Download presentation
Presentation is loading. Please wait.

1
Epidemiologic Transition: Russian examples
Abdel Omran. The Epidemiologic Transition: A Theory of the epidemiology of population change. Milbank Quarterly ;49: Omran has writen several classic papers on the epidemiologic transition. This lecture will be dedicated to the process of epidemiologic transition in Russia. Faina Linkov, PhD, University of Pittsburgh

2
Questions to be discussed at the end of the lecture
Can Omran’s theory be applied to changing mortality patterns in Russia? Epidemiologic transition in Russia: did it take place? Reversal of transition in Russia. How does it relate to Omran’s theory? Virtually all industrialized countries followed the pattern of epidemiologic transition described by Omran. During various periods of its history, Russia also followed this pattern, however in this lecture we will learn that Russia’s pattern of morbidity and mortality does not fit Omran’s theory perfectly. We will discuss these questions at the end of the lecture. There is no right or wrong answer to these questions.

3
The content of this lecture is relevant to the territory of Russian Federation, as well as the countries of the Former Soviet Union, which became separate independent countries around 1991.

4
Epidemiologic transition: Definition
The epidemiologic transition is that process by which the pattern of mortality and disease is transformed from one of high mortality among infants and children and episodic famine and epidemic affecting all age groups to one of degenerative and man-made diseases (such as those attributed to smoking) affecting principally the elderly. Encyclopedia Britanica Epidemiologic transition was first described by Abdel Omran in early 1970’s. The majority of the points he made in his classic paper are true today.
 affecting principally the elderly. Encyclopedia Britanica. Epidemiologic transition was first described by Abdel Omran in early 1970’s. The majority of the points he made in his classic paper are true today.")
5
Stages of Epidemiological Transition
Age of Pestilence and Famine Age of Receding Pandemics Age of Degenerative and Man-made diseases These are the three major stages of epidemiologic transition coined by Omran

6
Age of Pestilence and Famine
Characterized by high mortality rates, wide swings in the mortality rate, little population growth and very low life expectancy During the age of pestalence the population on a reoccuring basis is being decimated by epidemics of infectious diseases. The mortality rates drive the system. Life expectancy is low, fertility is high, but the high fertility rates are off set by very high mortality rates. Traditional society, chronic shortage of food, poor sanitary conditions, high MCH morbidity and mortality, environmental problems, young population

7
Peter I, the first emperor of Russia
Peter I, famous Russian tsar of the 18th centurey, had 10 legitimate children. Only 1 of them lived past the age of children died in infancy. Thus, despite being one of the richest people of his time, the morbidity and mortality patterns of his family followed the classical route of the age of pestilence and famine.

8
Age of Receding Pandemics
Epidemics become less frequent, infectious diseases in general become less frequent, a slow rise in degenerative diseases begin to appear, improved life expectancy, organized health services, increased proportion of older people In this era, the epidemics of TB, plague, malaria, etc. begin to subside. The death rate goes down with little change to the fertility rates, thus population growth occurs. During this time one sees the beginning of non-communicable diseases.

9
Alexander III, the last Russian Emperor to die from natural causes
Alexander III was a Russian monarch of the late 19th century, who lived during the timeframe corresponding to the age of receding pandemics. Only 1 of his 6 children died in infancy.

10
Age of Degenerative and Man-made diseases
Chronic diseases, cheap calories, morbidity overshadows mortality, rise in living standards, dramatic decline in fertility, comprehensive healthcare This is the age we are living in today

11
Mickhail Gorbachev, the first and the last President of the USSR
Mickhail Gorbachev, Soviet/Russian leader of the late 20th century has just 1 child, who is currently in her 50’s and still alive. This demonstrates a very interesting concept outlined by Omran: fertility rates go down with the age of degenerative disease and children survive much longer.

