Download presentation
Presentation is loading. Please wait.

1
Congenital Heart Defects Left-to-Right Shunt Lesions by
Prof Dr AMR MEGAHED

2
Left-to-Right Shunt Lesions
Left-to-right shunt lesions such as atrial septal defect (ASD), ventricular septal defect (VSD), patent ductus arteriosus (PDA)
, ventricular septal defect (VSD), patent ductus arteriosus (PDA)")
3
Congenital Heart Disease
Congenital heart disease is a type of defect or malformation in one or more structures of the heart or blood vessels that occurs before birth. These defects occur while the fetus is developing in the uterus and affect 8-10 out of every 1,000 children. Congenital heart defects may produce symptoms at birth, during childhood, and sometimes not until adulthood.

4
What Causes Congenital Heart Disease?
In the majority of people, the cause of congenital heart disease is unknown. However, there are some factors that are associated with an increased chance of getting congenital heart disease. These risk factors include: Genetic or chromosomal abnormalities in the child such as Down syndrome. Taking certain medications or alcohol or drug abuse during pregnancy. Maternal viral infection, such as rubella (German measles) in the first trimester of pregnancy.
 in the first trimester of pregnancy.")
5
The risk of having a child with congenital heart disease is higher if a parent or a sibling has a congenital heart defect -- the risk increases from eight in 1,000 to 16 in 1,000.

6
Left-to-Right Shunt Lesions
Atrial Septal Defect ASD (ostium secundum defect) occurs as an isolated anomaly in 5 % to 10% of all congenital heart defects. It is more common in females than in males (male/female ratio of 1:2). Types of ASDs exist: Secundum defect Primum defect
 occurs as an isolated anomaly in 5 % to 10% of all congenital heart defects. It is more common in females than in males (male/female ratio of 1:2). Types of ASDs exist: Secundum defect. Primum defect.")
7
Left-to-Right Shunt Lesions
Ostium secundum defect is the most common type of ASD, accounting for 50% to 70% of all ASDs. Ostium primum defects occur in about 30% of all ASDs

8
Left-to-Right Shunt Lesions

9
Left-to-Right Shunt Lesions
CLINICAL MANIFESTATIONS : History.: Infants and children with ASDs are usually asymptomatic Physical Examination A widely split and fixed S2 and a grade 2 to 3/6 systolic ejection murmur are characteristic findings of ASD in older infants and children. With a large left-to-right shunt, a mid-diastolic rumble resulting from relative tricuspid stenosis may be audible at the lower left sternal border.

10
Left-to-Right Shunt Lesions
Electrocardiography Right axis deviation of +90 to +180 degrees and mild right ventricular hypertrophy (RVH) or right bundle branch block (RBBB) with an rsR' pattern in V1 are typical findings. In about 50% of the patients with sinus venosus ASD, the P axis is less than 30 degrees.
 or right bundle branch block (RBBB) with an rsR pattern in V1 are typical findings. In about 50% of the patients with sinus venosus ASD, the P axis is less than 30 degrees.")
13
Left-to-Right Shunt Lesions
Left-to-Right Shunt Lesions

14
Left-to-Right Shunt Lesions
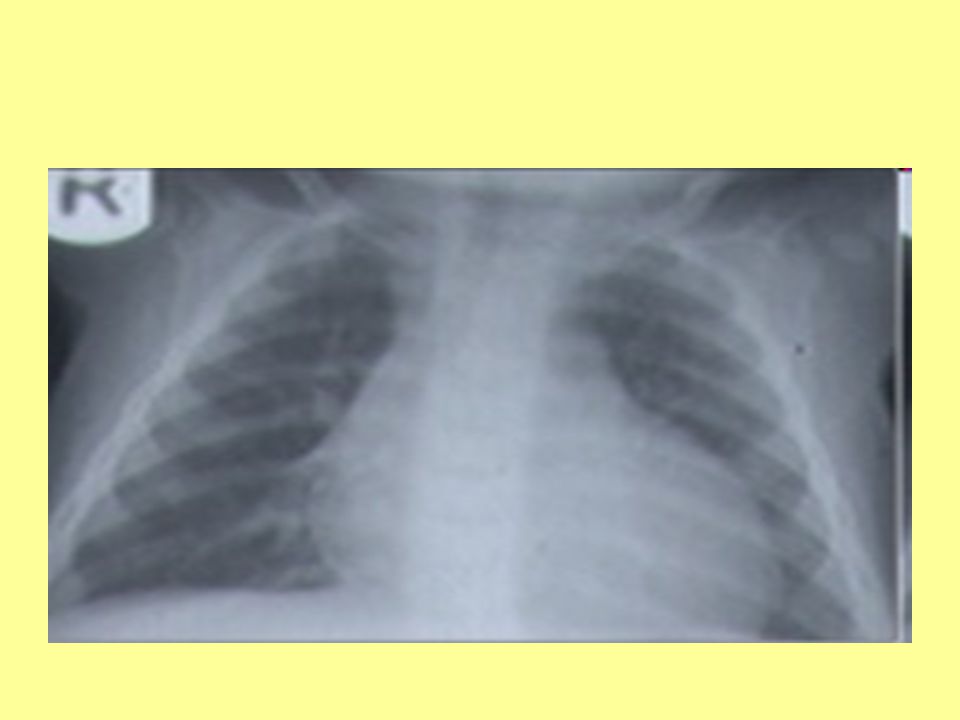
X-ray Studies : Cardiomegaly with enlargement of the RA and right ventricle (RV) may be present. 2. A prominent pulmonary artery (PA) segment and increased pulmonary vascular markings are seen when the shunt is significant.
 may be present. 2. A prominent pulmonary artery (PA) segment and increased pulmonary vascular markings are seen when the shunt is significant.")
17
Left-to-Right Shunt Lesions
Echocardiography MANAGEMENT Medical 1. Exercise restriction is unnecessary. 2. Prophylaxis for infective endocarditis is not indicated unless the patient has associated MVP or other associated defects. Prophylaxis is indicated in patients with primum ASD. 3. In infants with CHF, medical management is recommended because of its high success rate and the possibility of spontaneous closure of the defect.

