Download presentation
Presentation is loading. Please wait.

1
Assessment of Operability in CHD with PAH
Krishna Kumar Amrita Institute of Medical Sciences and Research Center Cochin Kerala, India

2
Congenital Heart Disease
Surgery for PDA Paul Wood: Eisenmenger syndrome, Open heart surgery for common shunts Early Open Heart surgery in Infants Infant open heart surgery widely established in developed countries Infant open heart surgery in selected parts of the developing world 100% Developed world Percentage of infants with large VSD receiving timely surgery Developing world

3
Pulmonary Vascular Obstructive Disease
Definition: PVR in CHD (Qp) Precludes safe closure PAp high after closure; may further Timely CHD correction: prevents (but not eliminates) Common in developing world
 Precludes safe closure. PAp high after closure; may further Timely CHD correction: prevents (but not eliminates) Common in developing world.")
4
Estimated proportion of infants with critical CHD undergoing surgery within the first year of life in India Number undergoing surgery in the first year of life Estimated number of infants with critical CHD 2012

5
CHD Services in Selected Asian Countries
Sources: 1: Children’s HeartLink, 2: Dr. Sukman Putra, 3. Dr. Masood Sadiq ,4. Dr. Euneil Solinap, 5. Dr. Duminda Samarasinghe

6
Parts of The World Where the Average Child in the Region has Access to Congenital Heart Surgery

7
Deciding operability of L-R shunts
Clinical evaluation Chest X-ray and ECG Measurement of oxygen saturation Echocardiography MRI Cardiac catheterization

8
Agenda Basic concepts How do we decide on operability of L-R shunts today? What are the indications to perform catheterization? What are the limitations of the tools that we have with us?

9
What determines the development of pulmonary vascular obstructive disease?
Pre vs. post tricuspid Size Associated lesions: pulmonary venous hypertension Lungs and airways obstruction Altitude Syndromes: Tri-21 Anatomy of defect Associated conditions Time Unknown influences * Genetic???

10
Conceptual framework:
Pre-tricuspid shunts: gradual increase in Qp as RV accommodates and enlarges – ASD, PAPVC, TAPVC* Post tricuspid shunts: Direct transmission of pressure head: VSD (systolic), PDA, AP-Window (systolic and diastolic)
, PDA, AP-Window (systolic and diastolic)")
11
Conceptual framework:
Pulmonary venous hypertension, associated mitral stenosis, other forms of LV inflow obstruction: May introduce a substantial element of reversibility May protect pulmonary vasculature from the effects of increased pulmonary blood flow???

12
Conceptual framework:
Hypoxia elevates pulmonary vascular resistance Diseases of pulmonary parenchyma Airways (upper and lower) Hypoventilation High altitude
 Hypoventilation. High altitude.")
13
Conceptual framework:
Time The likelihood of development of PVOD increases with time The rate of increase in PVR varies depending on a number of influences

14
Defect vs. PVOD Risk 100% TGA VSD/PDA Unrestrictive VSD or PDA
Large Fossa ovalis ASD Truncus SV ASD Likelihood of operability Age Early childhood Infancy Adolescence Adulthood

15
Risk of development of PVOD: Other (unknown) influences
Remarkable individual variability ASD with severe PAH in a child VSD with shunt reversal in an infant Operable AP window in a teenager Operable large VSD in an adult Prediction for an individual patient is sometimes quite challenging

16
Other (?Genetic) Influences
Least Most IPAH?? Risk of PVOD

17
What principles govern decision on operability?
Post tricuspid shunts: Generally operable if there is evidence of a significant shunt in the basal state irrespective of PA pressure Pre-tricuspid shunts: Pulmonary hypertension (anything more than mild) warrants concern especially if basal shunt is not obvious
 warrants concern especially if basal shunt is not obvious.")
18
Deciding operability: Principles
Age is an important variable and benefit of doubt must be given to younger patients. E.g. a 1 year old with VSD and severe PAH where basal shunt is not obvious Lung, airway and ventilation issues can elevate PVR and confound assessment Pulmonary venous hypertension can result in reversible elevations in PVR

19
Congenital Heart Disease (L-R shunts) and Pulmonary Hypertension
Maurice Beghetti, and Nazzareno Gali, J. Am. Coll. Cardiol. 2009;53;

21
Clinical Spectrum of PAH in CHD
Operable Clear evidence of a large L-R shunt Typically younger patients Borderline situation: PVR elevated ; operability uncertain. Inoperable: Eisenmenger physiology Shunt reversal Typically older patients