12
Infant Mortality Rate in Russia: 1940-1993
One of the major points of Omran’s theory is that infant mortality is the basic driving force for increases and decreases of life expectancy. A radical reduction of the infant mortality rate (IMR) occurred in Russia in the late 1940s and the 1950s. Between 1940 and 1956, the IMR in Russia decreased by approximately 4 times, from 200 per 1,000 to 49 per 1,000.[18] In the next decade, the IMR was cut in half to 25.5 per 1,000 in 1965 (Figure 4.5). As a result, the increase in life expectancy at birth was very large between and years for males and 27.1 for females (Table 4.3). Decreasing mortality at ages under 5 contributed approximately equal fractions of the improvement for males and females (16.5 and 16.8 years, respectively). The influence of mortality decline at adult ages on overall life expectancy improvements was much smaller and unequal by sex: 7.8 years for males and 10.3 years for females. Hence, during two postwar decades, Russian women gained significantly more than Russian men due to the more favorable mortality trends at adult ages. Despite economical crises that took place in Russia over the past 15 years, infant mortality remains relatively low, however male life expectancy is very short.
 occurred in Russia in the late 1940s and the 1950s. Between 1940 and 1956, the IMR in Russia decreased by approximately 4 times, from 200 per 1,000 to 49 per 1,000.[18] In the next decade, the IMR was cut in half to 25.5 per 1,000 in 1965 (Figure 4.5). As a result, the increase in life expectancy at birth was very large between and years for males and 27.1 for females (Table 4.3). Decreasing mortality at ages under 5 contributed approximately equal fractions of the improvement for males and females (16.5 and 16.8 years, respectively). The influence of mortality decline at adult ages on overall life expectancy improvements was much smaller and unequal by sex: 7.8 years for males and 10.3 years for females. Hence, during two postwar decades, Russian women gained significantly more than Russian men due to the more favorable mortality trends at adult ages. Despite economical crises that took place in Russia over the past 15 years, infant mortality remains relatively low, however male life expectancy is very short.")
13
Theory criticisms 2 major challenges/criticisms of the theory
-epidemiologic transition may not be unidirectional (reversal of transition) -consideration for variation among groups
 -consideration for variation among groups.")
14
Applications of Omran’s Theory to Russia: Difficulties in Applying the General Rules
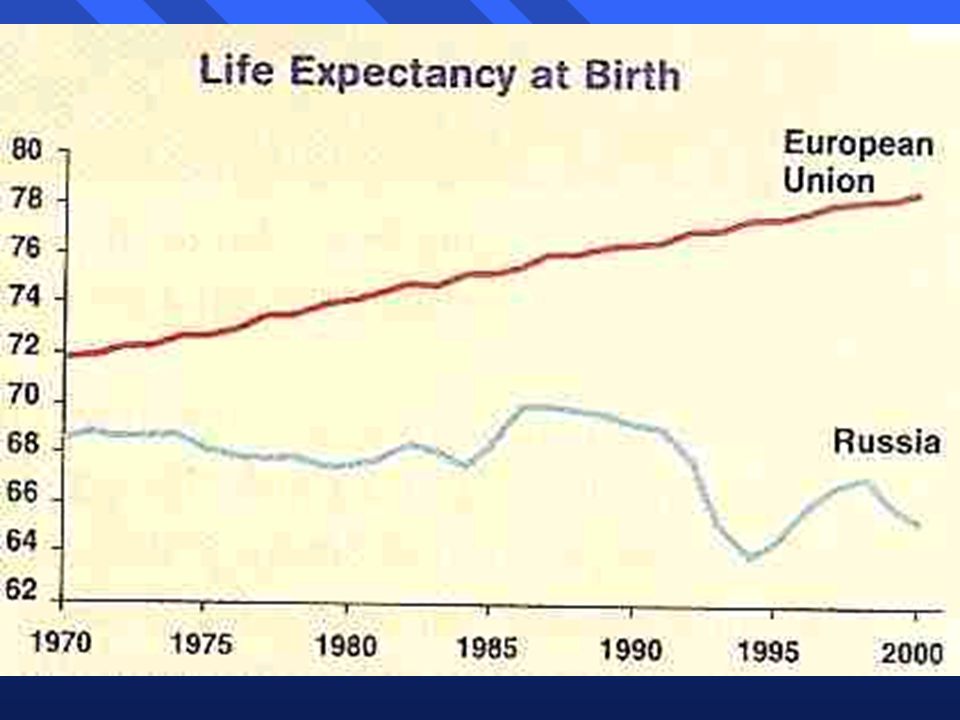
Increased morbidity associated with WWI and WWII, famines, and political repressions Reverse transition in 1990’s Excess mortality for Russian males After the breakdown of Soviet Union in 1991, Russia underwent series of economic crisis. Life expectancy in the 1990’s, especially for males, decreased significantly.

15
Russia’s transition in 1990’s

16
Net Migration and Natural Increase in Russia, 1980–2001
This shows decrease in Russian population starting in the 1990’s, which still continues today, despite increases in migration.

17
Russia: decreasing population
This is another illustration of decreasing population

18
The health care principles upon which the Soviet health care system was to be based (Nikolai Semashko): government responsibility for health universal access to free services a preventive approach to “social diseases” quality professional care a close relation between science and medical practice continuity of care between health promotion, treatment and rehabilitation. How come life expectancy in Russia during the 1960’s was similar to that in the US and other developed world? The answer is simple: prevention and public health.

19
Next steps following the establishment of the “Semashko” model in 1918
The health care system was under the centralized control of the state, which financed services by general government revenues as part of national social and economic development plans. All health care personnel became employees of the centralized state, which paid salaries and provided supplies to all medical institutions. The main policy orientation throughout this period was to increase numbers of hospital beds and medical personnel*.

20
Next steps following the establishment of the “Semashko” model in 1918 (cont.)
Russia made massive strides in arresting the spread of infectious diseases. Drastic epidemic control measures were implemented, particularly in the cases of tuberculosis, typhoid fever, typhus, malaria and cholera. These involved community prevention approaches, routine check-ups, improvements in urban sanitation and hygiene, quarantines, etc.

