systems (10X higher in people with AIDS) TB is leading cause of death among people with HIV/AIDS
 TB is leading cause of death among people with HIV/AIDS. wfId=")
46
Tuberculosis Symptoms Airborne transmission
Fever Night sweats Weight loss Weakness Coughs (productive with bloody sputum) Airborne transmission Left untreated, one person with active TB can infect people each year
 Airborne transmission. Left untreated, one person with active TB can infect people each year.")
47
Tuberculosis: Diagnosis
Skin test Serum test CXR Shows nodules in active TB

48
Tuberculosis: Treatment
Latent TB: Treated with isoniazid, prevents development of active TB Active TB: Can almost always be cured by taking several antibiotics in combination Stay home for several weeks while contagious Take drugs for 6 months

49
Tuberculosis Resistant TB:
Can develop if patients do not take all medicine Growing problem 425,000 new cases per year In Russia and China, 14% of new cases are resistant Must be treated with special medicines Poorly supervised Rx is worse than no Rx DOTS: 6 month supply is $10 Cure rates of up to 95% even in poorest countries 17 million patients worldwide have been treated with DOTS since 1995 25% of world’s population does not have access to DOTS.

50
Cancer 580,000 people aged 15-44 die every year due to cancer
Cancer is a group of diseases characterized by uncontrolled cell growth Cancer cells usually form a tumor Cancer cells can spread from tumor to other sites in the body

51
Cancer 2nd leading cause of death in US
1 of every 4 deaths is from cancer 5-year survival rate: 59% Annual costs: $107 billion

52
Cancer Tumor Types of Tumors:
Abnormal mass of tissue Growth exceeds that of normal tissue Purposeless and preys on host Types of Tumors: Benign Malignant Only malignant tumors can spread (Metastasize)
")
53
Microscopic Appearance

54
2004 Estimated US Cancer Deaths*
Men 290,890 Women 272,810 Lung & bronchus 32% Prostate 10% Colon & rectum 10% Pancreas 5% Leukemia 5% Non-Hodgkin 4% lymphoma Esophagus 4% Liver & intrahepatic 3% bile duct Urinary bladder 3% Kidney 3% All other sites 21% 25% Lung & bronchus 15% Breast 10% Colon & rectum 6% Ovary 6% Pancreas 4% Leukemia 3% Non-Hodgkin lymphoma 3% Uterine corpus 2% Multiple myeloma 2% Brain/ONS 24% All other sites Lung cancer is, by far, the most common fatal cancer in men (32%), followed by prostate (10%), and colon & rectum (10%). In women, lung (25%), breast (15%), and colon & rectum (10%) are the leading sites of cancer death. ONS=Other nervous system. Source: American Cancer Society, 2004.
, followed by prostate (10%), and colon & rectum (10%). In women, lung (25%), breast (15%), and colon & rectum (10%) are the leading sites of cancer death. ONS=Other nervous system. Source: American Cancer Society,")
55
Differentiation and Anaplasia
Benign tumors Well differentiated Malignant tumors Range from well to poorly differentiated Hallmarks of anaplasia: Cells and nuclei show pleomorphism Cells contain abundant DNA, coarse, clumped chromatin Large NC ratio (1:1) rather than (1:4) Large nucleoli Large # of mitoses Dysplasia Precancerous condition in epithelial tissue Anaplastic cells in epithelium Dysplasia does not always progress to cancer
 rather than (1:4) Large nucleoli. Large # of mitoses. Dysplasia. Precancerous condition in epithelial tissue. Anaplastic cells in epithelium. Dysplasia does not always progress to cancer.")
56
Carcinogensis Carcinogenesis: Result of non-lethal genetic damage
Tumor masses result from the clonal expansion of a single progenitor cell that has incurred genetic damage

57
Biology of Tumor Growth
Natural hx of most cancers has 4 phases: Malignant transformation in target cell Growth of transformed cells Local invasion Distant metastases

58
Fig 7.33 – The Metastatic cascade Neoplasia

59
Tissue Invasion Metastasis causes 90% of cancer death
How do tumors invade: Detach from primary tumor Degrade surrounding matrix Migrate

60
Importance of Cancer Screening

61
Burden of Self-Inflicted Injuries
480,000 people aged take their own lives each year Highest rate of completed suicides Men >65 years old Highest rate of attempted suicides Men and women ages 20-24

62
Risk Factors Associated with Suicide
Psychiatric illness Affective, substance abuse, personality, other mental disorders Other risk factors Social adjustment problems Serious medical illness Living alone Recent bereavement Personal history of suicide attempt or completion Divorce or separation Unemployment

63
Methods of Suicide Most common: 2nd leading cause:
Firearms are used in 60% of suicides 2nd leading cause: Men: Hanging Women: Drug overdose or poison Alcohol is involved in 25-40% of suicides

64
Screening and Prevention
50-66% of all suicide victims visit physician <1 month before event 10-40% in the preceding week Hard to identify who is at risk Direct questioning has low yield General questions about sleep disturbance, depressed mood, guilt and hopelessness Survey instruments aren’t good at predicting what will happen

