Download presentation
Presentation is loading. Please wait.

1
Nutrition & the Politics of Famine International Development & Health Hilary Term 2009 Proochista Ariana

2
Overview Nutritional transitions with economic growth Anthropometry Famine Theories Famine Response

3
Points for Reflection What does anthropometry tell us about health? How can political, economic, or social factors help explain the dynamic changes in nutrition? To what extent are famines today a consequences of natural phenomena?

4
Epidemiological Transition?

5
Double Burden of Disease Concurrence of both communicable and non- communicable diseases Infection is responsible for 25% of cancers in the developing world compared with 10% in the developed world

6
Triple Burden of Disease Communicable, non-communicable, and socio-behavioural Increasing recognition of burden of mental illnesses Aging population and chronic diseases of lifestyle Tobacco: “By 2020, tobacco is expected to kill more people than any single disease, even HIV/AIDS”

7
Source: Global Burden of Disease 2004

10
5 stage model of Epi Transition StageCharacteristics Age of pestilence and famineInfectious and nutritional related cardiomyopathies; Rheumatic heart disease Age of receding pandemicsHypertensive cardiovascular disease Haemorrhagic strokes Age of degenerative and man-made diseases Haemorrhagic and ischemic stoke, ischemic heart disease, diabetes and obesity Onset at younger age Age of delayed degenerative diseasesAtherosclerotic cardiovascular disease; Onset of chronic disease at older ages – delay occurs due to improved prevention and treatment Age of health regression and social upheaval Social upheaval causes an increase in the prevalence of chronic disease at younger ages; Re-emergence of mortality due to infectious disease and rheumatic heart disease Source: Yusuf et al., (2001)
")
11
Delayed Degenerative Diseases The age of delayed degenerative disease is characterised by an increase in the average life expectancy and an increase in the age of onset for chronic disease. This stage includes regions with relatively advanced health care systems such as North America, Australia and Western Europe illustrate this stage

12
Health Regression & Social Upheaval re-emergence of mortality due to communicable disease in addition to non- communicable disease Average life expectancy decreases and an increase in the prevalence of non- communicable diseases is seen at younger ages

13
Social Determinants conditions in which people are born, grow, live, work, and age access to health care, schools and education, their conditions of work and leisure, their homes, communities, towns, or cities unequal living conditions are the consequence of poor social policies and programmes, unfair economic arrangements, and bad politics

14
Conditions of Life Different Exposures to disease-causing influences in early life Different Vulnerabilities Differences in ability to cope (material, psychosocial, behavioural)
")
15
Nutrition Transition

16
Nutrition Measures Anthropometric – Weight-for-height (wasting) – Height-for-age (stunting) – Body mass index – Adult height Dietary consumption Micronutrient levels
 – Height-for-age (stunting) – Body mass index – Adult height Dietary consumption Micronutrient levels")
17
Under-Nutrition Physical and mental lethargy Compromised immune system and increased susceptibility to infections Increased frequency and/or severity of morbidities and enhanced risk of mortality Compromised cognitive development

18
Over-Nutrition Blood pressure, cholesterol, triglycerides, and insulin Type 2 Diabetes Cardiovascular diseases and fatalities Cancer of the breast, colon, prostrate, endometroium, kidney and gallbladder Contributes to osteoarthritis, respiratory difficulties, musculoskeletal problems, infertility

19
Nutrition Transition Source: Mike Rayner (WHO, SDE/NHD, 2000)
")
20
Nutrition Transition 1.Hunting & gathering: Plants, low-fat wild animals; varied diet 2.Famine: Cereals predominant; diet less varied 3.Receding famine: Fewer starchy staples; more fruits, vegetables, animal protein; low variety 4.Degenerative disease: More fat, sugar & processed foods; less fibre 5.Behavioural change: Less fat and processing; increased carbohydrates, fruits and vegetables

21
Shifts in Diets increases in the consumption of foods sourced from animals, caloric sweeteners and fat Between 1970 and 1995 the world consumption of calories from starchy roots and pulses fell by 30% while the proportion of calories from meat increased by a third and from vegetable oils by almost half Over the same period the consumption of meat and poultry doubled in Asian countries while the consumption of vegetables halved

