Download presentation
Presentation is loading. Please wait.

1
A&E data sharing: other impacts and applications. Presentation to Alcohol Learning Centre Conference, Hilton Olympia 2nd June 2009

2
. Alcohol & Violence

4
Why A&E Depts? 1. Large number of violent offences which require A&E treatment do not appear in police statistics; Info about location, time of assault can be collected in A&Es to target police resources more effectively; A&Es are the only sources of info about serial (repeat) injury – a recognised precursor to homicide;
 injury – a recognised precursor to homicide;.")
5
Reasons Not to Report? Potential for reprisals; Can’t see value of reporting; Don’t know who assaulted them; Wish to avoid own conduct scrutinised; Anonymised data is essential for understanding more minor woundings. Personal data in cases where patient or others are at risk of future harm.

6
Why A&E Depts? 1. Large number of violent offences which require A&E treatment do not appear in police statistics; Info about location, time of assault can be collected in A&Es to target police resources more effectively; A&Es are the only sources of info about serial (repeat) injury – a recognised precursor to homicide;
 injury – a recognised precursor to homicide;.")
7
Why A&E Depts? 2. They can identify trends in weapon use: the use of glasses and bottles as weapons was first recognised not by police but by A&E services ; They can facilitate increased reporting of violence to the police by those injured who are not in a position to report; A&E staff are powerful and effective advocates for community safety when they work in local crime prevention partnerships;

8
Why A&E Depts? 3. A&E staff can act from patient/victim perspective: crime prevention tends to be orientated towards offenders and offending; NHS is a statutory partner in local crime prevention: A&Es have significant contributions to make if harnessed; Burdens on A&Es can be reduced; A&Es have an ethical responsibility in the public interest to report serious violence.

9
Southampton University Hospital A&E Reception

10
. Why Share?

13
Prevent young people from becoming involved with knife crime Increased risk for those who do carry a knife Over the six months, work intensively with 10 police force areas to make visible, rapid progress to reduce harm caused by teenage knife crime and increase public confidence. Reduce re-offending by those convicted of knife crime Promote responsible parenting Increase safety in high risk premises Reduce illegal sale of knives Deter young people from becoming involved with knife crime Increase likelihood of being caught Increase consequences of being caught Trading standards prioritise test purchasing of underage sales of knives -Youth forums -Marketing campaign -Education programmes -Support for parents (parentlin e plus) - Home Visits and letters to parents -Increase visibility of sentences -Extend expectation to prosecute -Support witnesses and victims -Target the most dangerous - Increase use of search/stop and search -Work with A&E to improve info sharing -Increase knife referral projects - Increase use of licensing act powers -Safer Schools partnerships Named neighbourhood police contact for every school in areas Purpose Objectives Outputs Improve Evidence Base Extend BCS Work with A&E KCP data
 - Home Visits and letters to parents -Increase visibility of sentences -Extend expectation to prosecute -Support witnesses and victims -Target the most dangerous - Increase use of search/stop and search -Work with A&E to improve info sharing -Increase knife referral projects - Increase use of licensing act powers -Safer Schools partnerships Named neighbourhood police contact for every school in areas Purpose Objectives Outputs Improve Evidence Base Extend BCS Work with A&E KCP data.")
14
Medical Confidentiality Patients have a right to expect that doctors will not disclose any personal information gleaned during treatment. Any information disclosed requires patient consent. Exceptions: Inability to provide consent; Court order/legal duty; Public interest. Duty of confidentiality owed to <16 year old is as great as that owed to any other person.

15
Identifies or expresses opinion about individuals Must be lawfully processed in line with patients’ rights Disclosure without consent is only justified when there is a substantial chance of preventing/detecting crime or arresting/prosecuting offenders Personal Data (Data Protection Act 1998)
")
16
GMC/ACPO/BAEM Guidance All gunshot wounds should be reported promptly Police investigations should not delay care Patients may choose not to speak to police Disclosures in the public interest are justified: Where this may assist in the prevention, detection and prosecution of a serious crime Where failure to disclose would put the patient or someone else at serious risk

17
. The Cardiff Model

18
Home Office Bid 1999 Prof Jonathan Shepherd Tackling Alcohol Street Crime (TASC) –Licensees Forum –Door Staff –Licensing Policy and Practice –Awareness Campaigns –Targeted Policing –Servewise –Education in Schools –Support for victims of assaults The Cardiff Model
 –Licensees Forum –Door Staff –Licensing Policy and Practice –Awareness Campaigns –Targeted Policing –Servewise –Education in Schools –Support for victims of assaults The Cardiff Model")
19
Electronic data collection system in A&E; Capacity to anonymise & share A&E data; Analyst in CDRP integrates and summarises info about violence from police & A&E sources; Senior NHS clinician committed to injury prevention willing to lead A&E implementation; A&E clinician attends CDRP regularly; Violence is prioritised as a public health issue; The Cardiff Model