65
Screening for Suicide Risk
How do we quantify the efficacy of such questionnaires? Goal of screening: Catch as many positives as possible, even at the risk of some false positives Sensitivity: Se = probability of testing positive if you will commit suicide Sensitivity of best questionnaires: 56% (low)
")
66
Screening for Suicide Risk
How many false positives result? Positive predictive value: PPV=probability of committing suicide if you test positive PPV of best questionnaires: 3% (pathetic)
")
67
Summary of Lecture Two Developing countries
Leading causes of mortality: ages 15-44 Developing world HIV/AIDS Road Accidents Interpersonal violence Developed world Road accidents Self-inflicted injuries

68
Summary of Lecture 3 Developing World Developed World HIV/AIDS
Unintentional injuries Cardiovascular diseases Tuberculosis Developed World Cancer Self-inflicted injuries

69
Assignments Due Next Time
HW3

70
Malaria and Tuberculosis
Infectious Diseases Malaria and Tuberculosis

71
What is Malaria? Periodic episodes of severe chills and high fevers along with profuse sweating at hour intervals, anemia. Plasmodium, a protozoa P. falciparum – Coma and death P. malarium P. ovali and vivax – latent stage in the liver Deaths in children <5 y/o in sub-Saharan Africa Infection does not necessarily cause symptoms Explain the diagram. Start with mosquito. Enters liver, grow and spread to the human RBCs, where they reproduce. The red cells fill with protozoa and burst. The red cells all burst at the same time, releasing the protozoa into the bloodstream and exposing them to the immune system, which results in fever. Bullet one. Bullet two. Bullet three. Bullet four – implications for treatment. *** Protozoa is a subkingdom of the animal kingdom, includes all of the so-called acellular or unicellular forms. They consist of a single functional cell unit or aggregation of nondifferentiated cells, loosely held together and not forming tissues. After a single sporozoite (the parasite form inoculated by the female mosquito) of Plasmodium falciparum invades a liver cell, the parasite grows in 6 days and produces 30,000-40,000 daughter cells (merozoites) which are released into the blood when the liver cell ruptures. In the blood, after a single merozoite invades a red blood cell, the parasite grows in 48 hours and produces 8-24 daughter cells, which are released into the blood when the red blood cell ruptures. Vector – invertebrate capable of transferring an infectious agent to vertebrates
 of Plasmodium falciparum invades a liver cell, the parasite grows in 6 days and produces 30,000-40,000 daughter cells (merozoites) which are released into the blood when the liver cell ruptures. In the blood, after a single merozoite invades a red blood cell, the parasite grows in 48 hours and produces 8-24 daughter cells, which are released into the blood when the red blood cell ruptures. Vector – invertebrate capable of transferring an infectious agent to vertebrates.")
72
Malaria is a disease of the tropics
Title. Sub-Saharan Africa has highest incidence of falciparum. What impact does malaria have on a community or country? Source: CDC

73
Impact of Malaria Enormous economic burden
Direct costs Drugs, doctors’ fees, lost wages, insecticide treated mosquito nets Indirect costs Pain and suffering, hampered schooling Reduced tourism and business investments “Growth penalty” of 1.3% per year Disease of poverty and a cause of poverty Malaria has a sign economic impact. Bullets. Growth penalty, when compounded, is sign. How do we control malaria? *** Direct cost – incurred by a particular job or operation, such as utilities, management salaries, material handling, data processing Indirect - Costs that are not incurred by a particular job or operation, such as utilities, management salaries, material handling, data processing

74
How Do We Control Malaria?
Prevent mosquito bite Eliminate vector (Anopheles mosquito) with pesticides at dusk in living and sleeping areas Use insect repellants and mosquito nets, and wear long-sleeved shirts and long pants Expensive Treat those will malaria Treatment prevents spread of disease Not all infected have symptoms Treatment depends on species and strain How? 2 ways, prevent mosquito bites and treat malaria. Bullets. As mentioned, ITNs. Solutions? Dip-it-yourself Encourage the development of commercial markets (large scall promotion activities, tax and tariff reforms) Voucher schemes Social marketing to raise awareness of the value of ITNs Treat. bullets Insecticide-treated mosquito net
 with pesticides at dusk in living and sleeping areas. Use insect repellants and mosquito nets, and wear long-sleeved shirts and long pants. Expensive. Treat those will malaria. Treatment prevents spread of disease. Not all infected have symptoms. Treatment depends on species and strain. How 2 ways, prevent mosquito bites and treat malaria. Bullets. As mentioned, ITNs. Solutions Dip-it-yourself. Encourage the development of commercial markets (large scall promotion activities, tax and tariff reforms) Voucher schemes. Social marketing to raise awareness of the value of ITNs. Treat. bullets. Insecticide-treated mosquito net.")
75
Who pays for treatment and control?
Local governments, Non-profits, governments of developed countries Private sector Supporting malaria control helps boost profit Quick. Bullets.