24
Source: Pomerleau et al 2002

25
Physical Activity shifts away from physically demanding economic activities (e.g. farming, mining and forestry) towards more sedentary activities (e.g. office based, assembly lines) Technological innovation leads to decreased activity in previously physically demanding jobs Leisure activities are increasingly sedentary in nature
 towards more sedentary activities (e.g. office based, assembly lines) Technological innovation leads to decreased activity in previously physically demanding jobs Leisure activities are increasingly sedentary in nature.")
26
Global Obesity Epidemic According to the WHO, over 1 billion adults are overweight, 300 million of whom are obese Obesity ranges from under 5% in China to over 75% in urban Samoa 17.6 million children under five are estimated to be overweight worldwide In the US, the number of overweight children has doubled and the number of overweight adolescents has trebled since 1980

27
Global Distribution of Obesity Source: WHO

28
Source: World Health Organisation (2006) Global Health Atlas * Data for latest year available
 Global Health Atlas * Data for latest year available")
29
Increase in Obesity in many developing regions obesity prevalence is outstripping rates in the developed world The rate of increase in obesity among adults in Asia, North Africa and Latin America are between two and five times of the rate of increase in Northern America

30
Income and Overweight Wang et al, 2002

31
Trends in Childhood Obesity Source: Anderson 2005

32
Trends in Overweight Children

33
Shift from Under to Over-weight Source: Wang et al 2002

34
Under- and Over-Weight Source: Wang et al 2002

35
China (1991-2004) Source: Dearth-Wesley et al 2008
 Source: Dearth-Wesley et al 2008")
36
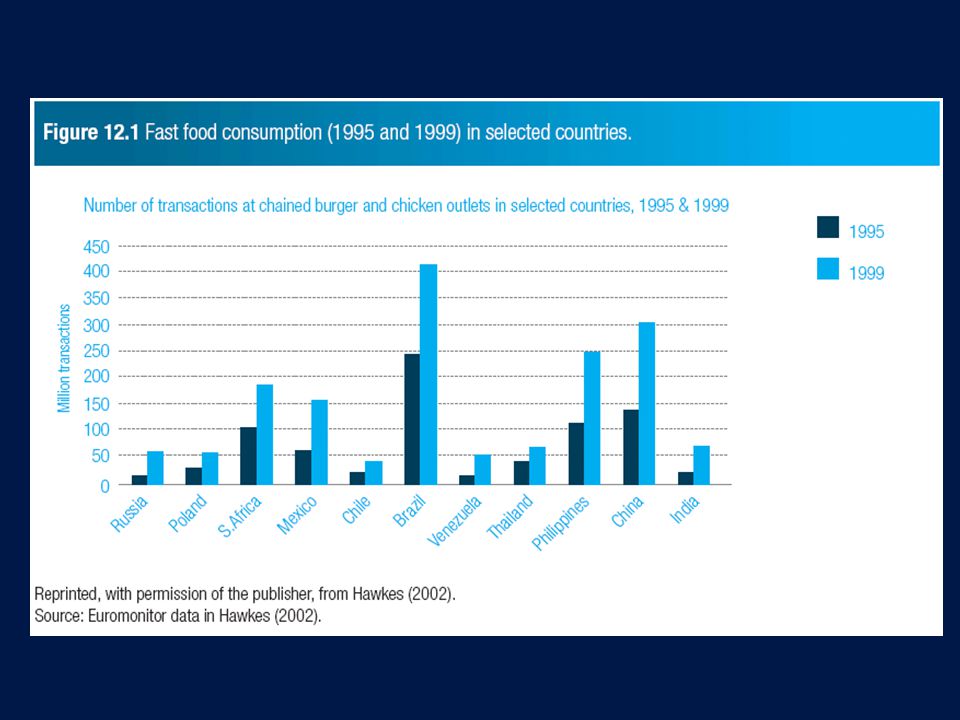
Transition to Obesity Shift to Western dietary habits and a proliferation of fast-food chains Higher energy-dense foods, larger portion size and an increase in the consumption of sugar rich soft drinks In combination with increasingly automated and sedentary lifestyles

37
Fast Food Chains Between 1970 and 1980, the number of fast-food outlets in the United States increased from about 30,000 to 140,000, and to about 222,000 in 2001 (Source: Paeratakul S, Ferdinand D, Champagne C, Ryan D, Bray G. Fast-food consumption among US adults and children. J Am Diet Assoc 2003:103:1332-8)
.")
38
Transition? Nutrition related non-communicable disease risk among the well off population appear concurrent with simultaneous persistence of under-nutrition and low food security among the poorer populations of the same country

