Download presentation
Presentation is loading. Please wait.

1
WHO VIP Webinar THE CARDIFF MODEL FOR VIOLENCE PREVENTION Jonathan Shepherd Professor of Oral & Maxillofacial Surgery Director, Violence Research Group

3
Rank5-14 years15-29 years30-44 years 1 Childhood cluster 200 139 HIV / AIDS 855 406 HIV / AIDS 855 406 2 Road traffic injuries 118 212 Road traffic injuries 354 692 Tuberculosis 368 501 3 Drowning 113 614 Tuberculosis 238 021 Road traffic injuries 354 692 4 Respiratory infections 112 739 Self-inflicted injuries 216 661 Ischaemic heart disease 224 986 5 Diarrhoeal diseases 88 430 Interpersonal violence 188 451 Self-inflicted injuries 215 263 6 Malaria 76 257 War injuries 95 015 Interpersonal violence 146 751 7 HIV / AIDS 46 022 Drowning 78 639 Cerebrovascular disease 145 965 8 War injuries 43 671 Respiratory infections 65 153 Cirrhosis of the liver 135 072 TOP EIGHT GLOBAL CAUSES OF DEATH 2008 SOURCE: WHO

5
RECORDING OF VIOLENCE BY THE POLICE AND IN EDs Police recording varies by victim age and gender and violence location Only 23% of people injured in violence who attend EDs are known to the police Crime surveys in UK, Sweden and US demonstrate similar police recording rates

6
LOW POLICE ACSERTAINMENT OF SERIOUS VIOLENCE IS AN INTERNATIONAL PROBLEM 869 (62%) victims 327 (23%) victims 207 (15%) victims ODENSE UNIVERSITY HOSPITAL POLICE (Faergemann 2006) 1403 (100%) victims
 victims 327 (23%) victims 207 (15%) victims ODENSE UNIVERSITY HOSPITAL POLICE (Faergemann 2006) 1403 (100%) victims")
7
Police recording is not closely related to injury severity 13% of firearm violence recorded in Atlanta EDs was not recorded by police ( Kellerman el al 2003)
")
8
REASONS WHY VIOLENCE IS NOT KNOWN TO THE POLICE Non reporting reflects fear of reprisals, inability of injured people to identify assailant(s), unwillingness to have own conduct scrutinised and need for emergency treatment Non recording of reported incidents
, unwillingness to have own conduct scrutinised and need for emergency treatment Non recording of reported incidents")
9
National / Regional violence measurement Emergency Department data Local surveillance/prevention INJURY-BASED APPROACH:

10
INDEPENDENT NATIONAL CORRELATES WITH ED TREATMENT AFTER VIOLENCE Unemployment / Deprivation Ethnic minority population Alcohol expenditure Alcohol price Season

11
PROTOTYPE COMMUNITY SAFETY PARTNERSHIP

12
PROTOTYPE CRIME REDUCTION PARTNERSHIP: CARDIFF VIOLENCE PREVENTION GROUP Statutory in UK: 373 crime reduction partnerships Crime and Disorder Act 1998 Police Reform Act 2002

13
SUSTAINABLE ED DATA COLLECTION AND USE Step One: 24 hour electronic data collection (precise violence location, time and weapon) by ED clerical staff when patients first attend Step Two: Monthly anonymisation and data sharing by hospital IT staff with crime analyst Step Three: Monthly combination of police and ED data by analyst Step Four: Summary of violence times, locations and weapons – for police deployment and license regulation Step Five: Continuous implementation and updating of prevention action plan
 by ED clerical staff when patients first attend Step Two: Monthly anonymisation and data sharing by hospital IT staff with crime analyst Step Three: Monthly combination of police and ED data by analyst Step Four: Summary of violence times, locations and weapons – for police deployment and license regulation Step Five: Continuous implementation and updating of prevention action plan")
17
Licensed premises traffic light scheme. Effective policing, situational and environmental interventions: VIOLENCE PREVENTION Targeted street patrols, CCTV, redeployment of police from suburbs into city centre at night Plastic glassware, fast food outlet relocation Pedestrianisation of entertainment streets Identification of people injured in domestic violence