76
What is the role of technology?
Develop a vaccine Better diagnostic techniques Low cost, rapid, user-friendly (e.g. dipstick test) Pre-packaging drugs Mapping of the Plasmodium falciparum genome -> better drugs Mapping malaria vectors Bullets Analysis of distribution and abundance of malaria vectors using GIS and GPS
 Pre-packaging drugs. Mapping of the Plasmodium falciparum genome -> better drugs. Mapping malaria vectors. Bullets. Analysis of distribution and abundance of malaria vectors using GIS and GPS.")
77
Who pays for technology development?
US Govt gives tax credits for companies that develop new vaccines World Bank may create a revolving fund to subsidize purchase of new vaccines Roll Back Malaria WHO-founded global partnership Roll Back Malaria is another WHO-founded global partnership with a goal of cutting the world’s malaria burden in half by With a shorter treatment period, effective prevention technology and recent successes in fighting malaria in affected countries, this effort may have the best chance among the large-scale disease initiatives for hitting its marks. Demonstrating success in rolling back malaria on a global scale is seen to be crucial for demonstrating that similar large partnerships for TB and HIV are feasible.

78
Disease Burden and Funding
R&D funding per disability-adjusted life year, if you recall from lecture 2 is a measure of healthy life lost, a combined index of morbidity and mortality. Notice that malaria is remarkably underfunded. Perhaps too much funding goes to Diabetes R&D. SOURCE: MALARIA R&D ALLIANCE

79
Where is the malaria vaccine?
What is stopping us? Funding Thousands of antigens to the human immune system -> which ones are useful targets? Plasmodium has several life stages -> different antigens at each stage Plasmodium has several strategies to confuse, hide, and misdirect human immune system Multiple malaria infections of the different species and different strains of the same species in one host! Explain points

80
Tuberculosis Bacterial infection of the lungs and occasionally other body parts caused by Mycobacterium tuberculosis Incidence: 7.5 million people (WHO) Deaths: 2.5 million people/year. TB infects one-third of all humans. Follow poverty and urban crowding Particularly severe in: AIDS patients Those who can't afford medical care Noncompliant patients. Once upon a time, tuberculosis -- a bacterial infection of the lungs and occasionally other body parts -- was highly responsive to antibiotics. No longer. TB remains a global menace, afflicting 7.5 million people, according to the World Health Organization, and killing as many as 2.5 million people each year. That makes it the leading cause of death among infectious diseases. TB is particularly severe in AIDS patients, those who can't afford medical care, and patients who disobey doctors. According to the WHO, the pathogen infects one-third of all humans. Tuberculosis is a contagious respiratory infection that follows poverty and urban crowding, infecting 30 million each year and killing 5,000 people every day. Worldwide, TB is the leading killer of people with HIV, and the course of both HIV and TB is much more rapid and deadly in persons with both infections. In Africa, half of all TB cases are associated with HIV, and although relatively rare in the U.S. due to robust prevention and treatment efforts, 10 to 20 percent of TB cases are associated with HIV. Slides of TB pathogen, mycobacterium, a thin rod-shaped organism with high lipid content in the cell walls, making it acid-fast on staining. Primary is subclinical lung inf. Secondary is pulmonary and other organs. Perhaps most ominous, some strains of the disease-causing organism, Mycobacterium tuberculosis, have become resistant to a series of antibiotics. So now just having enough money to buy antibiotics no longer guarantees a cure.
 Deaths: 2.5 million people/year. TB infects one-third of all humans. Follow poverty and urban crowding. Particularly severe in: AIDS patients. Those who can t afford medical care. Noncompliant patients. Once upon a time, tuberculosis -- a bacterial infection of the lungs and occasionally other body parts -- was highly responsive to antibiotics. No longer. TB remains a global menace, afflicting 7.5 million people, according to the World Health Organization, and killing as many as 2.5 million people each year. That makes it the leading cause of death among infectious diseases. TB is particularly severe in AIDS patients, those who can t afford medical care, and patients who disobey doctors. According to the WHO, the pathogen infects one-third of all humans. Tuberculosis is a contagious respiratory infection that follows poverty and urban crowding, infecting 30 million each year and killing 5,000 people every day. Worldwide, TB is the leading killer of people with HIV, and the course of both HIV and TB is much more rapid and deadly in persons with both infections. In Africa, half of all TB cases are associated with HIV, and although relatively rare in the U.S. due to robust prevention and treatment efforts, 10 to 20 percent of TB cases are associated with HIV. Slides of TB pathogen, mycobacterium, a thin rod-shaped organism with high lipid content in the cell walls, making it acid-fast on staining. Primary is subclinical lung inf. Secondary is pulmonary and other organs. Perhaps most ominous, some strains of the disease-causing organism, Mycobacterium tuberculosis, have become resistant to a series of antibiotics. So now just having enough money to buy antibiotics no longer guarantees a cure.")
81
Stages of Tuberculosis Illness
Primary TB Latent TB Secondary, or reactivation, TB

83
Stop TB Partnership Goal: Reduce the global burden of the disease by half by the year 2010. How: A broad commitment from governments and NGOs. Stop TB Partnership, a global association of all organizations and individuals working to control and eliminate TB in the world.