39
Double Burden Households Doak et al, 2005

40
Anthropometry

41
Anthropometric Measures Weight-for-Height: An indicator of acute malnutrition or ‘wasting’ Height-for-Age: An indicator of chronic malnutrition or ‘stunting’ Weight-for-Age: one of the first measures of nutritional status and remains the measure most closely correlated to fatal health (Gomez et al 1956)
")
42
Cut offs States of malnutrition are classified using WHO’s recommended two standard deviation cut-off points: “In general, abnormal anthropometry is statistically defined as an anthropometric value below -2 standard deviations (SD) or Z-scores ( 97.7 th percentile) relative to the reference mean or median. These cut-offs define the central 95% of the reference distribution as the “normality” range” (WHO, 1995 p.181).
..")
43
International Standard 1978 National Center for Health Statistics (NCHS) reference curves for height-for-age, weight-for-age, and weight-for-height Sample of American formula-fed infants Restricted socio-economic and genetic background Intervals of measurement preclude precise curve fitting Positively skewed weight distribution
 reference curves for height-for-age, weight-for-age, and weight-for-height Sample of American formula-fed infants Restricted socio-economic and genetic background Intervals of measurement preclude precise curve fitting Positively skewed weight distribution")
44
NCHS versus WHO Standards Source: de Onis 2006

45
Categories of Undernutrition Stunting: “the process of failure to reach linear growth potential as a result of inadequate nutrition and/or public health”; Wasting: “describes a recent or current severe process leading to significant weight loss, usually as a consequence of acute starvation and/or disease” Underweight: is simply defined as “low weight for age”

46
Stunting WHO contrasts stunting with shortness which they define as “a descriptive term for low height-for-age, without implication of cause” (WHO, 1995 p.422) “a high prevalence of low height-for-age indicates poor nutrition, high morbidity from infectious disease, or-most often-both” (WHO)
 a high prevalence of low height-for-age indicates poor nutrition, high morbidity from infectious disease, or-most often-both (WHO)")
47
Wasting “A high prevalence of low weight-for-height is indicative of severe recent or current events, for example starvation or outbreaks of infectious diseases such as diarrhoea or measles” (WHO, 1995 p.181).
.")
48
Body Mass Index Underweight<18.50 Severe thinness<16.00 Moderate thinness16.00 - 16.99 Mild thinness17.00 - 18.49 Normal range18.50 - 24.99 Overweight≥25.00 Pre-obese25.00 - 29.99 Obese≥30.00 Obese class I30.00 - 34-99 Obese class II35.00 - 39.99 Obese class III≥40.00

49
Proxy for Malnutrition Initially anthropometry was developed and applied as an easy way to approximate clinical malnutrition in the field Changes in body composition signify one manifestation of malnutrition which can be readily measured Anthropometry alone is insufficient to define malnutrition (which requires clinical assessment) Rather it identifies individuals at greater risk for malnutrition (Trowbridge FL, 1979)
 Rather it identifies individuals at greater risk for malnutrition (Trowbridge FL, 1979)")
50
Validity Relies on evidence linking outward expression of stature to physiological processes Concurrent validity: the ability of the anthropometric measures to correspond to clinical assessments of malnutrition Predictive validity: the ability of the indicator to predict future morbidity and mortality

51
Other Implications Even without extra susceptibility to disease, stunting or wasting or overweight may have consequences for: – Energy – Productivity – Feelings of well-being – Shame, humiliation or pride & self-confidence – Quality of life

52
Causes versus Consequences Causes: Factors that could explain current nutritional states (nutritional intake, activity, illness, stress, etc.) Consequences: Risks that could emerge from the nutritional states (illness, cognitive impairment, educational attainment, income- earning potential)
 Consequences: Risks that could emerge from the nutritional states (illness, cognitive impairment, educational attainment, income- earning potential)")
53
Childhood stunting, severe wasting, and underweight 2005 Black et al, 2008

54
Prevalence of Childhood Stunting (Source: de Onis et al 2000)
")
55
Trends in Stunting (Source: de Onis et al 2000)
")
56
Consequences of Stunting Childhood height-for-age related to adult height Stunting predicts poorer cognitive performance and/or lower school grades attained in middle childhood Early childhood stunting associated with adult BMI and central adiposity Early childhood stunting associated with risk of having a LBW infant

57
Height-for-age and attained height Victora et al, 2008

58
Height-for-age and attained schooling Victora et al, 2008

59
Global deaths and disease burden attributable to undernutrition Black et al, 2008

60
Height

61
Trends in Height Baten: Working Paper

62
Heights in Africa Baten, Working Paper

63
Contributing Factors National income or Political system Proximity to protein sources Price of food Disease environment Dietary Customs Genetic (intergenerational transmission of height) Elevation or types of activities
 Elevation or types of activities")
64
Height and GDP Baten, Working Paper