18
Left-to-Right Shunt Lesions
Nonsurgical closure using a catheter-delivered closure device Surgical Closure

19
Left-to-Right Shunt Lesions
Ventricular Septal Defect VSD is the most common form of congenital heart defect and accounts for 15% to 20% of all such defects PATHOLOGY : The ventricular septum may be divided into a small membranous portion and a large muscular portion

20
Left-to-Right Shunt Lesions
The defects vary in size, ranging from tiny defects without hemodynamic significance to large defects with accompanying CHF and pulmonary hypertension. CLINICAL MANIFESTATIONS With a small VSD, the patient is asymptomatic with normal growth and development

21
Left-to-Right Shunt Lesions
With a moderate to large VSD, delayed growth and development, decreased exercise tolerance, repeated pulmonary infections, and CHF are relatively common during infancy. With long-standing pulmonary hypertension, a history of cyanosis and a decreased level of activity may be present.

22
Left-to-Right Shunt Lesions
A systolic thrill may be present at the lower left sternal border. Precordial bulge and hyperactivity are present with a large-shunt VSD. The intensity of the P2 is normal with a small shunt and moderately increased with a large shunt. The S2 is loud and single in patients with pulmonary hypertension or pulmonary vascular obstructive disease. A grade 2 to 5/6 regurgitant systolic murmur is audible at the lower left sternal border

24
Left-to-Right Shunt Lesions
Electrocardiography With a small VSD, the ECG is normal. With a moderate VSD, left ventricular hypertrophy (LVH) and occasional left atrial hypertrophy (LAH) may be seen With a large defect, the ECG shows biventricular hypertrophy (BVH) with or without LAH
 and occasional left atrial hypertrophy (LAH) may be seen. With a large defect, the ECG shows biventricular hypertrophy (BVH) with or without LAH.")
28
Left-to-Right Shunt Lesions
X-ray Studies Cardiomegaly of varying degrees is present and involves the LA, left ventricle (LV), and sometimes RV. Pulmonary vascular markings increase. The degree of cardiomegaly and the increase in pulmonary vascular markings directly relate to the magnitude of the left-to-right shunt.
, and sometimes RV. Pulmonary vascular markings increase. The degree of cardiomegaly and the increase in pulmonary vascular markings directly relate to the magnitude of the left-to-right shunt.")
29
Left-to-Right Shunt Lesions

30
Left-to-Right Shunt Lesions
Echocardiography. Management Treatment of CHF, if it develops, is indicated with digoxin and diuretics for 2 to 4 months to see if growth failure can be improved. Surgical

31
Left-to-Right Shunt Lesions
Patent Ductus Arteriosus PDA occurs in 5% to 10% of all congenital heart defects, excluding premature infants. It is more common in females than in males (male/female ratio of 1:3). PDA is a common problem in premature infants
. PDA is a common problem in premature infants.")
32
Left-to-Right Shunt Lesions
PATHOLOGY : There is a persistent patency of a normal fetal structure between the left PA and the descending aorta, that is, about 5 to 10 mm distal to the origin of the left subclavian artery

33
Left-to-Right Shunt Lesions
CLINICAL MANIFESTATIONS Patients are usually asymptomatic when the ductus is small A large-shunt PDA may cause a lower respiratory tract infection, atelectasis, and CHF (accompanied by tachypnea and poor weight gain).
.")
34
Left-to-Right Shunt Lesions
Physical Examination Tachycardia and tachypnea may be present in infants with CHF Bounding peripheral pulses with wide pulse pressure The precordium is hyperactive. A systolic thrill may be present at the upper left sternal border. The P2 is usually normal, but its intensity may be accentuated if pulmonary hypertension is present. A grade 1 to 4/6 continuous (“machinery”) murmur is best audible at the left infraclavicular area or upper left sternal border
 murmur is best audible at the left infraclavicular area or upper left sternal border.")
36
Left-to-Right Shunt Lesions
Electrocardiography. The ECG findings in PDA are similar to those in VSD. A normal ECG or LVH is seen with small to moderate PDA. BVH is seen with large PDA. If pulmonary vascular obstructive disease develops, RVH is present

38
Left-to-Right Shunt Lesions
X-ray findings are also similar to those of VSD. Echocardiography MANAGEMENT Medical Indomethacin is ineffective in term infants with PDA and should not be used. Standard anticongestive measures with digoxin and diuretics are indicated when CHF develops

40
TOF

Similar presentations



















 tricuspid valve 2. Hypoplastic right ventricle 3. Ventricular septal defect 4. Atrial.>")