84
What is the role of technology?
Vaccine development and evaluation Early diagnosis and monitoring Drug-sensitive v. drug-resistant strains of TB Epidemiology New molecular tools Drug development and treatment Mechanisms of drug resistance and activity Discovery and development of new candidate antibiotics Basic Research Molecular biology, genetics, immunology and pathogenic mechanisms of TB Read bullets. ***** Epidemiology is the investigation of factors that determine the frequency and distribution of disease or other health-related conditions within a defined human population during a specified period. Basic Research: Encourage, and give priority to, meritorious investigator-initiated research directed toward improved understanding of basic and molecular biology, genetics, immunology and pathogenic mechanisms of M. tuberculosis (TB). Provide research materials to qualified investigators to encourage and enable basic research in TB. Vaccine development and evaluation: Support basic and clinical research leading to the development and testing of an effective new vaccine(s) for the prevention and control of TB. Diagnosis: Support the development of improved diagnostic tools for early diagnosis and monitoring of infection and disease, due to drug-sensitive and drug-resistant strains of M. tuberculosis. Epidemiology: Support research, including the development of new molecular tools, to assess the factors influencing the occurrence, distribution, and transmission of TB and multidrug-resistant TB. Animal models: Support research to improve animal models of TB for use in the study of virulence and pathogenic mechanisms and for the evaluation of TB therapies and candidate vaccines. Provide facilities and resources for screening anti-TB vaccine candidates in appropriate animal models. Drug development and treatment: Support research on mechanisms of drug resistance and activity, discovery and development of new candidate antibiotics, and clinical testing of prophylactic and therapeutic anti-TB regimens and evaluate and improve the effectiveness of treatment, especially against multi-drug resistant tuberculosis.
. Provide research materials to qualified investigators to encourage and enable basic research in TB. Vaccine development and evaluation: Support basic and clinical research leading to the development and testing of an effective new vaccine(s) for the prevention and control of TB. Diagnosis: Support the development of improved diagnostic tools for early diagnosis and monitoring of infection and disease, due to drug-sensitive and drug-resistant strains of M. tuberculosis. Epidemiology: Support research, including the development of new molecular tools, to assess the factors influencing the occurrence, distribution, and transmission of TB and multidrug-resistant TB. Animal models: Support research to improve animal models of TB for use in the study of virulence and pathogenic mechanisms and for the evaluation of TB therapies and candidate vaccines. Provide facilities and resources for screening anti-TB vaccine candidates in appropriate animal models. Drug development and treatment: Support research on mechanisms of drug resistance and activity, discovery and development of new candidate antibiotics, and clinical testing of prophylactic and therapeutic anti-TB regimens and evaluate and improve the effectiveness of treatment, especially against multi-drug resistant tuberculosis.")
85
Overlapping Epidemics
Malaria and HIV For people with HIV, especially pregnant women, episodes of acute malaria are complicated and more serious. TB and HIV TB is the leading killer of people with HIV In Africa, half of all TB cases are associated with HIV. Collectively, HIV, TB, and malaria may be responsible for over six million deaths per year, with many more trailing in their wake as the burden on economies and health care capacity becomes overwhelming. Indeed, there are opportunities to be mined in these overlapping epidemics. Increasingly, the fear that destabilized societies and economies may impact the security of Western nations has stimulated a great deal of rhetoric and an increasing amount of money dedicated to addressing the burden of disease in the world. Hopefully, several emerging global partnerships will be able to direct a coordinated and effective response to these threats as the promised resources become available. Indeed, there are opportunities to be mined in these overlapping epidemics. Infrastructure in place to deliver TB treatment has been proposed as a platform on which to build a network to provide antiretroviral therapy. The high rate of antenatal clinic attendance in some parts of Africa gives an opportunity to detect HIV and sexually transmitted diseases, forestalling transmission to infants and preventing complications due to malaria. Malaria and HIV bullet. TB is the leading killer of people with HIV, and the course of both HIV and TB is much more rapid and deadly in persons with both infections In Africa, half of all TB cases are associated with HIV. There is a lot of HIV and TB. TB and HIV are relatively rare in the U.S. due to robust prevention and treatment efforts, 10 to 20 percent of TB cases are associated with HIV.

86
Who is helping? World Health Organization
Global Fund for AIDS, Tuberculosis and Malaria (GFATM) Responds to intertwining threats by underwriting expanded treatment programs Gates Foundation $186 million to fight malaria $200 million with NIH for childhood vaccines, insect control, nutrition, new treatments Read bullets. ***** The Global Fund for AIDS, Tuberculosis and Malaria (GFATM) was established to respond to these intertwining threats and has taken the first tentative steps towards underwriting expanded treatment programs on a country and regional basis. Although commitments to spend $2 billion by 2005 have been made, so far only $150 million has been disbursed. Despite the growing recognition that these diseases are a linked catastrophe, political will by the donor nations has lagged and the GFATM remains underfunded. The Gates Foundation recently committed $168 million to fighting malaria and has issued challenges to develop affordable tests to diagnose infectious diseases and monitor therapy for HIV. The Grand Challenges in Global Health initiative is a $200 million partnership with the National Institutes of Health to get scientists to address open scientific questions in such fields as childhood vaccines, insect control, nutrition, and new treatments for debilitating latent infections that impede international development. But the largest world body addressing the multiplicity of disease in the developing world is the World Health Organization (WHO), which, together with the UN’s UNAIDS and other partners has launched an ambitious plan to bring HIV treatment to 3,000,000 people who need it over the next two years. While the thrust of this program is to procure drugs and diagnostics and establish guidelines for treating HIV with a restricted list of standard regimens, the necessary expansion of training and capacity improvement in the health care sector to allow ARV delivery is also expected to strengthen the ability to deliver a broader range of health services.
 Responds to intertwining threats by underwriting expanded treatment programs. Gates Foundation. $186 million to fight malaria. $200 million with NIH for childhood vaccines, insect control, nutrition, new treatments. Read bullets. ***** The Global Fund for AIDS, Tuberculosis and Malaria (GFATM) was established to respond to these intertwining threats and has taken the first tentative steps towards underwriting expanded treatment programs on a country and regional basis. Although commitments to spend $2 billion by 2005 have been made, so far only $150 million has been disbursed. Despite the growing recognition that these diseases are a linked catastrophe, political will by the donor nations has lagged and the GFATM remains underfunded. The Gates Foundation recently committed $168 million to fighting malaria and has issued challenges to develop affordable tests to diagnose infectious diseases and monitor therapy for HIV. The Grand Challenges in Global Health initiative is a $200 million partnership with the National Institutes of Health to get scientists to address open scientific questions in such fields as childhood vaccines, insect control, nutrition, and new treatments for debilitating latent infections that impede international development. But the largest world body addressing the multiplicity of disease in the developing world is the World Health Organization (WHO), which, together with the UN’s UNAIDS and other partners has launched an ambitious plan to bring HIV treatment to 3,000,000 people who need it over the next two years. While the thrust of this program is to procure drugs and diagnostics and establish guidelines for treating HIV with a restricted list of standard regimens, the necessary expansion of training and capacity improvement in the health care sector to allow ARV delivery is also expected to strengthen the ability to deliver a broader range of health services.")
87
Drug Resistance and Tuberculosis