65
Consequences Cognitive capacity Employment opportunities Income earnings Morbidity & Mortality (?) Low birthweight
 Low birthweight")
66
Height and IQ Height at age 9 years a significant predictor of childhood IQ after adjusting for socioeconomic status Height at age 13 a significant predictor of IQ after adjusting for socioeconomic status Height at age 13 also explained an additional 2.5% of the variation in IQ scores to that already explained by socioeconomic status and height at age nine. Pearce et al, 2005

67
Height, Ability and Labour Markets A large and significant association between height and test scores for children followed in the British Cohort Study (BCS) for tests they took at ages 5 and 10 and for children in the National Child Development Survey (NCDS) for tests at ages 7 and 11. Economic returns to height are the result of correlation between height and cognitive ability - a correlation that is evident early in life and remains throughout. Case et al, 2006

68
Height and Labour Market Outcomes Persico et al, 2004 In the past 13 US presidential elections, the taller candidate has won 10 times (the most recent exception being George W. Bush)
.")
69
Height and Labour Market Outcomes Data from Britain’s National Child Development Survey(NCDS) showed that among white British men every additional inch of adult height is associated with a 2.2 percent increase in wages. Data from the US National Longitudinal Survey of Youth (NLSY) showed that among adult white males in the US, every additional inch of height as an adult is associated with a 1.8 percent increase in wages. The tallest quarter of the population has a median wage that is more than 13 percent higher than that of the shortest quarter. Persico et al, 2004
 showed that among adult white males in the US, every additional inch of height as an adult is associated with a 1.8 percent increase in wages. The tallest quarter of the population has a median wage that is more than 13 percent higher than that of the shortest quarter. Persico et al,")
70
Height on Workplace Success and Income For every inch of height increase amounts to a salary increase of about $789 annually Judge et al, 2004

71
Macronutrients and Micronutrients

72
Total Energy Malnutrition: Marasmus Caused by inadequate intake of protein and calories Presents as decreased activity, lethargy, behavioural changes, slowed growth and weight loss Subsequent effects on the body are wasting and a loss of subcutaneous fat and muscle, resulting in growth retardation. CDC Public Health Image Library

73
Protein Energy Malnutrition: Kwashiorkor Caused by inadequate protein intake Characterised by failure to gain weight, generalised oedema, protuberant (swollen) abdomen, diarrhea, skin desquamation (peeling) and vitiligo (white spots on the skin)
 abdomen, diarrhea, skin desquamation (peeling) and vitiligo (white spots on the skin)")
74
Vitamin A Thiamin Riboflavin NiacinFolate Manganese Magnesium Iron Iodine CobalaminCobaltZinc Vitamin C Vitamin E Vitamin D Vitamin K Vitamin B 6 Vitamin B 12 Selenium Chromium Phosphorus ….are endemic almost throughout the world including in most emergency-affected populations….

75
Iron Deficiency Feeling tired and weak Decreased work and school performance Slow cognitive and social development during childhood Difficulty maintaining body temperature Decreased immune function, which increases susceptibility to infection

76
Anemia in Pre-schoolers WHO, 2008

77
Anemia in Pregnant Women WHO, 2008

78
Anemia in Women of Reproductive Age WHO, 2008

79
Sources of Iron Dried beans; Dried fruits Eggs (especially egg yolks) Liver Lean red meat (especially beef) Oysters Poultry Salmon Tuna Whole grains Iron-fortified cereals Iron from vegetables, fruits, grains, and supplements is harder for the body to absorb. Dried fruits: prunes, raisins, apricots, Legumes: lima beans, soybeans, dried beans and peas, kidney beans, Seeds, almonds, Brazil nuts; Vegetables: broccoli, spinach, kale, collards, asparagus, dandelion greens; Whole grains: wheat, millet, oats, brown rice If you mix some lean meat, fish, or poultry with beans or dark leafy greens at a meal, you can improve absorption of vegetable sources of iron up to three times.

