Download presentation
Presentation is loading. Please wait.

1
Video Capsule Endoscopy Cem KALAYCI Marmara University Head, Dept. of Gastroenterology ESGAR, Istanbul 2008

2
Small Intestinal Capsule

3
Comparative Capsule Designs

4
VCE PillCam (PillCam SB). (Given Imaging; Yoqneam, Israel): FDA Approval 2000. EndoCapsule (Olympus): FDA Approval 2007 Similar characteristics to the PillCam SB but has a CCD chip instead of a CMOS chip.
: FDA Approval 2007 Similar characteristics to the PillCam SB but has a CCD chip instead of a CMOS chip..")
5
Given vs Olympus 51 patients with obscure GI bleeding PillCam SB and the EndoCapsule 40 minutes apart in randomized order Similar results for normal and abnormal Gastrointest Endosc 2007; 65:AB125.

6
CAPSULE ENDOSCOPY

7
The Diagnostic Process

8
Technics Two images per second 55,000 images over eight hours. Magnification 1:8 Review of the video, generation of a report: 30 to 90 minutes. Viewing: 1-25 frames per second (standard video speed).
..")
9
Primary Indications Obscure gastrointestinal bleeding Suspected Crohn's disease Small bowel tumors

10
Gastric Antral Vascular Ectasia (GAVE)
")
11
Angioectasia in Ileum

12
Aphthous Ulcers

13
Crohn’s Disease: Ulcers

14
Crohn’s Disease: Edema

15
Crohn’s Disease: Strictures

16
Gastrointestinal Stomal Tumors (GIST)
")
17
Other Indications NSAID injury to the small bowel Abdominal pain (functional vs organic) Celiac disease
 Celiac disease")
18
NSAID Ulceration

19
NSAID Stricture/Webs

20
Celiac Disease

21
Additional Applications Small bowel polyps Rejection in small bowel transplantation GVH diseaase after bone marrow transplantation Surveillance of patients with hereditary polyposis syndromes.

22
Advantages Noninvasive Examination of the majority of the small bowel mucosa, which is not possible with push enteroscopy Small bowel series, enteroclysis, and intra- operative enteroscopy are capable of examining the entire length of the small bowel, they are either quite insensitive or invasive.

23
Disadvantage No tissue sampling or therapeutic intervention.

24
Obscure Bleeding

25
Obscure Bleeding (100 patients) n Pos.Study (%) Ongoing overt bleeding 26 92 Previous overt bleeding 31 13 FOBT + and IDA43 44 Pennazio et al, Gastroenterology 2004;126:643.
 n Pos.Study (%) Ongoing overt bleeding Previous overt bleeding FOBT + and IDA43 44 Pennazio et al, Gastroenterology 2004;126:643.")
26
MOST COMMON FINDINGS Angioectasia (29 percent) Crohn's disease (6 percent). Diagnostic yield is highest when performed as close as possible to the bleeding episode. Pennazio et al, Gastroenterology 2004;126:643.

27
Obscure Bleeding Sixty-two patients underwent further examination that led to independent verification of the diagnosis in 56. Sensitivity: 89 %, Specificity: 95 % PPV: 97 % NPV: 83 % Ongoing obscure bleeding (overt or occult) are the best candidates Pennazio et al, Gastroenterology 2004;126:643.
 are the best candidates Pennazio et al, Gastroenterology 2004;126:643..")
28
Video Capsule Endoscopy vs Push Enteroscopy in the Diagnosis of Obscure GI Bleeding

29
Yield in Obscure bleeding A meta-analysis of 14 studies: Capsule endoscopy: (63 percent) Push enteroscopy (26 percent), Barium studies (8 percent) Triester, SL et al. Am J Gastroenterol 2005; 100:2407.