88
Drug Resistance Selective pressure –Darwin’s theory of survival of the fittest Resistance is expected Factors can reduce development of resistance Finish a course of antibiotics Only those who need antibiotics Narrow spectrum Why finish a course? More important for certain diseases – strep throat, tuberculosis. Antibiotics generally kill off the weak bacteria first. The tougher ones are more likely to die off with extra pummelling. That is why there is usually a ten day course to be followed. When the course is stopped early, the few and the strong multiply. ACK! It's the stronger variety that has been selected to continue on and make the rest of us miserable. What we have here is evolution on a microbial scale with an extra boost from antibiotic misuse.

89
How does an organism acquire resistance?
Mutation and selection Exchange of genes between strains and species Mutation and selection (vertical evolution) Exchange of genes between strains and species (horizontal evolution) Acquired resistance Bacteria that don’t begin life resistant to a certain antibiotic can acquire that resistance. In the case of vertical evolution and inherent resistance, mutations occur on chromosomes and are then selected for an environment where resistance increases fitness. In the case of horizontal evolution, genes pass from a resistant strain to a nonresistant strain, conferring resistance on the latter. The introduction of an antibiotic alters the environment and acts as a selective pressure. Conjugation Transmission of resistance genes via plasmid exchange. Bacteria have circles of DNA called plasmids that they can pass to other bacteria during conjugation. Plasmids, the key players in conjugation, are even referred to as resistance transfer factors. This type of acquisition allows resistance to spread among a population of bacterial cells much faster than simple mutation and vertical evolution would permit. Transduction A virus serves as the agent of transfer between bacterial strains. Transformation DNA released from a bacterium is picked up by a new cell. After the new DNA is introduced—whether via conjugation, transduction, or transformation—it is incorporated into the cell and results in the emergence of a new, resistant genotype. Source: Essential Biochemistry
 Exchange of genes between strains and species (horizontal evolution) Acquired resistance. Bacteria that don’t begin life resistant to a certain antibiotic can acquire that resistance. In the case of vertical evolution and inherent resistance, mutations occur on chromosomes and are then selected for an environment where resistance increases fitness. In the case of horizontal evolution, genes pass from a resistant strain to a nonresistant strain, conferring resistance on the latter. The introduction of an antibiotic alters the environment and acts as a selective pressure. Conjugation. Transmission of resistance genes via plasmid exchange. Bacteria have circles of DNA called plasmids that they can pass to other bacteria during conjugation. Plasmids, the key players in conjugation, are even referred to as resistance transfer factors. This type of acquisition allows resistance to spread among a population of bacterial cells much faster than simple mutation and vertical evolution would permit. Transduction. A virus serves as the agent of transfer between bacterial strains. Transformation. DNA released from a bacterium is picked up by a new cell. After the new DNA is introduced—whether via conjugation, transduction, or transformation—it is incorporated into the cell and results in the emergence of a new, resistant genotype. Source: Essential Biochemistry.")
90
You be the Doctor You are the health care provider and you have a patient with active TB TB strain in patient is susceptible to isoniazid, rifampin, ethambutal Poll: Which drug(s)? How long? 2 weeks, 6 months or 2 years?
 How long 2 weeks, 6 months or 2 years")
91
Choices to treat TB Isoniazid: Rifampin Ethambutol
1 in 106 organisms is resistant to isoniazid Adverse: liver toxicity Rifampin 1 in 108 organisms is resistant Adverse: liver toxicity, interactions with other meds Ethambutol 1 in 106 organisms is resistant Adverse: eye damage Poll: Which drug(s)? How long? 2 weeks, 6 months or 2 years
 How long 2 weeks, 6 months or 2 years.")
92
Treat with Isoniazid x x x
1 in 106 organisms is resistant to isoniazid At 2 weeks, 25% chance of resistant organisms Not Cured! At 6 months, 60% chance Cured! At 2 years, 80% chance Not cured! Resistance to isoniazid! 999,999 1 > x x x