80
Vitamin A Deficiency Bitot spots - areas of abnormal squamous cell proliferation and keratinization of the conjunctiva Night blindness Blindness Dry skin, dry hair, pruritus, broken fingernails

81
Distribution of Vitamin A Deficiency WHO, 2004

82
Prevalence of vitamin A deficiency in children <5 Black et al, 2008

83
Sources of Vitamin A http://ods.od.nih.gov/factsheets

84
Iodine Deficiency Goiter Hypothyroidism Cretinism Mental retardation

85
Distribution of Iodine Deficiency WHO, 2004

86
Sources of Iodine Iodized salt Seafood is naturally rich in iodine; Cod, sea bass, haddock, and perch are good sources. Kelp is the most common vegetable seafood that is a rich source of iodine. Dairy products also contain iodine. Other good sources are plants grown in iodine-rich soil.

87
Scurvy - Vitamin C deficiency Fatigue swollen and bleeding gums Haemorrhage slow healing of wounds populations with no access to fruit and vegetables or entirely reliant on rations as source of food

88
Vitamin C Sources All fruits and vegetables contain some amount of vitamin C. Foods that tend to be the highest sources of vitamin C include green peppers, citrus fruits and juices, strawberries, tomatoes, broccoli, turnip greens and other leafy greens, sweet and white potatoes, and cantaloupe. Other excellent sources include papaya, mango, watermelon, brussels sprouts, cauliflower, cabbage, winter squash, red peppers, raspberries, blueberries, cranberries, and pineapples.

89
Zinc deficiency Zinc deficiency is characterized by growth retardation, loss of appetite, and impaired immune function. In more severe cases, zinc deficiency causes hair loss, diarrhea, delayed sexual maturation, impotence, hypogonadism in males, and eye and skin lesions. Weight loss, delayed healing of wounds, taste abnormalities, and mental lethargy can also occur.

90
National risk of zinc deficiency in children <5 Black et al, 2008

91
Zinc Sources High-protein foods contain high amounts of zinc. Beef, pork, and lamb contain more zinc than fish. The dark meat of a chicken has more zinc than the light meat. Other good sources of zinc are peanuts, peanut butter, and legumes.

92
Famines

93
Caloric Needs For basal metabolic activities For physical or mental exertion For growth (children and pregnant women) For immune response (Gender and age differences in requirements)
 For immune response (Gender and age differences in requirements)")
94
Food Shortage How many days can we go without food? How many days can we go without water?

95
Adaptive Processes Metabolic: efficiency with which convert food to energy Physiological: prioritise vital organs – Blood glucose – Fat stores – Break down muscle mass (wasting) – Compromised linear growth (stunting) Socio-behavioural: activities
 – Compromised linear growth (stunting) Socio-behavioural: activities")
96
Infection- Undernutrition Cycle Undernutrition compromises immune system Infection exacerbates undernutrition by – Decreasing absorption of nutrients – Decreasing appetite – Increasing demand for energy

97
Starvation Long process (not a static state) Loss of body mass Weakness and lethargy Compromised temperature regulation Irritability, lack of concentration Immune deficiency Anaemia and manifestation of other micro- nutrient deficiencies
 Loss of body mass Weakness and lethargy Compromised temperature regulation Irritability, lack of concentration Immune deficiency Anaemia and manifestation of other micro- nutrient deficiencies")
98
Social interpretations Deprivation on a mass scale in multiple spheres: – Sociability – Various dimensions of satisfaction What are some local words for starvation or famine?

99
But what is Famine?

100
“ There is still a major controversy over whether the Ethiopia crisis of 1999-2000 should be labeled a “ famine ” or not, in light of the emotive and political connotations of the word. In the author ’ s view - given the number of people affected, the damage to livelihoods and human development, and the loss of human life - there is no question about whether Ethiopia 1999-2000 was a famine. But the continued controversy over this issue points to the need for a broadly accepted operational definition of famine. ” Maxwell, 2005