20
Police Action / Targeted Intervention Alcohol-Related Assault Community Safety Data Collected in Emergency Department Identify Share Information Data Matching and Analysis Solution to cause – crime reduction The Virtuous Circle

21
Essential A&E Data Victim age and gender Violence date and time Exact location Weapon Also Desirable Assailant gender and number Repeat violence Relationship with assailant(s) Reported to Police?
 Reported to Police")
22
NEW DATA - ESSENTIAL Assault Type Assault location Body Part Weapon Pushed Unknown Body Part Fist Feet Head Other Weapon Glass Bottle Knife Blunt object Gun Other Bar/pub Club Street Own home Someone else’s home Workplace Other Free text facility to give specific details of location EXISTING DATA Age & gender Postcode of Residence Incident Type Assault Date & time of assault

23
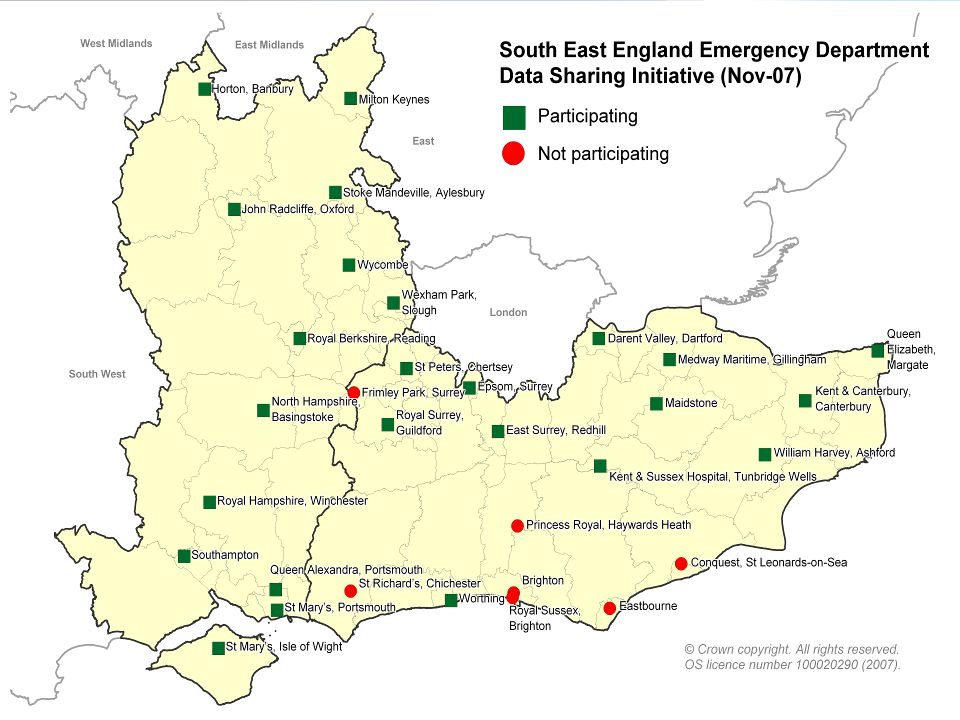
Raising the profile of Cardiff model within existing partnerships; Identifying key individuals who would act as local advocates; Identifying early adopter sites; Implementation in the South East Sub-regional conferences to promote initiative.

24
Implementation in the South East Establish electronic A&E data collection system with a minimum data set; Produce protocols - data safety and transfer & management of patients who are identified as vulnerable/at-risk; Create a system to transfer de-personalised data to local CDRP/Community Safety data collation; Regular summary report for the CDRP, partners and GOSE; Requirements:

26
Challenges Connecting for Health; Sharing data with CDRPs; Ethical issues – giving data to the Police to prevent further assaults; Ownership of follow-through by senior clinicians and NHS managers; Embedding comprehensive approach to community violence prevention.

27
. From Tactics to Strategy

28
Violence and the Health Sector In the Emergency Dept: Routine enquiry re alcohol & violence; Record location & time of violent injuries; Share Anonymous Information with CDRP; Domestic Violence support Nurse; Alcohol Brief Interventions - A&E, GUM, 1° Care; Embed Protocols & Training; Alcohol & Violence Support - info & leaflets; Confidential Police-direct phone in A&E waiting area; Ambulance forensic blankets; Referral pathways to GUM/SARC, GP, Drug Services, Mental Health & Vol & Community Sector.