93
Treat with Rifampin x x 1 in 108 organisms is resistant to rifampin
At 2 weeks, 25% chance of resistant organisms Not cured! At 6 months, 60% chance Not cured! Resistance to rifampin! At 2 years, 80% chance 99,999,999 1 > x x

94
Treat with Ethambutol x x x
1 in 106 organisms is resistant to ethambutol At 2 weeks, 25% chance of resistant organisms Not cured! Resistant to ethambutol! At 6 months, 60% chance Not cured! Resistance to ethambutol! At 2 years, 80% chance 999,999 1 x x x

95
Treat with Isoniazid and Rifampin
The probability of developing resistance to 2 unrelated agents is the product of probabilities 1 in 106 x 1 in 108 = 1 in 1014 Spontaneous evolution of multidrug-resistant bacillus is exceedingly rare

96
Solution Always treat with at least two drugs for which the strain is susceptible. If resistance develops, add at least two drugs for which the strain is susceptible

97
Case 2 – Two patients with TB resistant to Isoniazid
Which drug combination?

98
6 month Check-up Patient 1 has no active TB infection
Patient 2 has TB resistant to all three drugs. Why?

99
TB in the Last Century TB incidence declined in the 1960’s and 1970’s. Incidence increased in the 1980’s. Drug prescription practices followed the previously mentioned guidelines. Why did therapy fail? Compliance.

100
Directly Observed Therapy Short-course (DOTS)
A health care worker watches and helps as the patient swallows anti-TB medicines in his/her presence. DOTS shifts responsibility for cure from patient to health care system Requires political commitment, accurate diagnosis, quality drugs, observation, follow up DOTS works well in many developing countries DOTS is a multifaceted approach to TB therapy, including observed pill-taking, community and local government commitment, case detection by sputum smear microscopy, stable drug supply, and standardized systems for case follow-up. Successful DOTS programs include all of these essential activities.

101
Directly Observed Therapy with HIV
Controversial Requiring DOT may impose substantial barriers to drugs in resource-poor countries HIV is more stigmatizing than TB Does directly observed therapy prevent more HIV mortality and transmission than self-administered therapy? How would you find out? Recent price cuts and the introduction of "off-patent" antiretroviral HIV/AIDS drugs bring new hope that antiretroviral therapy will become more widely available in the resource-poor countries where over 90 percent of HIV infections occur. There is concern, however, that poor adherence to antiretroviral therapy will accelerate widespread drug resistance in Africa, and some maintain that treatment should be delayed until adherence can be ensured. Based on concerns that the widespread, unregulated access to antiretroviral drugs in sub-Saharan Africa could lead to the rapid emergence of drug-resistant viral strains, creating havoc for individuals, curtailing future treatment options, and leading to the transmission of resistant virus, directly observed therapy programs for tuberculosis have been proposed as a model for the provision of HIV drugs in resource-poor countries. But the authors of the current study propose that calls for such programs to provide routine HIV care are premature, as "witnessed dosing has unclear efficacy in improving adherence and reducing HIV transmission, and may paradoxically promote drug resistance. Furthermore, requiring directly observed therapy may impose substantial barriers to antiretroviral access in resource-poor countries." The call for directly observed HIV therapy is rooted in experience with TB treatment. DOTS is a multifaceted approach to TB therapy, including observed pill-taking, community and local government commitment, case detection by sputum smear microscopy, stable drug supply, and standardized systems for case follow-up. Successful DOTS programs include all of these essential activities. While observational studies suggest that DOTS programs achieve higher cure rates than historical controls, the impact of witnessed therapy has rarely been isolated from other components of the DOTS strategy. As has been argued elsewhere, the success of TB control programs depends more on the strength of diverse structural components, including reliable drug supply and distribution, than just on observed dosing. Many believe that widespread poverty in resource-poor countries makes adherence a particular concern for the provision of HIV therapy. However, early data suggest that adherence to combination antiretroviral therapy is at least as good as in wealthy countries. Two recent South African studies determined that adherence ranged from 88 percent to 95 percent in clinical trial settings that included impoverished participants. Though such studies may not be representative of the larger HIV-positive population in resource-poor countries, there remains no evidence to suggest that adherence will be less in poorer countries. Studies with objective adherence measures indicate that HIV-positive patients in wealthy countries take roughly 70 percent of their medication. There is nothing to preclude equal or better adherence in resource-poor countries. Preventing HIV transmission is the strongest rationale for making adherence interventions a requirement of therapy. However, the assumption that treatment will prevent transmission and that treatment with directly observed therapy will prevent more transmission than treatment with self-administered therapy has not yet been tested. Because HIV is more stigmatizing than TB and requires lifelong therapy, the negative impact of directly observed HIV therapy on human rights could be potentially greater than TB. Although the prospect of access to treatment may encourage individuals to determine their HIV status, the linkage of treatment to directly observed therapy may paradoxically lower the use of counseling and testing services due to confidentiality concerns. In the United States, fears regarding HIV disclosure have led to a delay in treatment. These issues underscore the potential impact of compromising privacy by linking treatment to directly observed therapy programs. While the authors "suggest restraint in the enthusiasm for directly observed HIV therapy as part of routine HIV care," they cannot "minimize the importance of developing effective and culturally appropriate voluntary adherence interventions to improve individual treatment outcomes globally. While the public health advantages of directly observed HIV therapy are in question, the impact on individual freedoms is not. We do not require direct observation of HIV therapy in resource-rich countries, and unless rigorous studies find important differences in adherence, there is no rationale for a different approach in resource-poor settings. We should not assume inequity with respect to people's ability to self-direct their medical care, including adherence to therapy."