21
The period until 1991 Life expectancy (both sexes)
")
22
The period until 1991 Life expectancy in 1965

23
A campaign against alcohol
By the 1980s, the gap between Russia and Western countries in life expectancy at birth came to about 10 years for men and 6 years for women, mostly due to high death rates among those of working age (6). In the mid-1980s, the government made an attempt to address this problem (9). It was by then generally understood that potentially avoidable human losses were mostly attributable to excess adult age mortality from particular causes such as injuries, accidental poisoning, suicide, homicide, sudden cardiac death, hypertension and other conditions closely related to alcohol abuse and its consequences.
. In the mid-1980s, the government made an attempt to address this problem (9). It was by then generally understood that potentially avoidable human losses were mostly attributable to excess adult age mortality from particular causes such as injuries, accidental poisoning, suicide, homicide, sudden cardiac death, hypertension and other conditions closely related to alcohol abuse and its consequences.")
24
Life expectancy related to Campaign

25
But…. Russia failed to maintain this record, however: by 1987 the USSR was no longer able to enforce the anti-alcohol campaign and death rates rapidly resumed their upward trend from 1988 onwards. The anti-alcohol campaign was largely prohibitive and did not affect the attitude of the majority of Russia’s population towards alcohol.

26
The period after 1991 The health status of the Russian population declined precipitously following the collapse of the Soviet Union in late By all accounts, in the last decade Russia has been experiencing a shock unprecedented in peacetime to its health and demographic profiles.

27
Life expectancy in Russia, male

28
Life expectancy in Russia, female

29
The leading causes of death in the Russia Federation
Cardiovascular diseases with rates that are the highest in the European Region External causes of injury and poisoning Cancer

30
Causes of the mortality crisis
Major social and economic shock and income stratification in a population already vulnerable because of: Poor diet, high levels of smoking, and weak systems of social support, in which alcohol and, increasingly, intravenous drugs, are easily available. Health care system is poorly equipped to respond to challenges.

32
Figure 4.2 shows for each age group the proportion of mortality due to four principal diagnostic categories of causes of death: 1) infectious diseases (tuberculosis, diarrheal diseases, all other food-born or air-born infections, influenza, rheumatism, pneumonia and other acute respiratory diseases, septicemia, inflammatory diseases, venereal diseases, etc.); 2) degenerative diseases (cardiovascular diseases, cancers, chronic respiratory, digestive, geneto-urinary, nervous diseases); 3) external causes (accidents and violence); and 4) other and unspecified causes. The top figure presents information for Russian males in while the lower panel presents the same information for U.S. males in 1940.

33
OURCES: Real Per Capita Income and Daily Protein Intake provided by the Laboratory for Prognosis of Population Wages and Consumption, Institute for Economic Forecasting, Moscow; Physicians and Hospital Beds Per 10,000 Population from "Sources of Statistical Data," given in this paper; Real Alchohol Consumption, by Shkolnikov, Nemtsov, 1995, and evaluated by A. Nemtsov. Figure Real Per Capita Income, Daily Protein Intake, Number of Physicians and Hospital Beds per 10,000, and Real Alcohol Consumption, Each Compared to the Basic Level of 1970: Russia, As such, a large part of the striking rise in mortality in the 1990s can be ascribed to the effects of a number of serious shifts in Russian society. All of them are closely interrelated. It is possible, however, to extract the two principal factors among them. These are: 1) lower living standards; and 2) social disorganization. We cannot discuss the links between these two here. However, we can say that the negative changes in living conditions themselves are not as bad as to lead to the massive deterioration in public health evident in the shifts in mortality by age and cause of death in In many countries, where living standards are much worse than in Russia--even in some developing countries--male life expectancy is significantly higher. We can suppose that some kind of complex interaction effect, coming from both principal factors, is responsible for the deteriorating health situation. In that case, the negative influence of the first component (real living conditions) is reinforced by the second group of factors (socio-psychological conditions) and vice versa.
 lower living standards; and 2) social disorganization. We cannot discuss the links between these two here. However, we can say that the negative changes in living conditions themselves are not as bad as to lead to the massive deterioration in public health evident in the shifts in mortality by age and cause of death in In many countries, where living standards are much worse than in Russia--even in some developing countries--male life expectancy is significantly higher. We can suppose that some kind of complex interaction effect, coming from both principal factors, is responsible for the deteriorating health situation. In that case, the negative influence of the first component (real living conditions) is reinforced by the second group of factors (socio-psychological conditions) and vice versa.")
34
Questions to be discussed at the end of the lecture
Can Omran’s theory be applied to changing mortality patterns in Russia? Epidemiologic transition in Russia: did it take place? Reversal of transition in Russia. How does it relate to Omran’s theory?

Similar presentations









 Mr Elliott SSOT.>")




>")