23
Clearly Operable: Cath not required
LV RV LA LV RA RV Clearly Operable: Cath not required

24
26 year old Blue Single loud S2

25
Clearly Inoperable: Cath not required
RV LV RA LA Clearly Inoperable: Cath not required

26
Clinical spectrum of post-tricuspid shunts with PAH
Operable Failure to thrive, precordial activity, mid diastolic murmur at apex, Cardiac enlargement, pulmonary blood flow Q in lateral leads on ECG, good LV forces LA/LV enlargement, exclusively L-R flows across the defect Clear clinical /noninvasive evidence of a large left – right shunt Borderline clinical non-invasive data: uncertain operability Cyanosis, quiet precordium, no MDM Normal heart size, peripheral pruning No Q in lateral leads, predominent RV forces No LA LV enlargement, significant R-L flows across the defect Clear evidence of shunt reversal resulting from high PVR. Inoperable

27
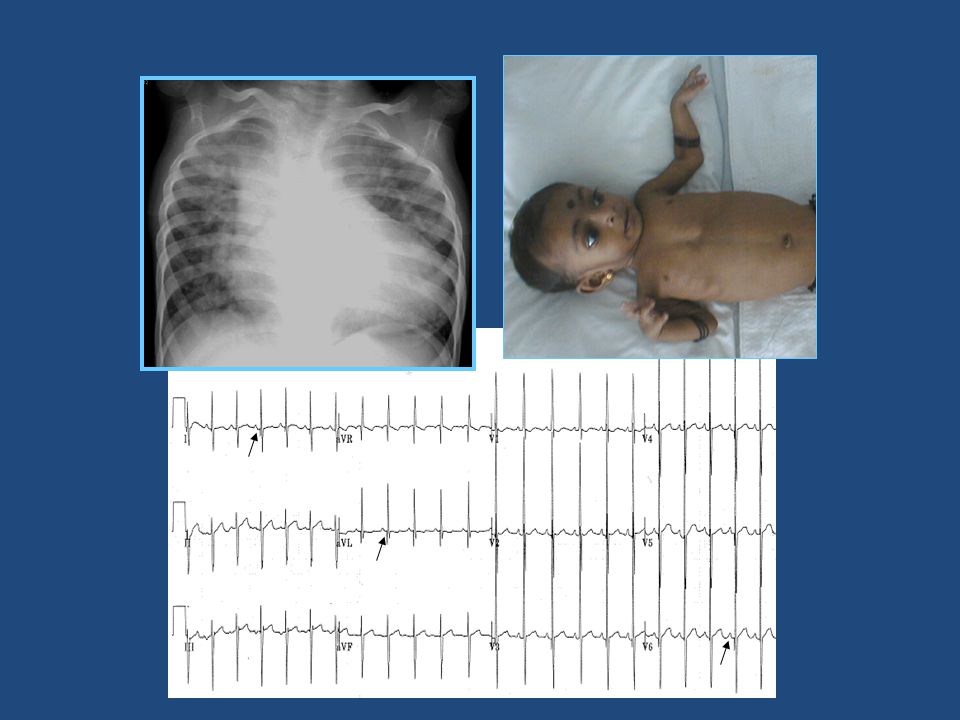
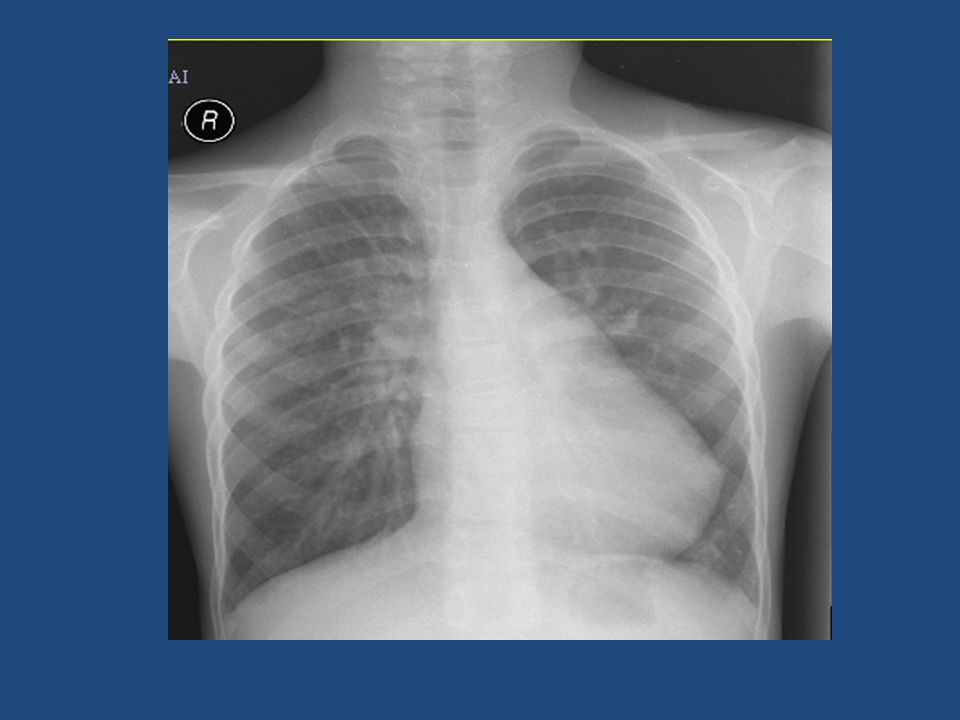
Another Example…… 10 yr old boy
Detected to have congenital heart disease in early infancy but did not undergo surgery. Asymptomatic except for an occasional respiratory infection

