Download presentation
Presentation is loading. Please wait.

1
Inherited Disorders of Haemostasis and Thrombosis Dr Cleona Duggan Consultant Haematologist

2
How does bleeding start and stop? Blood vessel injury The capillary contracts to help slow the bleeding. Platelets make a plug to patch the hole. Clotting factors in plasma work together to form a clot over the plug.

3
How does bleeding start and stop? Blood vessel injury The capillary contracts to help slow the bleeding. Platelets make a plug to patch the hole. Clotting factors in plasma work together to form a clot over the plug.

4
Prolonged bleeding in Haemophilia Haemophilia - clotting factor absent or low. This makes it difficult for the blood to form a clot, so bleeding continues longer than usual (not faster). FVIII deficiency FIX deficiency
. FVIII deficiency FIX deficiency.")
5
Vessel injury Platelet Release rxn Platelet Aggregation Vasoconstriction Coagulation Cascade Stable Haemostatic Plug

6
Congenital bleeding disorders Haemophilia A (Factor VIII Deficiency) Haemophilia B (Factor IX Deficiency) Von Willebrand Disease Factor X Deficiency Factor XI Deficiency Factor VII Deficiency Factor V Deficiency Congenital thrombocytopenia Platelet function defect Rare defects
 Haemophilia B (Factor IX Deficiency) Von Willebrand Disease Factor X Deficiency Factor XI Deficiency Factor VII Deficiency Factor V Deficiency Congenital thrombocytopenia Platelet function defect Rare defects")
7
Principal Bleeding Disorders Haemophilia A (factor VIII deficiency) Haemophilia B (factor IX deficiency) von Willebrand Disease (vWD) Other
 Haemophilia B (factor IX deficiency) von Willebrand Disease (vWD) Other")
8
Haemophilia Haemophilia A VIII deficiency X-linked, 1/3rd carriers <50% FVIIIC. 1:20,000 births Haemophilia B IX deficiency X-linked, 1/3rd carriers <50% FIXC. 1:100,000 These are clinically indistinguishable

10
Haemophilia 1:10,000 males FVIII > FIX x 6 X-linked recessive -lyonisation- females can be affected. 1/3 no family history / spontaneous mutation in FVIII/FIX genes of mother. Molecular diagnosis possible > 90% Carrier status of mother can be accurately predicted (though germline mosaicism cannot be excluded even if maternal DNA does not appear to carry the mutation)
.")
11
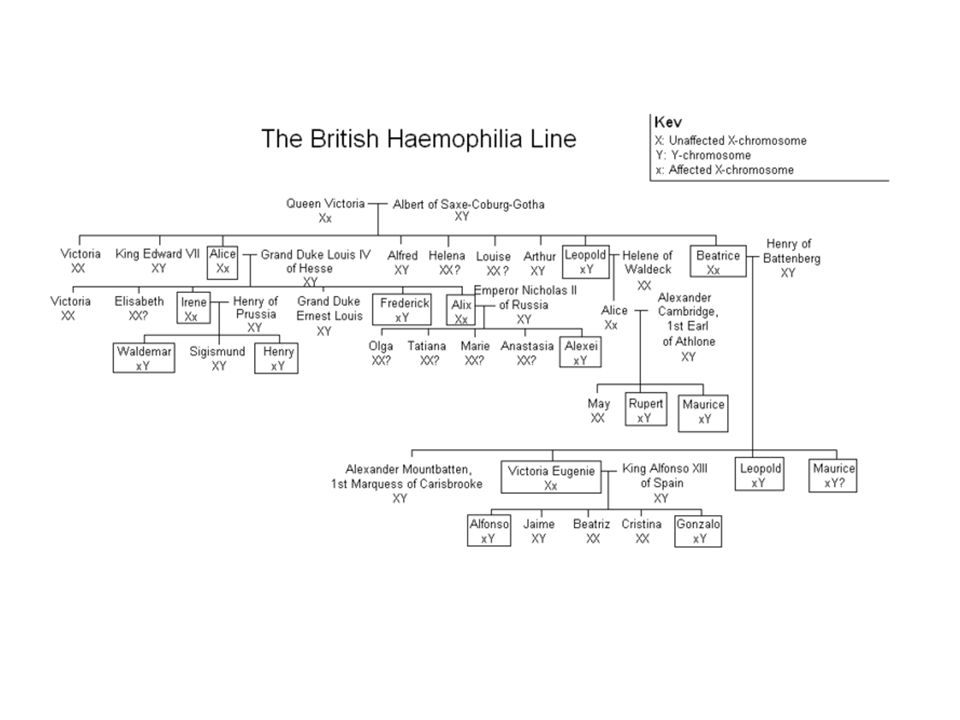
Inheritance What are the chances a baby will have haemophilia? Females XX MalesX Y. The haemophilia gene is carried on the X chromosome X-LINKED DISORDER