35
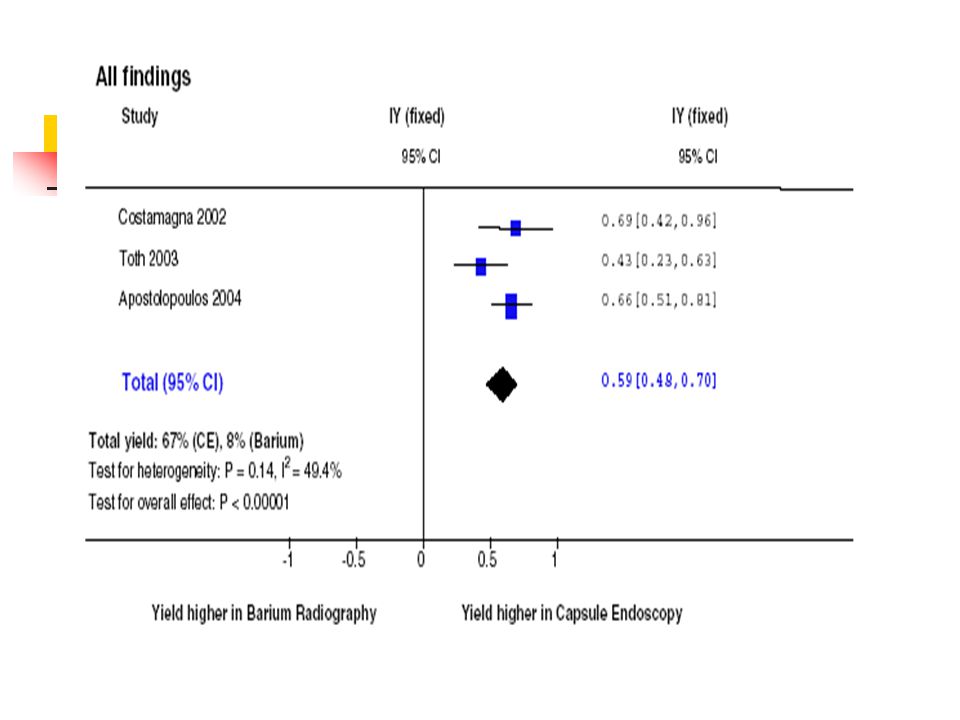
VCE vs SBFT 22 patients suspected of having small bowel pathology, underwent both VCE and SBFT. Diagnostic study: VCE: 45 % SBFT: 20 % Finding the cause of Obscure bleeding: VCE: 31% SBFT: 5 % Costamagna, G, et al. Gastroenterology 2002;123:999.

36
Hadithi M, et al. Am J Gastroenterol 2006:100 :1-6

37
VCE vs DBE Diagnosing the etiology: VCE: 80 % DBE: 60 % A procedure/treatment was performed in 77 % of the patients with DBE 74 % of the patients remained stable during 5 month follow up Hadithi M, et al. Am J Gastroenterol 2006:100 :1-6

38
Crohn’s Disease

39
nVCEPush Entero Crohn’s 22 17 3 4 Suspected CD 21 4* 0 1 (false) *2 were false diagnosis Chong et al, Gastrointest Endosc 2005;61:255-61
 *2 were false diagnosis Chong et al, Gastrointest Endosc 2005;61:255-61")
40
Crohn’s Disease VCE detected more erosions than push entero and enteroclysis (p<0.001) There was no difference in patients with suspected Crohn’s disease. Capsule endoscopy had a higher yield than push enteroscopy and enteroclysis in patients with known Crohn's disease Chong et al, Gatsrointest Endosc 2005;61:255-61 Marmo, R, et al. Clin Gastroenterol Hepatol 2005; 3:772.

41
Video Capsule Endoscopy and the Diagnosis of Suspected Crohn’s Disease

42
VCE vs Barium in suspected Crohn’s recurrence Studies produced complementary results VCE: Mucosal disease in six patients with a normal SBFT SBFT: Grade 1 mucosal disease in five patients with a normal VCE study. Buchman, AL, et al. Am J Gastroenterol 2004; 99:2171.

43
Risk: Retention of the capsule Clinically important retention < 1 %. Patients with increased risk known or suspected Crohn's disease intermitent SB obstruction secondary to adhesions radiation enteritis severe motility disorders Zenker's diverticulum. A normal barium study or CT scan does not exclude the possibility of retention.