102
Clinical Trial Question: Does combined directly observed therapy for HIV and TB decrease HIV mortality in a resource-limited developing country? NIH study in resource-poor Durban, South Africa 2 groups of patients: Group 1 will undergo DOT for HIV and TB simultaneously. Group 2 will undergo DOTS for TB and HIV therapy without DOT Primary outcome: Diagnosis of an AIDS-defining illness; 18-month mortality TB is the most common serious infectious complication associated with HIV in sub-Saharan Africa and is also the most common cause of death among HIV infected patients in developing countries. Furthermore, TB in an HIV infected person accelerates the progression of HIV disease and hastens death. This study will evaluate a combined TB and antiretroviral treatment (ART) strategy utilizing DOT in HIV infected people coinfected with TB. This study will compare two treatment strategies: TB and HIV medications given concurrently (integrated arm) and TB treatment completed first, followed by HIV treatment (sequential arm). This study has two parts. The entire study will last 24 months after participants have been randomly assigned to one of two arms. Arm 1 (integrated arm) participants will receive didanosine (ddI), efavirenz (EFV), and lamivudine (3TC) once daily concurrent with standard TB therapy. ART and TB medications will be provided through DOT on weekdays; participants will take their medications without DOT on weekends. Arm 1 participants will also attend four 15- to 20-minute sessions of an adherence study program at study start, Week 2, Month 2, and 1 to 3 weeks prior to the end of TB therapy. Arm 2 (sequential arm) participants will first receive DOT-provided TB treatment alone. After completion of TB treatment, participants will receive ddI, EFV, and 3TC once daily without DOT. Study visits in the first part of the study will occur at screening, study start, Weeks 1, 2, and 3, and every month until the end of the first part of the study at Month 12. Study visits will include blood collection, medical and medication history assessment, a physical exam, and pill counts. Patients will be asked to complete an adherence questionnaire at every study visit and a sexual behavior survey and quality of life questionnaire at study start and Month 6.
 strategy utilizing DOT in HIV infected people coinfected with TB. This study will compare two treatment strategies: TB and HIV medications given concurrently (integrated arm) and TB treatment completed first, followed by HIV treatment (sequential arm). This study has two parts. The entire study will last 24 months after participants have been randomly assigned to one of two arms. Arm 1 (integrated arm) participants will receive didanosine (ddI), efavirenz (EFV), and lamivudine (3TC) once daily concurrent with standard TB therapy. ART and TB medications will be provided through DOT on weekdays; participants will take their medications without DOT on weekends. Arm 1 participants will also attend four 15- to 20-minute sessions of an adherence study program at study start, Week 2, Month 2, and 1 to 3 weeks prior to the end of TB therapy. Arm 2 (sequential arm) participants will first receive DOT-provided TB treatment alone. After completion of TB treatment, participants will receive ddI, EFV, and 3TC once daily without DOT. Study visits in the first part of the study will occur at screening, study start, Weeks 1, 2, and 3, and every month until the end of the first part of the study at Month 12. Study visits will include blood collection, medical and medication history assessment, a physical exam, and pill counts. Patients will be asked to complete an adherence questionnaire at every study visit and a sexual behavior survey and quality of life questionnaire at study start and Month 6.")
104
Back Up Inherent (Natural) Resistance. Bacteria may be inherently resistant to an antibiotic. For example, a streptomycete has some gene that is responsible for resistance to its own antibiotic; or a Gram-negative bacterium has an outer membrane that establishes a permeability barrier against the antibiotic; or an organism lacks a transport system for the antibiotic; or it lacks the target or reaction that is hit by the antibiotic. Acquired Resistance. Bacteria can develop resistance to antibiotics, e.g. bacterial populations previously-sensitive to antibiotics become resistant. This type of resistance results from changes in the bacterial genome. Acquired resistance is driven by two genetic processes in bacteria: (1) mutation and selection (sometimes referred to as vertical evolution); (2) exchange of genes between strains and species (sometimes called horizontal evolution). Vertical evolution is strictly a matter of Darwinian evolution driven by principles of natural selection: a spontaneous mutation in the bacterial chromosome imparts resistance to a member of the bacterial population. In the selective environment of the antibiotic, the wild type (non mutants) are killed and the resistant mutant is allowed to grow and flourish. The mutation rate for most bacterial genes is approximately This means that if a bacterial population doubles from 108 cells to 2 x 108 cells, there is likely to be a mutant present for any given gene. Since bacteria grow to reach population densities far in excess of 109 cells, such a mutant could develop from a single generation during 15 minutes of growth. Horizontal evolution is the acquisition of genes for resistance from another organism. For example, a streptomycete has a gene for resistance to streptomycin (its own antibiotic), but somehow that gene escapes and gets into E. coli or Shigella. Or, more likely, Some bacterium develops genetic resistance through the process of mutation and selection and then donates these genes to some other bacterium through one of several processes for genetic exchange that exist in bacteria. Bacteria are able to exchange genes in nature by three processes: conjugation, transduction and transformation. Conjugation involves cell-to-cell