12
INHERITANCE OF HAEMOPHILIA

14
Haemophilia Spectrum of severity is wide - clinical phenotype tends to be similar in all affected members of the same family When there is no family history, infants with moderate/severe disease usually present: – post-circumcision bleeding – bad “toddler bruising” – soft tissue/muscle or joint bleeds at 6-18 months of age – RARE, intracranial, ilio-psoas, intra-abdominal, haematuria

15
DISEASE SEVERITY 50-200% 5-50% 2-5% <1% Mild Moderate Severe

16
Detection of Haemophilia Family history Symptoms Haemostatic challenges – Surgery – Dental work – Trauma, accidents Laboratory testing APTT prolonged in FVIII/FIX deficiency F VIII, F IX,vWF

18
Ankle bleed

19
Bleeding following a vein puncture using a vacuum system

20
Femoral arterial puncture

21
Haemophilia in pregnancy Delivery & neonatal period is a high risk time for baby and carrier mother In 1/3 of cases there is no family history 31% of carriers with +ve family history not aware of their carrier status at delivery* Knowledge of carrier status has an impact on delivery and management of baby Mothers unaware of their status were more likely to have instrumental deliveries* *Maclean Haemophilia 2004; 10: 560-4

22
CLINICAL PRESENTATION Bleeding has a prediliction for joints, particularly weight bearing. – Haemarthrosis – Also bleed intramuscularly – Bleed post haemostatic challenge – surgery/dental extraction/injury – Intracranial haemorrhage

23
HAEMOPHILIA - HAEMARTHROSIS

24
CHRONIC JOINT BLEEDING

26
Which joint bleeds are most common? Most common ankles, knees, and elbows – weight bearing joints Bleeds in other joints can also happen, including the toes, shoulders, and hips.

27
What happens in a joint bleed? joint feels tingly and warm. Swelling, painful and difficult to move.

28
Long-term effects of Joint bleeds? Repeated bleeding causes synovium (lining) to swell The synovium stops producing the slippery, oily fluid that helps the joint move. Damages the cartilage- joint stiff, painful and unstable. With time, most of the cartilage breaks down and some bone wears away. The whole process is called haemophilic arthropathy.
 to swell The synovium stops producing the slippery, oily fluid that helps the joint move. Damages the cartilage- joint stiff, painful and unstable. With time, most of the cartilage breaks down and some bone wears away. The whole process is called haemophilic arthropathy..")
29
What Happens in a Muscle bleed? During a bleed, the muscle feels STIFF and PAINFUL. The bleed causes SWELLING that is WARM and PAINFUL to touch. In some deeper muscles, the swelling may press on nerves or arteries, causing TINGLING and NUMBNESS muscle SPASM.

30
Common Muscle Bleeds Calf, thigh, and upper arm. Bleeds in the psoas muscle (front of the hip Can put pressure on nerves and arteries, causing permanent damage. (numbness – classic sign) Joints above and below the muscle can’t move properly. May bleed more often. Nerve damage.
 Joints above and below the muscle can’t move properly. May bleed more often. Nerve damage..")
31
Serious or Life-threatening bleeds? Head injury - Throat /airway bleeds Major loss uncommon except after injury or if related to another medical condition. Other bleeds may be very serious, but usually not life-threatening, eg bleeds into the eyes, spine, and psoas muscle.

