Download presentation
Presentation is loading. Please wait.

1
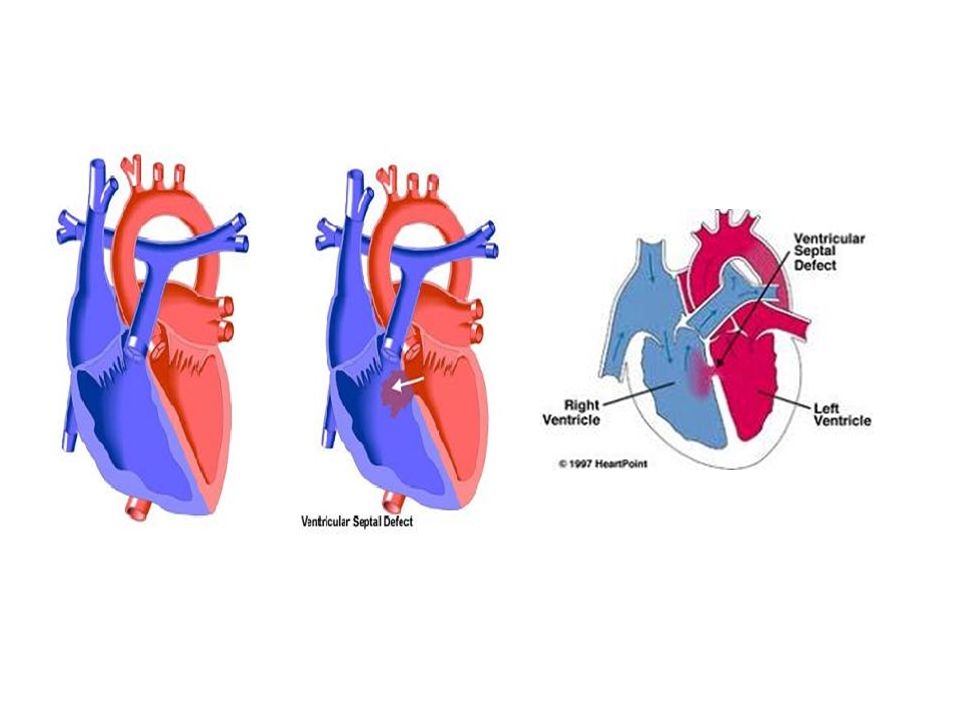
VENTRICULAR SEPTAL DEFECT (VSD)
It is a hole on interventricular septum Congenital or acquired

2
VENTRİKÜLER SEPTAL DEFEKT (VSD)
Congenital Acquired Isolated VSD can be seen in nearly 2 per live births. It is the most frequent congenital cardiac anomaly. can be associated with other anomalies. It is mostly seen as a complication of acute myocardial infaction. Rarely trauma is a cause .

4
VSD MORPHOLOGICAL CLASSIFICATION
Yerleşim Neighbourhood Perimembraneous %80 Subarterial %5-10 ( Juxta- arterial, conal, infundibular) Muscular %5 Inlet septal <%5 (AV kanal , AV septal) Tricuspid valve , conduction system (posteroinferior) Both semilunar valves ( Right coronary cusp) It is surrounded by muscle Conduction system (posteriorinferior)
 Muscular %5 Inlet septal <%5 (AV kanal , AV septal) Tricuspid valve , conduction system (posteroinferior) Both semilunar valves ( Right coronary cusp) It is surrounded by muscle. Conduction system (posteriorinferior)")
5
VSD MORFOLOJİK SINIFLAMA

7
VSD MORFOLOJİK SINIFLAMA

10
CLASS ACCORDING TO SIZE
VSD büyüklükleri; aort orifis çapına göre değerlendirilebildiği gibi VSD rezistans indekslerine (Rİ) göre de değerlendirilebilir. VSD Rİ = LVP - RVP x m2 Qp-Qs LVP= Sol ventrikül basıncı; RVP= Sağ ventrikül basıncı; Qp= Pulmoner kan akımı; Qs= Sistemik kan akımı; m2= Vücut alanı
 göre de değerlendirilebilir. VSD Rİ = LVP - RVP x m2. Qp-Qs. LVP= Sol ventrikül basıncı; RVP= Sağ ventrikül basıncı; Qp= Pulmoner kan akımı; Qs= Sistemik kan akımı; m2= Vücut alanı.")
11
VSD Large VSD Moderate VSD VSD diameter < Aort diameter RVP=1/2 LVP
VSD diameter ≥ Aortic diameter VSD Rİ < 20 Ü/m2 Resistance to flow is small RVP = LVP Qp/Qs ratio depends on degree of pulmonary vascular resistance (PVR). VSD diameter < Aort diameter RVP=1/2 LVP Qp/Qs≥2
. VSD diameter < Aort diameter. RVP=1/2 LVP. Qp/Qs≥2.")
12
VSD Small VSD VSD has not enough space to increase the right ventricular sistolic pressure. VSD Rİ>20Ü/m² Qp/Qs<1.75

13
Patients with large VSD and increased Qp/Qs Weak peripheral pulses
Symptoms and signs Patients with large VSD and increased Qp/Qs Weak peripheral pulses Tachypnea, subcostal drawings, profuse sweating Hepatomegaly, high jugular venous pressure, Difficulty in feeding, growth retardation