19
VIOLENCE HOTSPOTS IN 21 st CENTURY CARDIFF

20
CHOLERA HOTSPOTS IN VICTORIAN LONDON

21
VIOLENCE RELATED ATTENDANCES – CARDIFF A&E

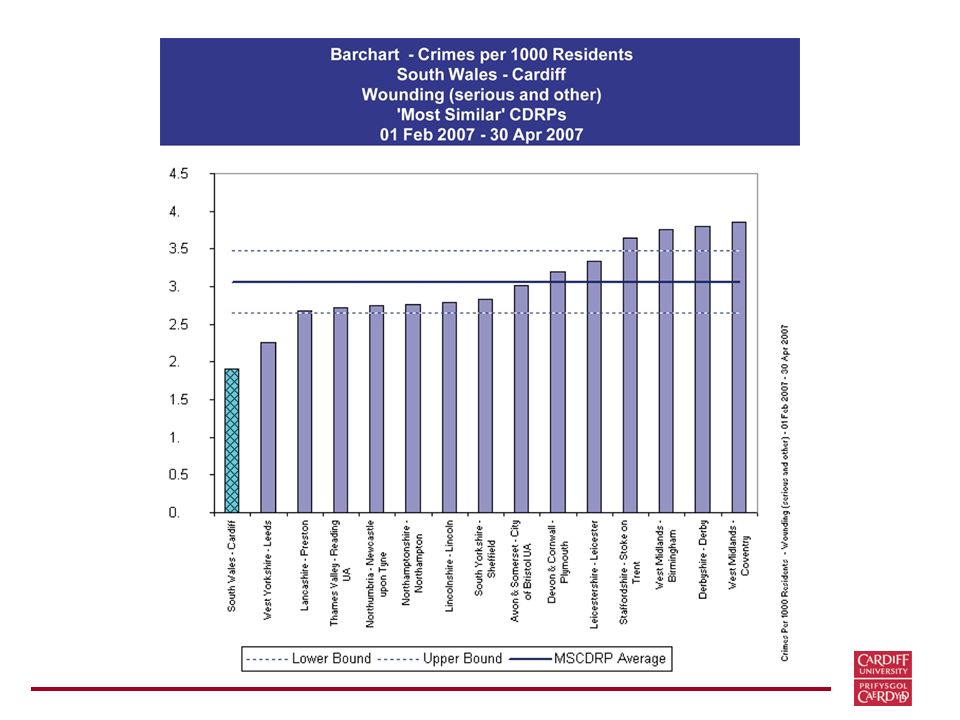
23
Woundings per 1000 population

24
Case Studies ED information identified a source of blunt weapons – a construction site next to a night club with skips containing bricks, concrete blocks and pieces of wood. Skips were secured and violence fell ED information identified series of attacks on cyclists in a neighbourhood. Police targeted this area and violence fell ED information identified several violence hotspot pubs/night clubs. Alcohol licence conditions imposed and some licences revoked. Violence fell Source: Dines 2011

25
CHANGES IN VIOLENCE RELATED HOSPITAL ADMISSIONS AND WOUNDINGS RECORDED BY THE POLICE Hospital Admissions: down 24/year/100,000 population in Cardiff up 36/year/100,000 in comparison cities Woundings recorded by police : up 336/year/100,000 population in Cardiff up 720/year/100,000 in comparison cities Florence et al BMJ 2011

26
ANNUAL COSTS AND BENEFITS Annual cost of Intervention: £5,176 Annual cost of recorded woundings avoided (benefits): £789k Cost/Benefit Ratio - total costs avoided = 1:152 Cost/Benefit Ratio - criminal justice costs avoided = 1:31 Analyses carried out by Curtis Florence at the US Centres for Disease prevention and Control, Atlanta, using 2008 costs
: £789k Cost/Benefit Ratio - total costs avoided = 1:152 Cost/Benefit Ratio - criminal justice costs avoided = 1:31 Analyses carried out by Curtis Florence at the US Centres for Disease prevention and Control, Atlanta, using 2008 costs")
27
How does the Cardiff Model work?

29
The Cardiff Model works by facilitating earlier and more frequent police intervention through the use of information from EDs – and keeps people out of hospital and out of prison

30
Targeted policing prevents violence Eg Braga 2007 and has violence prevention diffusion effects Eg Weisburd et al 2007

32
-4 -2 0 2 4 6 8 10 12 2 years before CCTV Control towns (n=5) CCTV towns (n=5) Percentage change 2 years after CCTV EFFECT OF CCTV ON POLICE VIOLENCE DETECTION Sivarajasingam et al, 2003
 CCTV towns (n=5) Percentage change 2 years after CCTV EFFECT OF CCTV ON POLICE VIOLENCE DETECTION Sivarajasingam et al, 2003")
33
EFFECT OF CCTV ON ASSAULT ED ATTENDANCE Control towns CCTV towns Control towns

34
OTHER MECHANISMS OF EFFECTIVENESS Identification and support of people injured in domestic violence – prevents repeat victimisation Identification of weapon trends – informs weapon-orientated prevention strategies Identifies violence hotspots, park locations and walkways for example, which can be targeted by city government officials

35
PREVENTION INGREDIENTS Emergency physician/surgeon contributions to local community safety partnerships: advocacy from health makes a difference

37
PITFALLS Lack of leadership and management Low data quality Poor analysis Information not used Purpose of information not explained Too much strategy, not enough tactics Complicating a simple process

38
A NEW WEAPON STRATEGY: PREVENTING GLASS INJURY

39
Toughened glass Non-toughened glass

41
All violenceDomesticStrangerAcquaintance (%) (%) (%) (%) NATIONAL EFFECT: USE OF WEAPONS IN VIOLENCE British Crime Survey 19982000199820001998200019982000 Glass /52<1<112463 bottle weapon No8082889372818178 weapon
 (%) (%) (%) NATIONAL EFFECT: USE OF WEAPONS IN VIOLENCE British Crime Survey Glass /52<1< bottle weapon No weapon")
42
HIGH PROFILE HOMICIDES CAN GALVANISE PREVENTION

45
UK IMPLEMENTATION Profession guidelines Government Policy Wales: Welsh Government England: Department of Health Scotland: Violence Reduction Unit INTERNATIONAL IMPLEMENTATION US (CDC), Western Cape, Holland WHO IMPLEMENTATION Implementation of the recommendations of the World Report on Violence and Health
, Western Cape, Holland WHO IMPLEMENTATION Implementation of the recommendations of the World Report on Violence and Health")
Similar presentations
















 is an approach that seeks to – Determine the underlying complex mechanisms.>")









 Dr Lesley Graham ISD.>")

 living in private households in England and Wales Measures crime victimisation.>")