32
Haemophilia Mild haemophilia ( 5 - 20 %): –bleed only with trauma and surgery. Severe haemophilia( < 1%) : –Haemarthroses 2-8 times/month. –Muscle bleeds. –Intracerebral bleeding –Prolonged bleeding with trauma and surgery.
 : –Haemarthroses 2-8 times/month. –Muscle bleeds. –Intracerebral bleeding –Prolonged bleeding with trauma and surgery..")
33
Treatment of Bleeds Bleeds should be treated quickly to recover more fully, quickly and prevent later damage. If in doubt, treat. Don’t wait!

34
Treatment of bleeding disorders - general principles Avoid IM injections Avoid NSAIDs Avoid delay in treating the patient. Treat on suspicion of a bleed Listen to the patient - he/she has lifelong experience Record any treatment given including batch numbers to ensure full traceability of factor concentrates Contact the haematologist on call if in doubt

35
Evolution of Clotting Factor Therapy 1. Fresh whole blood 2. Fresh frozen plasma ( FFP ) 3. Cryoprecipitate ( “CRYO” ) 4. Factor VIII / IX concentrates 5. Ultra high purity plasma derived factor VIII / IX concentrates 6. Recombinant factor concentrates
 3. Cryoprecipitate ( CRYO ) 4. Factor VIII / IX concentrates 5. Ultra high purity plasma derived factor VIII / IX concentrates 6. Recombinant factor concentrates.")
36
Factor Concentrates CONCENTRATEINDICATION HALF - LIFE Advate Recombinant FVIII Deficiency 12 Hours BeneFIXRecombinant FIX Deficiency 18 Hours NovosevenRecombinant Patients with inhibitors to FVIII or FIX +/-2.7 Hours

37
Role of factor concentrate Replaces missing factor Injected IV Bleeding stops when enough factor reaches the bleeding site Treat ASAP R.I.C.E.

38
Investigation of bleeding disorders PT, APTT Von Willebrand Factor Specific clotting factor assays Platelet function testing

39
Von Willebrand Disease 1926 1926 5yr old girl – died at 13yr during 4 th menstrual period 5yr old girl – died at 13yr during 4 th menstrual period 4 siblings died from gastrointestinal haemorrhage 4 siblings died from gastrointestinal haemorrhage Both parents had significant bleeding history Both parents had significant bleeding history VWF – identified 1950s, purified 1972, sequenced 1985 VWF – identified 1950s, purified 1972, sequenced 1985