contact as DNA crosses a sex pilus from donor to recipient. During transduction, a virus transfers the genes between mating bacteria. In transformation, DNA is acquired directly from the environment, having been released from another cell. Genetic recombination can follow the transfer of DNA from one cell to another leading to the emergence of a new genotype (recombinant). It is common for DNA to be transferred as plasmids between mating bacteria. Since bacteria usually develop their genes for drug resistance on plasmids (called resistance transfer factors, or RTFs), they are able to spread drug resistance to other strains and species during genetic exchange processes. The combined effects of fast growth rates, high concentrations of cells, genetic processes of mutation and selection, and the ability to exchange genes, account for the extraordinary rates of adaptation and evolution that can be observed in the bacteria. For these reasons bacterial adaptation (resistance) to the antibiotic environment seems to take place very rapidly in evolutionary time: bacteria evolve fast!
 Resistance. Bacteria may be inherently resistant to an antibiotic. For example, a streptomycete has some gene that is responsible for resistance to its own antibiotic; or a Gram-negative bacterium has an outer membrane that establishes a permeability barrier against the antibiotic; or an organism lacks a transport system for the antibiotic; or it lacks the target or reaction that is hit by the antibiotic. Acquired Resistance. Bacteria can develop resistance to antibiotics, e.g. bacterial populations previously-sensitive to antibiotics become resistant. This type of resistance results from changes in the bacterial genome. Acquired resistance is driven by two genetic processes in bacteria: (1) mutation and selection (sometimes referred to as vertical evolution); (2) exchange of genes between strains and species (sometimes called horizontal evolution). Vertical evolution is strictly a matter of Darwinian evolution driven by principles of natural selection: a spontaneous mutation in the bacterial chromosome imparts resistance to a member of the bacterial population. In the selective environment of the antibiotic, the wild type (non mutants) are killed and the resistant mutant is allowed to grow and flourish. The mutation rate for most bacterial genes is approximately This means that if a bacterial population doubles from 108 cells to 2 x 108 cells, there is likely to be a mutant present for any given gene. Since bacteria grow to reach population densities far in excess of 109 cells, such a mutant could develop from a single generation during 15 minutes of growth. Horizontal evolution is the acquisition of genes for resistance from another organism. For example, a streptomycete has a gene for resistance to streptomycin (its own antibiotic), but somehow that gene escapes and gets into E. coli or Shigella. Or, more likely, Some bacterium develops genetic resistance through the process of mutation and selection and then donates these genes to some other bacterium through one of several processes for genetic exchange that exist in bacteria. Bacteria are able to exchange genes in nature by three processes: conjugation, transduction and transformation. Conjugation involves cell-to-cell contact as DNA crosses a sex pilus from donor to recipient. During transduction, a virus transfers the genes between mating bacteria. In transformation, DNA is acquired directly from the environment, having been released from another cell. Genetic recombination can follow the transfer of DNA from one cell to another leading to the emergence of a new genotype (recombinant). It is common for DNA to be transferred as plasmids between mating bacteria. Since bacteria usually develop their genes for drug resistance on plasmids (called resistance transfer factors, or RTFs), they are able to spread drug resistance to other strains and species during genetic exchange processes. The combined effects of fast growth rates, high concentrations of cells, genetic processes of mutation and selection, and the ability to exchange genes, account for the extraordinary rates of adaptation and evolution that can be observed in the bacteria. For these reasons bacterial adaptation (resistance) to the antibiotic environment seems to take place very rapidly in evolutionary time: bacteria evolve fast!")
105
Malaria Control Reduce human/insect contact Prevent mosquito breeding
Use insect repellents, mats, coils, bednets Residual treatment of interior walls Insecticide-treated mosquito nets Expensive. Any solutions?

106
What are the Challenges for Malaria?
Mapping areas that are difficult to access Poor communication Direction – Transfer of vector control efforts from malaria control authorities to local primary health care center Financial support – decreased standard of living from wars, environmental factors, migration Corruption, graft

107
HIV, TB, and Malaria Selected Preventable Causes of Death
HIV/AIDS 2,886,000 TB 1,664,000 Malaria 1,124,000 Diarrheal diseases 2,001,000 Perinatal conditions 2,504,000 Childhood diseases 1,318,000 Lung cancer 1,213,000 Traffic accidents 1,194,000 Suicide 849,000 War ,000 Source: The World Health Report 2002, WHO Collectively, HIV, TB, and malaria may be responsible for over six million deaths per year, with many more trailing in their wake as the burden on economies and health care capacity becomes overwhelming. Indeed, there are opportunities to be mined in these overlapping epidemics. Increasingly, the fear that destabilized societies and economies may impact the security of Western nations has stimulated a great deal of rhetoric and an increasing amount of money dedicated to addressing the burden of disease in the world. Hopefully, several emerging global partnerships will be able to direct a coordinated and effective response to these threats as the promised resources become available.

Similar presentations













 Facts>")





 Randy Kim.>")



>")