29
Routine evaluation of the impact of these decisions Strategic & operational decisions routinely based on this analysis Regular commissioning & consideration of analytical products by RAG and TCG Regular analysis of the A&E data (strategic & operational) in conjunction with other violence data sources Regular exchange of A&E data with CSP (monthly & electronically) Degrees of engagement
 in conjunction with other violence data sources Regular exchange of A&E data with CSP (monthly & electronically) Degrees of engagement")
30
-Crime Reduction -Safer Communities -Improving Health LSP- LAA Priority, CDRP ensures Action A&E and Health: Routine enquiry re alcohol & violence: A&E, MH, 1° Care Record location & time Of violent injuries Share Anonymous Information with CDRP DV support Nurse Alcohol Brief Interventions: A&E, GUM, PHC Embed Protocols & Training Alcohol & Violence Support/ info leaflets Police direct phone in A&E Waiting area Ambulance forensic blankets Referral pathways to GUM/ SARC, GP, Drug Services, MH & VCS Local Authority: Workplace violence & Bullying policies Housing & support for Offenders & drug misuse Improve Street Lighting Night time public transport Disperse fast food venues & Taxi ranks Reduce litter & graffiti Night time litter collection Increase Pedestrian Areas Alcohol Misuse Enforcement Campaigns Police: Increase Reporting of Crime Analyse police & A&E data to inform activity Inform location of CCTVs Share data with CDRP Refer Child Protection & DV unit Refer Victim Support Fixed Penalty Notices, ASBOs & Drink Banning Orders Licensing Committee: Licence & Opening hours Reduce happy hours, increase lager price Soft drinks & ‘cooling down’ period Door Supervisors & staff training Alcohol Disorder Zones Toughened bottles & glasses Public awareness posters VCS Support Ensure sufficient Capacity, Resources & Standards Children & YP: Parenting Skills Violence Prevention skills Schools & high risk groups School Bullying Policy CAMHS: Conduct Disorder Child Protection- Health & SS Drinks Industry: Local sponsorship Policy & Staff training Social Responsibility Standards Shepherd J, Sheehan D & Nurse J, 2005

31
Child Protection A pathway was developed to identify vulnerable carers with dependant children at home During a 2 year period over 300 children at risk were identified from carers with drug/ mental health/ alcohol/ Domestic abuse related issues. These children were not present at the time of their carers attendance to A&E Over 60 cases of high risk DA were identified and referred to relevant agencies during a 5 month period The A&E joined the Multi Agency Risk Assessment conference Teaching sessions were developed Links were made with maternity services

32
Ambulance Data A collaborative project between the Directorate of Public Health East Midlands, the East Midlands Ambulance Service NHS Trust (EMAS) and the East Midlands Public Health Observatory (EMPHO). To explore the contribution that CAD (Control Ambulance Dispatch) data can make to alcohol harm reduction by: developing a methodology to identify which calls to the ambulance service were likely to be alcohol-related mapping these alcohol related pickups to identify locations where alcohol harm is taking place
 data can make to alcohol harm reduction by: developing a methodology to identify which calls to the ambulance service were likely to be alcohol-related mapping these alcohol related pickups to identify locations where alcohol harm is taking place.")
33
Alcohol-related pickups interpolated heat map Warmer colours indicate a greater number of expected alcohol-related pickups. Map based on actual counts of pickups (July September 2007). Using this map areas of interest were identified for closer examination.
. Using this map areas of interest were identified for closer examination..")
34
Alcohol-related pickups by ambulance The counts of pickups were 'clustered' by laying a 100m grid over the surface and counting the number of pickups occurring within each 100m square.

35
Alcohol-related pickups by ambulance Centre of Nottingham, corresponds well with local knowledge.

36
Cost of alcohol-related pickups Each pickup is estimated to cost £193 (EMAS 2006/7). Nottingham centre is overlaid with concentric circles of radius 0.5km, 1m and 1.5km. The cost due to alcohol-related pickups in each ring is shown in red within the ring. The cost for the centre of Nottingham was £63,304.

37
Contact Details David Sheehan Department of Health South East Government Office South East Bridge House 1 Walnut Tree Close Guildford Surrey GU1 4GA 01483 882498 david.sheehan@dh.gsi.gov.uk

Similar presentations










 25 th June 2012.>")



 Sue Richards Managing Director Results Leadership Group Australia.>")




 and Schools in Cambridgeshire Josie Collier – LSCB Business Manager Sally.>")
>")