28
Evaluation Normal Growth & Development. Pulse: 88/min, BP: 104/70mmHg
SPO2: 100% CVS: S1 normal .S2 split normally. A2=P2 Harsh ESM at LUSB. S3+. RS: B/L Clear. No hepatomegaly.

30
ECG 75/min. P axis 60deg, QRS axis: 75deg. No e/o atrial enlargement R/S: V1=25/5, V6=35/20. tiny q waves in V6

31
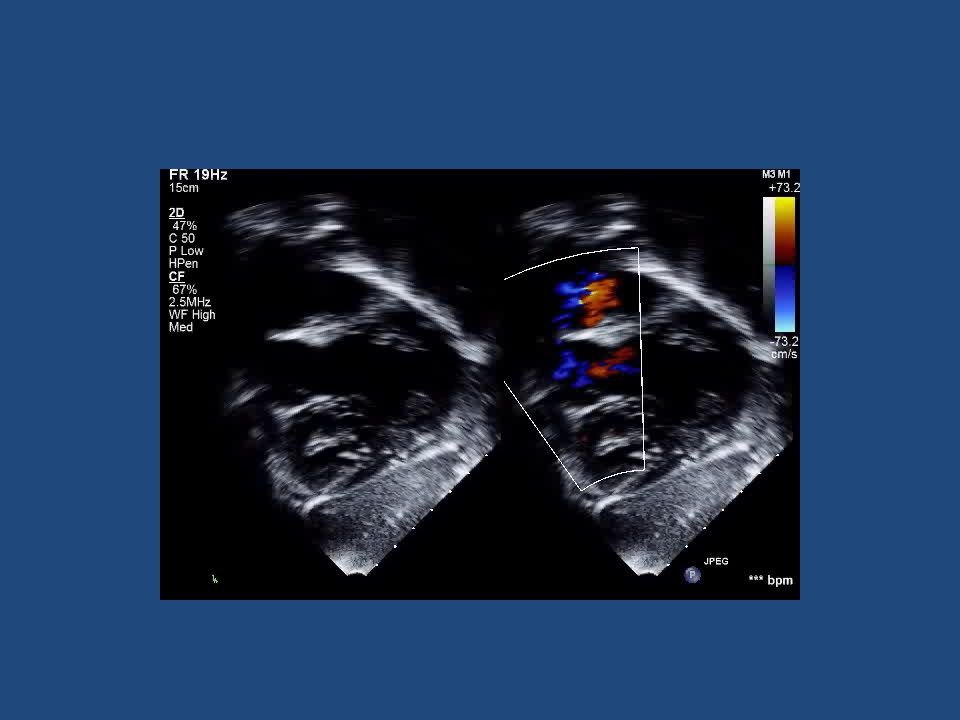
ECHO

33
Cath Data (Room Air) Dias(a) Mean O2 % SVC 3 6 2 74.7 RA PA 105 46 75
Chamber Sys(v) Dias(a) Mean O2 % SVC 3 6 2 74.7 RA PA 105 46 75 85 PA wedge 5 PV 98 (a) RV 120 ED= 4 Ao 114 54 77 94.3 PV was not entered. Saturation was assumed Oxygen consumption was assumed
 Dias(a) Mean. O2 % SVC RA. PA PA wedge. 5. PV. 98 (a) RV ED= 4. Ao PV was not entered. Saturation was assumed. Oxygen consumption was assumed.")
34
Parameter Condition 1 ( room air) O2 Consumption 156 ml/m2 Qp 6.01 Qs 4.47 Qep 3.5 Qp/Qs 1.34 PVRI 11.82 SVRI 16.78 L-R shunt 2.51

35
Decision Has cath data helped to make a decision
Is he suitable for VSD closure? Do we significantly alter his natural history by intervention? Should we test with pulmonary vasodilators?