40
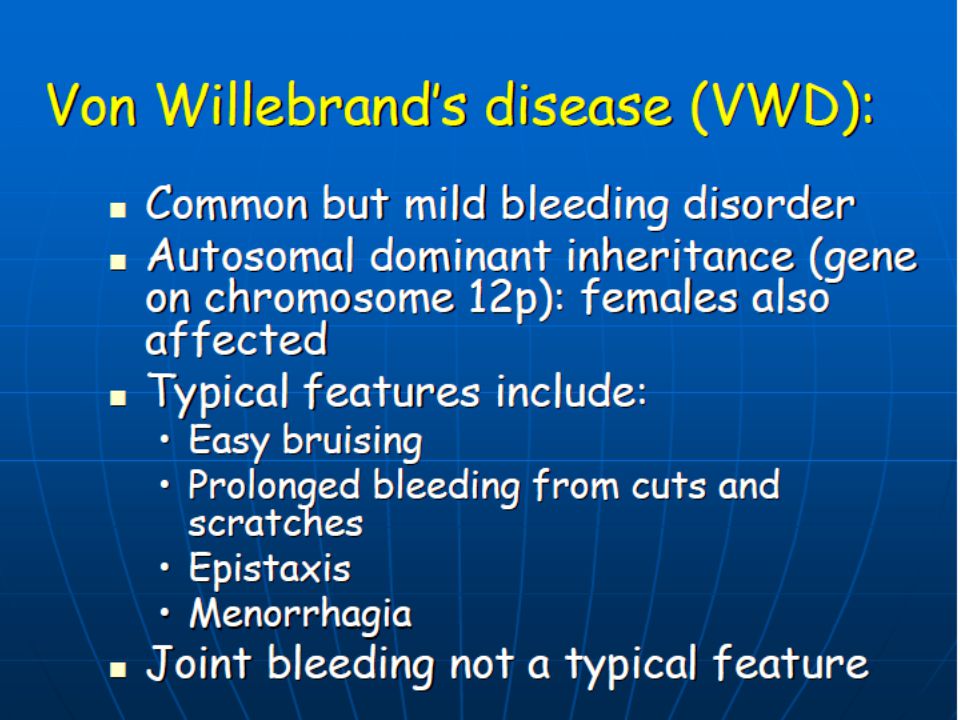
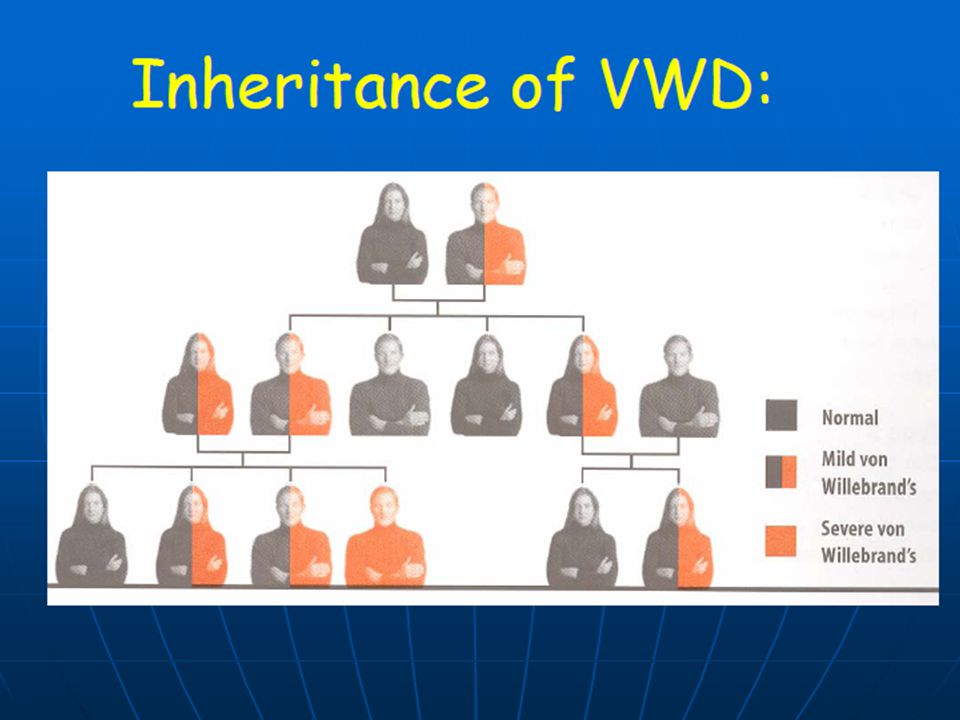
Von Willebrand Disease Up to 1% of the population 125 / million have a clinically significant bleeding disorder Autosomal inheritance