101
Theoretical Definitions “ In statistical terms, [famine] can be defined as a severe shortage of food accompanied by a significant increase in the local or regional death rate. ” (Mayer, 1975: 572) “ Famine is a socio-economic process which causes the accelerated destitution of the most vulnerable, marginal and least-powerful groups in a community, to a point where they can no longer, as a group, maintain a sustainable livelihood. Ultimately, the process leads to the inability of the individual to acquire sufficient food to sustain life. ” (Walker, 1989: 6)
![Theoretical Definitions In statistical terms, [famine] can be defined as a severe shortage of food accompanied by a significant increase in the local or regional death rate.](http://images.slideplayer.com/15/4571171/slides/slide_101.jpg "(Mayer, 1975: 572) Famine is a socio-economic process which causes the accelerated destitution of the most vulnerable, marginal and least-powerful groups in a community, to a point where they can no longer, as a group, maintain a sustainable livelihood. Ultimately, the process leads to the inability of the individual to acquire sufficient food to sustain life. (Walker, 1989: 6).")
102
Useful? “ Most definitions merely provide ‘ a pithy description ’ of what happens during famines, rather than ‘ helping us to do the diagnosis - the traditional function of a definition ’. ” (Sen 1981: 40)
.")
103
Indian Famine Codes (1880s) Codify administrative responses to food crises Three levels of food stress: near scarcity, scarcity and famine Scarcity was defined as “prevailing want of food or other necessaries”, while famine was “the aggravation of conditions of scarcity into a state of extreme scarcity” (Singh, 1993: 149). Scarcity was identified by: three successive years of crop failure; crop yields of four to six annas (compared to a normal yield of 12 annas); and large populations in distress. The declaration of famine was based on additional criteria, including: food price rises above the “scarcity rate” (defined as 40 per cent above the “normal price”), signs of increased migration and the extent of mortality.
; and large populations in distress. The declaration of famine was based on additional criteria, including: food price rises above the scarcity rate (defined as 40 per cent above the normal price ), signs of increased migration and the extent of mortality..")
104
Early Warning Systems Historical precedents of Famine Codes using various food security indicators developed after the mid- 1980s famines in Sub-saharan Africa. Context-specific food security indicators are monitored and analysed as to whether current conditions qualifies as a potential or actual crisis “indicators of vulnerability, of imminent crisis, of famine” (Cuny, 1999) complemented by anthropometric data, where available, to assess severity of food situation
 complemented by anthropometric data, where available, to assess severity of food situation.")
105
Coping Strategies as Indicators Generalisable patterns and sequences of behavioural responses of populations affected by food crises used as indicators Stage a: includes strategies for overcoming ‘ normal seasonal stress ’, such as rationing food or diversifying income. Stage b: food stress is prolonged, increasingly irreversible strategies - such as selling breeding livestock or mortgaging land which trade short-term gain for long- term problems (discounting) Stage c: dependence on external support such as food aid Stage d: starvation and death
 Stage c: dependence on external support such as food aid Stage d: starvation and death.")
106
Nutrition Surveillance

107
Famine Highly politicized label When is a ‘famine’ declared and who decides? Incentives or disincentives to declare What are the information needs and how reliable are information sources?

108
Famine Theories Food Availability Decline (FAD) Food Entitlement Decline (FED) Market Failure Concatenation Process
 Food Entitlement Decline (FED) Market Failure Concatenation Process")
109
Food Availability Decline Supply theory of famine Shortage of food Assessed through estimation of – Food production (+) – Imports (+) – Exports (-) – Wastage (-) – grain needed for sowing (-) – residual stocks (+)
 – Imports (+) – Exports (-) – Wastage (-) – grain needed for sowing (-) – residual stocks (+)")
110
Relevance of FAD Equation Closed Systems – Remote regions, environmentally hostile & isolated regions, islands – Sanctions, economic blockades, or conflict Reliance on local Production

111
Causes of FAD Drought or floods Diseases of plants or animals Declines in soil productivity Conflict Government policies (e.g. cash cropping) Regulations on land use Trade regulations Alternative use of agricultural production (e.g. Food as fuel)
 Regulations on land use Trade regulations Alternative use of agricultural production (e.g. Food as fuel).")
112
Food Entitlement Decline Demand theory of famine Failure to demand even when supply sufficient Types of entitlements (entitlement set): – Ownership – Exchange – Non-market Relationship between non-food and food prices Famine may result form a change in the price of key items in the entitlement set
: – Ownership – Exchange – Non-market Relationship between non-food and food prices Famine may result form a change in the price of key items in the entitlement set")
113
Market Failures Imperfect system of distribution – Infrastructure – Transport (ownership, repair, alternative uses) Physical fragmentation – Transaction costs & risks (physical isolation, imperfect information) Speculation and hoarding – Collusion of merchants to artificially limit supply in order to increase costs and profits
 Physical fragmentation – Transaction costs & risks (physical isolation, imperfect information) Speculation and hoarding – Collusion of merchants to artificially limit supply in order to increase costs and profits")
114
Modern Famines Complex combinations of many factors including FAD and FED and market failures Conflicts and/or sanctions HIV/AIDS FAD may lead to FED by leading to unemployment and consequent price scissors – Price of goods sold by poor ↓ (supply ↑ demand↓) – Price of goods bought by poor ↑ (supply ↓ demand↑)
 – Price of goods bought by poor ↑ (supply ↓ demand↑)")
115
Food Waste Today, over one third of the world's cereals are being used as animal feed (UNEP, 2009) Currently an estimated 30 million tons of fish are discarded at sea annually Losses and food waste in the United States could be as high as 40-50 per cent, according to some recent estimates Up to one quarter of all fresh fruits and vegetables in the US is lost between the field and the table
 Currently an estimated 30 million tons of fish are discarded at sea annually Losses and food waste in the United States could be as high as per cent, according to some recent estimates Up to one quarter of all fresh fruits and vegetables in the US is lost between the field and the table")
116
Food Waste Almost one-third of all food purchased in the United Kingdom every year is not eaten in Africa, the total amount of fish lost through discards, post-harvest loss and spoilage may be around 30 per cent of landings Food losses in the field between planting and harvesting could be as high as 20-40 per cent of the potential harvest in developing countries (source: UNEP 2009)
")
117
Policy Response to Famine Reformism (deliberate relief policy) Mild interventionist (emergency relief) Non-interventionist Radical non-intervention
 Mild interventionist (emergency relief) Non-interventionist Radical non-intervention")
118
Reformism Often integrated with development policies Idea that markets insufficient so need long- term policies offering state-welfare – Institutions – Employment – Food distribution Hope to decrease vulnerability to such disasters