44
Capsule Retention Palpation by the surgeon of the capsule retained above a stricture may be helpful in localizing the stricture, which may have no serosal signs, thus avoiding the need for intra-operative enteroscopy. Removal of the retained capsule by double balloon enteroscopy has also been described

45
Patency capsule Same size as the PillCam Composed of lactose and barium Contains a radiofrequency identification tag that allows it to be detected by a scanning device Dissolves in 40 to 80 hours after ingestion.

46
Patency capsule To assure small bowel patency before VCE Diagnostic test for suspected small bowel strictures that cannot be identified by standard radiographic means. 25 percent of patients with strictures developed abdominal pain, some severe, and two patients required emergency surgery Delvaux, M, V, et al. Endoscopy. 2005; 37:801.

48
Contraindications Dementia Gastroparesis (the capsule can be placed in the duodenum by endoscopy) Esophageal stricture, swallowing disorders (eg, Zenker's diverticulum) (endoscopic placement)
 Esophageal stricture, swallowing disorders (eg, Zenker s diverticulum) (endoscopic placement)")
49
Partial or intermittent small bowel obstruction Those who are inoperable or refuse surgery Patients who have defibrillators or pacemakers. This is a recommendation in the package insert, but does not appear to be a significant clinical problem. Contraindications

50
Thank you.....

51
OGIB:VCE Prior to Push Enteroscopy (PE) 89 patients VCE before PE is a more effective strategy than beginning with push enteroscopy 12 months follow up VCE first followed by PE vs PE followed by VCE as needed had similar diagnostic yields. VCE first strategy reduced the percentage of patients needing the alternative study (25% vs 79%). de Leusse, A, et al. Gastroenterology 2007; 132:855.
. de Leusse, A, et al. Gastroenterology 2007; 132:855..")
52
We suggest proceeding directly with VCE in those in whom EGD and colonoscopy have been unrevealing. Preliminary evidence suggest a higher diagnostic yield in those studied with recent bleeding. (See "Efficacy" above).See "Efficacy" above In those in whom a lesion is detected within reach of the push enteroscope, we suggest proceeding with push enteroscopy with the intention of treating or tattooing the lesion (or both). Treatment is more difficult in those with a lesion beyond the reach of the enteroscope. Surgery, medical treatment, or angiography may be appropriate depending upon the clinical setting. We proceed with angiography in those in whom VCE is unrevealing and patients continue to require transfusion. We have not found intra-operative enteroscopy to be helpful after a negative VCE. Such patients often have punctate bleeding sites or Dieulafoy's lesions, which are unlikely to be found unless they continue to bleed during the procedure. Provocation of bleeding during angiography (with anticoagulants) to help identify the bleeding site has been described, but the safety and efficacy of this approach is uncertain [65].65
.See Efficacy above In those in whom a lesion is detected within reach of the push enteroscope, we suggest proceeding with push enteroscopy with the intention of treating or tattooing the lesion (or both). Treatment is more difficult in those with a lesion beyond the reach of the enteroscope. Surgery, medical treatment, or angiography may be appropriate depending upon the clinical setting. We proceed with angiography in those in whom VCE is unrevealing and patients continue to require transfusion. We have not found intra-operative enteroscopy to be helpful after a negative VCE. Such patients often have punctate bleeding sites or Dieulafoy s lesions, which are unlikely to be found unless they continue to bleed during the procedure. Provocation of bleeding during angiography (with anticoagulants) to help identify the bleeding site has been described, but the safety and efficacy of this approach is uncertain [65].65.")
53
Normal Variants: Pylorus

54
Barrett’s Esophagus

55
Occult GI Bleeding) More effective than push enteroscopy Finding the cause 50-70 % Gastrointest Endosc 2002;56:349, 2002;55AB88, AB128 Am J Gastro 2002;97:S299, 2002;97:S299 Endoscopy 2002;34:685 Gut 2003;52:1122, Gastrointest Endosc 2004;59:492, APT2004;20:189
 More effective than push enteroscopy Finding the cause % Gastrointest Endosc 2002;56:349, 2002;55AB88, AB128 Am J Gastro 2002;97:S299, 2002;97:S299 Endoscopy 2002;34:685 Gut 2003;52:1122, Gastrointest Endosc 2004;59:492, APT2004;20:189")
56
Radiation Injury

Similar presentations