14
Large VSD and light PVR There is a strong pansystolic (holosystolic) murmur or thrill on the left parasternal region over the 3th ,4th intercostal space ( subarterial VSD on 2nd, 3th ICS), Apical diastolic murmur because of increased blood flow passing throughout th mitral valve. S2 is strong and splitted due to increased pulmonary flow.
 murmur or thrill on the left parasternal region over the 3th ,4th intercostal space ( subarterial VSD on 2nd, 3th ICS), Apical diastolic murmur because of increased blood flow passing throughout th mitral valve. S2 is strong and splitted due to increased pulmonary flow.")
15
Large VSD and high PVR Left to right shunt decreases and becomes bidirectional. Hyperactivity of the heart and cardiomegaly decrease. Pansytolic murmur change in character, becomes short and soft. Apical diastolic murmur is no more heard. S2 is forcefull. The patient becomes cyanotic If PVR>SVR. (Eisenmenger sendrome)
")
16
CHEST X-RAY Large VSD and light PVR Large VSD and high PVR

17
Patients with Moderate size VSD
Pansystolic murmur Light – moderate left and right ventricular enlargement.

18
small VSD There is harsh pansystolic murmur due to small VSD and shunt. EKG ve Chest X ray are normal.

19
Echocardiography: 2 Dimensional, colour Doppler ECHO Give us incredible information about the situation and size of the VSD QP/QS can be calculated. Associated anomalies like Aortic coarctation and PDA .

20
HEART CATHETERIZATION
To measure Pulmonary artery pressure, Left to right shunt and PVR To define the place, number and size of the VSD To show definitely the associatied anomalies.

21
SPONTANOUS CLOSURE Large VSD ; 1 month %80 3 month %60 6 month %50 12 month %25 spontaneous closure chance.

22
SPONTANOUS CLOSURE Less chance to close More chance to close
Perimembranous Juxta aortic Inlet septal Juxta-tricuspid Muscular (outlet)
")
23
COMPLICATIONS Pulmonary Vascular disease
Large VSD can have serious pulmonary resistance (Rp) in first 2 years of life
 in first 2 years of life.")
24
Pulmonary Vascular disease (Heath Edwards Classification)
Grade 1: Medial hyperthrophy. Grade 2: Medial hyperthrophy and intimal cellular proliferation Grade 3: Medial hyperthrophy and intimal fibrosis early generalized vascular dilatation Grade 4: Generalized vascular dilatation, vascular oclusions due to intimal fibrosis, plexiform lesions. Grade 5: Cavernous ve angiomatoid lesions. Grade 6: Necrotizing arteritis.

25
Infective Endocarditis
It is seen % of patient per year More often small and moderate VSDs Right sided vegetations (Tricuspid kapak) Lung infections Aortic insufficiency In the first decade % . Especially subarterial VSD
 Lung infections. Aortic insufficiency. In the first decade % . Especially subarterial VSD.")
26
Early Death 9 % of the patient with large VSD die within the 1st year.
PDA, Coarctation, large ASD Recurrent lung infections (Viral). Pulmonary edema (heart failure). After the first decade Eisenmenger complications (Hemoptisis, polycytemia, cerebral emboli, abscesses, right heart failure) 50% of patients die before 35 years of age.
. Pulmonary edema (heart failure). After the first decade Eisenmenger complications (Hemoptisis, polycytemia, cerebral emboli, abscesses, right heart failure) 50% of patients die before 35 years of age.")
27
Pulmonary Vascular Resistance
< 4 ünite m2 Normal < 5 ünite m mildly elevated < 8 ünite m moderately elevated > 8 ünite m severely elevated

28
INDICATIONS FOR OPERATION
Large VSD Every patient with intractable heart failure under medical treatment can be operated before 12 months. (Swiss cheese – Pulmonary banding) If there is growth failure or Rp >8ü m2 at 6 month, the operation should be performed.( If Rp < 4ü m2 , the operation can be deferred untill 12 month.) After infancy Rp is truely and precisely measured. If Rp < 8ü m patient can be operated, If Rp >8ü m2 , after isoproteronol perfusion remeasurement should be made If Rp ≤ 7ü m2 patient can be operated,
 If there is growth failure or Rp >8ü m2 at 6 month, the operation should be performed.( If Rp < 4ü m2 , the operation can be deferred untill 12 month.) After infancy Rp is truely and precisely measured. If Rp < 8ü m2 patient can be operated, If Rp >8ü m2 , after isoproteronol perfusion remeasurement should be made If Rp ≤ 7ü m2 patient can be operated,")
29
INDICATIONS FOR OPERATION
Moderate VSD If Ppa mmHg and Qp/Qs is about 3 Rp is rarely elevates and we can wait for operation untill 5 years of age. Small VSD İnfective endocarditis, ventrikül dysfunction is rarely seen (After 10 years of age)
")
30
SURGICAL TREATMENT Pulmonary banding
1-Swiss cheese septum with intractable heart failure Complications Hospital mortality is high Pulmonary stenosis, migration

31
PATCH CLOSURE Perikardial, Dacron and PTFE patches can be used for closure. Interrupted suture (Teflon pledgeted single) or continuous suture can be used. From the right atrium Perimembranous. From the right ventricle----- subarterial (Ventricular scar can cause RBBB, Arythmia yüksek)
 or continuous suture can be used. From the right atrium Perimembranous. From the right ventricle----- subarterial. (Ventricular scar can cause RBBB, Arythmia yüksek)")
32
Rigth Atrium

34
Continuous suture

35
Right Ventriculotomy

36
Interrupted suture

Similar presentations