36
FLOW AND RESISTANCE CALCULATIONS
Parameter Condition 1 ( room air) Condition 2 (FiO2 100) Condition 3 (NO 40PPM + O2) O2 Consumption 156 152 Qp 6.01 8.66 8.9 Qs 4.47 4.05 3.68 Qep 3.5 Qp/Qs 1.34 2.14 PVRI 11.82 7.5 6.74 SVRI 16.78 19.25 18.2
 Condition 2. (FiO2 100) Condition 3. (NO 40PPM + O2) O2 Consumption Qp Qs Qep Qp/Qs PVRI SVRI")
37
Our Management Plan The family was counseled
Underwent fenestrated VSD closure + PDA ligation

38
Post op course Uneventful PA pressure 1/3 to ½ systemic
Extubated by day 2 Echo at discharge: Fenestration L->R IVG: 60mmHg Discharged on PDE5 inhibitors

39
Small Fenestration in VSD patch L->R Mild TR. RVSP 65+ RA.
Follow Up Echo Small Fenestration in VSD patch L->R Mild TR. RVSP 65+ RA.

40
CATH Data (On Sildenafil, 1 year later)
Chamber Sys(v) Dias(a) Mean O2 % PO2 SVC 79.8 45.9 RA 2 PA 66 30 50 82.7 48.2 PV 99(a) PA wedge 5 LV 120 ED 6 Ao 118 78 98 97.7 93.4 PVRI: 7.96 WU; PVR/SVR ratio: 0.4
 Dias(a) Mean. O2 % PO2. SVC RA. 2. PA PV. 99(a) PA wedge. 5. LV ED 6. Ao PVRI: 7.96 WU; PVR/SVR ratio: 0.4.")
41
Ideally….. Cath Operable Operable Operable Borderline Inoperable

42
PVR Estimation by Cardiac Catheterization
Pulmonary artery mean pressure Pulmonary venous mean pressure Trans-pulmonary gradient PVR = Pulmonary blood flow Oxygen consumption PVO2 content PA O2 Content

43
Sources of Error / Limitations in Catheterization Data
Assumed oxygen saturations Assumed pulmonary vein saturation “Non-physiologic” state Calculated PVRI (basal and post-pulmonary vasodilator) has not been adequately standardized against the gold standard “surgical outcome”
 has not been adequately standardized against the gold standard surgical outcome")
44
In the Real World…… Operable Inoperable Borderline Operable Inoperable

45
Cath criteria (Baseline Room Air)
Favorable Unfavorable PVRI (Wood U) <6 (Ideally < 4) >8 PVR/SVR ratio <0.3 >0.5 Positive vasodilator: > 20% fall in PVR Lopes et al Pulmonary Circulation 2013
 <6 (Ideally < 4) >8. PVR/SVR ratio. <0.3. >0.5. Positive vasodilator: > 20% fall in PVR. Lopes et al Pulmonary Circulation")
46
Indication for Cath in ASD
Clinical clues may be less obvious than VSD or PDA Echo evidence of elevated PA pressure (RVSP > mm Hg: Suggests need for cath Clear evidence of flow reversal (sats < 90%) suggestive of PVR do not require cardiac cath
 suggestive of PVR do not require cardiac cath.")
47
Indications for Cardiac Cath: Data From Amrita Institute: 1998-2001

48
Interventricular and Transductal velocity by Doppler
Clear understanding of the hemodynamics Comprehensive clinical assessment Influenced by the pulmonary artery and aortic pressures at the time of examination Proper alignment is essential Left parasternal view or high parasternal view for ductus; no ‘best’ view for VSD Record peak systolic and end diastolic gradients in PDA

49
Deciding operability of L-R shunts
Clinical evaluation Chest X-ray and ECG Measurement of oxygen saturation Echocardiography Resting and post exercise ABG (PO2) Cardiac catheterization ?MRI Viswanathan S, Kumar RK, Assessment of operability in congenital cardiac shunts with increased pulmonary vascular resistance, Cathet Cardiovasc Interv. 2008; 71:665-70
 Cardiac catheterization. MRI. Viswanathan S, Kumar RK, Assessment of operability in congenital cardiac shunts with increased pulmonary vascular resistance, Cathet Cardiovasc Interv. 2008; 71:")
50
What else can be done in the cath lab?
Test occlusion of the defects: ASD PDA Little validation with long term data Immediate reduction of PA pressure may not translate into long term benefits