119
Reformism Post disaster rehabilitation – Assets – Credit – food Institutional Support – Public/state distribution of subsidised grains – Food for work – Employment guarantees Medium-term reforms – Soil and water conservation efforts – Land reform – Agricultural technology

120
Mild Interventionists Markets necessary but not sufficient Relief only at times of acute starvation Early warning systems Nutritional surveillance and food balance sheets Satellite facilitated crop forecasting Supplementary feeding & rationing (food, water, fodder) Medical relief Loans, ↓taxes, public employment
 Medical relief Loans, ↓taxes, public employment")
121
Libertarian Non-Interventionism Competitive, integrated markets necessary and sufficient to deal with famines. Famine relief interferes with markets and creates inefficiency Population is regulated via the market to the level of the available means of subsistence. Relief distorts this process Relief misused by elites for their own ends and perpetuates exploitive economic arrangements Geo-political motivations

122
Radical Non-Intervention Markets unnecessary and insufficient Mechanisms of inequality which under- develops the poor Immiserisation conscientises (if you let things get really bad, people will make them right)
")
123
Thank You

124
Accidents and Injuries

125
Road Traffic Accidents Road traffic accidents rank as the 11th leading cause of death and account for 2.1% of all deaths globally – kill 1.2 million people a year or an average – injure or disable between 20 million and 50 million people a year 90% of road traffic deaths occur in low-income and middle-income countries

127
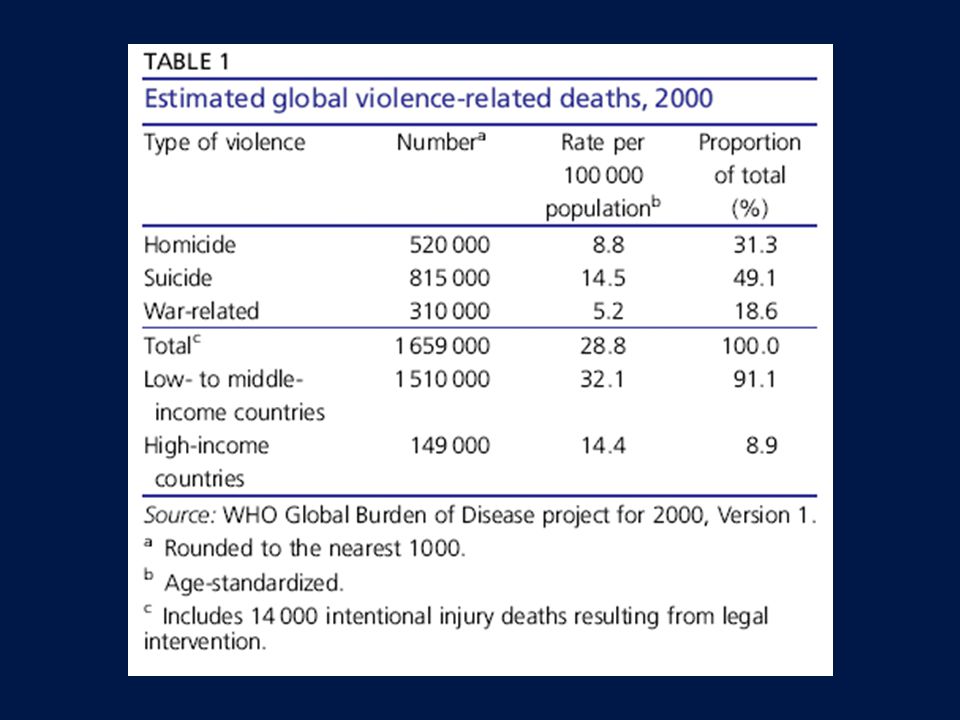
Violence Each year, more than 1.6 million people worldwide lose their lives to violence Violence is among the leading causes of death for people aged 15–44 years worldwide, accounting for about 14% of deaths among males and 7% of deaths among females Of the 1.6 million violence-related deaths worldwide (including those from conflict and suicide) that occur each year, 90% happen in low- and middle-income countries
 that occur each year, 90% happen in low- and middle-income countries")
130
Source: Deaton 2005

131
Iodine Toxicity Chronic toxicity may develop when intake is > 1.1 mg/day. Some people who ingest excess amounts of iodine, particularly those who were previously deficient, develop hyperthyroidism (Jod-Basedow phenomenon). Paradoxically, excess uptake of iodine by the thyroid may inhibit thyroid hormone synthesis (called Wolff- Chaikoff effect). Thus, iodine toxicity can eventually cause iodide goiter, hypothyroidism, or myxedema. Very large amounts of iodide may cause a brassy taste in the mouth, increased salivation, GI irritation, and acneiform skin lesions.
. Paradoxically, excess uptake of iodine by the thyroid may inhibit thyroid hormone synthesis (called Wolff- Chaikoff effect). Thus, iodine toxicity can eventually cause iodide goiter, hypothyroidism, or myxedema. Very large amounts of iodide may cause a brassy taste in the mouth, increased salivation, GI irritation, and acneiform skin lesions..")
132
Vitamin A Toxicity Can occur when large amounts of liver are regularly consumed and from taking excess amounts of the nutrient in supplements Four major adverse effects: –birth defects, –liver abnormalities, –reduced bone mineral density that may result in osteoporosis, and –central nervous system disorders Signs of acute toxicity include nausea and vomiting, headache, dizziness, blurred vision, and muscular uncoordination.

133
Iron Toxicity children can sometimes develop iron poisoning by swallowing too many iron supplements. Symptoms of iron poisoning include: Fatigue; Anorexia; Dizziness; Nausea; Vomiting; Headache; Weight loss; Shortness of breath; Grayish color to the skin

134
Zinc Toxicity Zinc supplements in large amounts may cause diarrhea, abdominal cramps, and vomiting, usually within 3 - 10 hours of swallowing the supplements. The symptoms go away within a short period of time after stopping the supplements.

135
Source: De Onis 2000

136
Dietary Energy Supply, USA WHO Global Database on Body Mass Index

137
Height-for-age and systolic blood pressure Victora et al, 2008

138
Trends in Body Weight Marques-Vidal et al, 2008

139
Trends in BMI Marques-Vidal et al, 2008

140
Trends in Height Marques-Vidal et al, 2008

141
Height-for-age and offspring birthweight Victora et al, 2008

142
Height-for-age and BMI Victora et al, 2008

143
Height-for-age and glucose concentration Victora et al, 2008

144
1984-1985 Ethiopian Famine

145
North Korean Famine 1996 After the withdrawal of USSR and Chinese food subsidies in the early 1990s and the cumulative effect of collective farming, food availability in North Korea declined steadily and then plummeted between 1995 and 1997 when flooding followed by drought struck the country. From 1994 to 1998, 2-3 million people died of starvation and hunger-related illnesses

146
North Korean Famine Timeline

147
Relief Foods Often cereals (corn, rice, flour) Lack nutritional diversity Emergency food aid today consists of cereals (often supplemented with soya for protein and micronutrients) and accompanied by pulses
 Lack nutritional diversity Emergency food aid today consists of cereals (often supplemented with soya for protein and micronutrients) and accompanied by pulses")
148
Prediction Efforts Identify ‘normal’ then detect deviations from that normal state Famine codes Early warning systems Coping strategies as prediction tools Nutrition surveillance

149
Coping Famines may be slow processes with long tails Trigger event then long process of coping strategies – Wild foods (non-customary) – Change in activities – Migration and risk taking Beneficiaries of process (those that get rich during famines)
 – Change in activities – Migration and risk taking Beneficiaries of process (those that get rich during famines)")
150
Height, Ability and Labour Markets Case et al, 2006

Similar presentations