51
Illustrative Example 16 year old boy, 9.4 mm duct
Nearly systemic PA pressures (Ao 120/60, mean: 90; PA 110/60: mean: 80) LL O2 Saturation: 96% Qp/Qs: 1.15:1 (Qp 3.8; Qs: 3.3) Basal PVRI: Wood Units; PVRI/SVRI ratio: 0.66
 LL O2 Saturation: 96% Qp/Qs: 1.15:1 (Qp 3.8; Qs: 3.3) Basal PVRI: Wood Units; PVRI/SVRI ratio:")
52
Illustrative Example Balloon Occlusion PA Ao

53
Illustrative Example 5 minutes after balloon occlusion Ao: 125/77 (96)
PA: 66/18 (41)
")
54
Conclusions Comprehensive clinical evaluation supplemented by echocardiography: Allows adequate hemodynamic assessment of for decision making in > 95% of patients with L-R shunts. Cardiac cath and pulmonary vasodilator testing is often done for borderline situations ?uncertain incremental value Some exceptions: Test occlusion of PDA

55
VSD: Case 1 8 months old boy
6mm perimembranous VSD, partly covered by STL IVG 60mmHg CFM: turbulent jet across the VSD Mild LA, LV dilatation

56
VSD: Case 2 3 year old girl 7 mm perimembranous VSD IVG 10mmHg
CFM: Nonturbulent flow across the VSD, transient right to left flow in diastole LA, LV dilatation

57
VSD: Case 3 8 months old girl 2mm perimembranous VSD IVG 10mmHg
CFM: Nonturbulent flow across the VSD

58
VSD: Case 4 1.5 year old, Intracardiac repair done for TOF
Weaning from ventilator not possible Echo: 3mm residual VSD, IVG 70mmHg, IVS motion paradoxical, mild LA and LV dilatation Cath: RVSP 70mmHg, LVSP 90mmHg, Qp:Qs 2.2

59
PA Pressure Estimation: Ideal Situation
Ideally, the peak instantaneous gradient measured by Doppler in VSD should be quite similar to the peak-peak gradient by cath. Peak-peak (cath) Peak instantaneous (Doppler)
 Peak instantaneous (Doppler)")
60
PA Pressure Overestimation by Doppler Because of Change in Slope of the RV Pressure Upstroke
If the slope (dp/dt) of the RV systolic pressure trace is slowed (green) because of RBBB or RV dysfunction there can be a significant difference in Doppler vs. cath gradients and Doppler may underestimate PA pressures Peak-peak (cath) Peak instantaneous (Doppler)
 of the RV systolic pressure trace is slowed (green) because of RBBB or RV dysfunction there can be a significant difference in Doppler vs. cath gradients and Doppler may underestimate PA pressures. Peak-peak (cath) Peak instantaneous (Doppler)")
61
In the presence of RBBB or RV dysfunction, IV doppler gradient is unreliable in predicting RVSP/size of the VSD

62
PDA: Case 1 “2mm” PDA Systolic PG 80, Diastolic PG 50
PA pressure 25/15, Ao 110/70

63
PDA: Case 2 “2.5mm” PDA Systolic PG 80, Diastolic PG 30
PA pressure 25/15, Ao 110/50

64
PDA: Case 3 “3mm” PDA SPG 60, DPG 20 PA pressure 60/20, Ao 120/40
An anxious patient or unsedated child will have systolic hypertension and would record high systolic PG even with a relatively large PDA Low (30mmHg) Diastolic gradient predicts significant flow and hence a larger duct
 Diastolic gradient predicts significant flow and hence a larger duct.")
65
PDA: Case 4 5mm PDA PA pressure 110/30, Ao 120/38 SPG 10, DPG 8
“Large but short duct”

66
Transductal velocity Large ‘short’ duct: Aortic pressure gets transmitted directly, can have near systemic or systemic pulmonary pressures. Systolic PG also would be small. Corollary: Small systolic PG may suggest shallow ampulla Large ‘long’ duct: Length of the duct offers resistance, no direct transmission of aortic pressure. Hence systolic PG would be moderately high

67
Flow Reversal in the Abdominal Aorta

68
Transductal velocity If DPG is recorded high, ductus is usually small, probably 2D echo is missing the narrowest PA end Patients with pulmonary vascular disease: small PG or bi-directional flow; duct has to be large Small PG or bi-directional flow but ductus size is small by 2D: Patients with high PVR due to other causes e.g. pneumonia. Corollary: Small gradient does not automatically mean a large duct.

Similar presentations




>")


 RV:15-25 edp 0-5. PA:15-25; diast. 6-10, m = 10-15. PAW: a = 6-12, V = 8-14, m 6-10 (12) LA (PV): a=6-12, V=8-14,>")