45
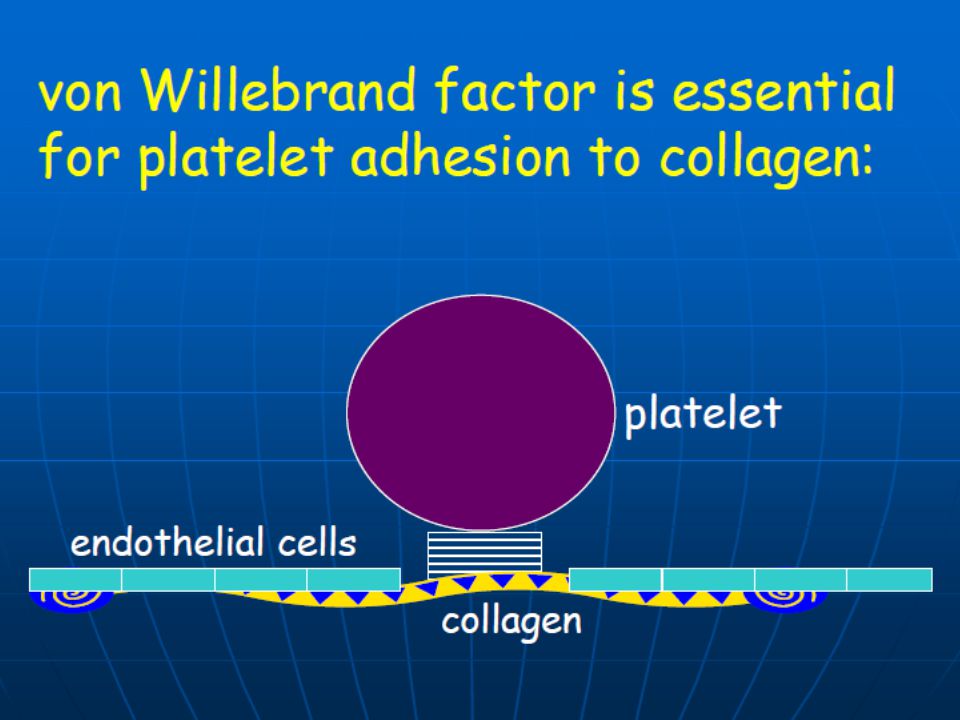
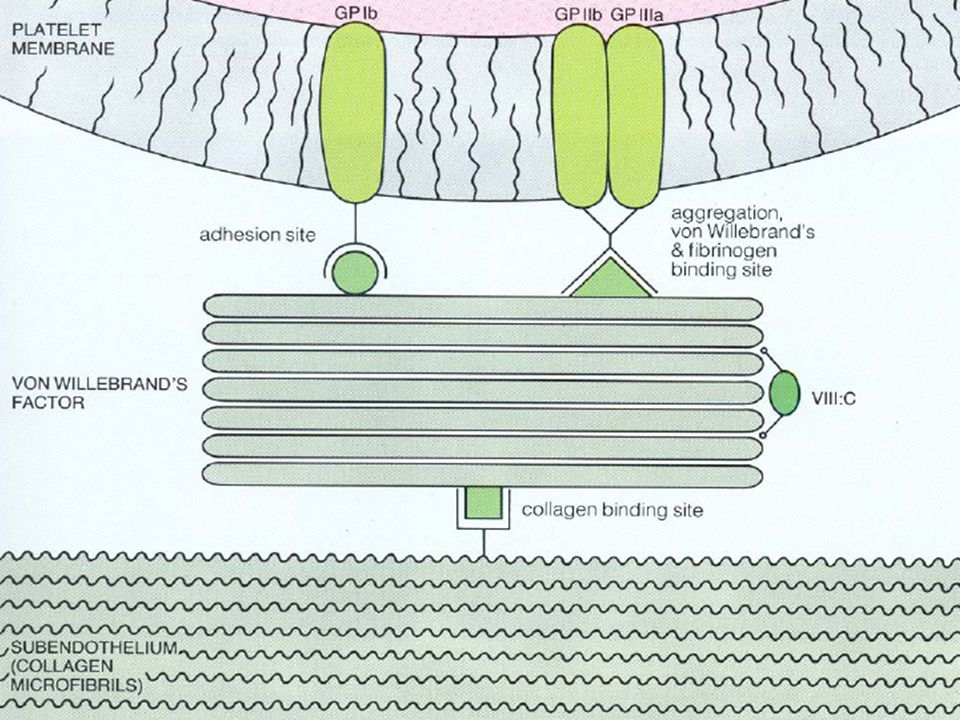
Von Willebrand factor Large glycoprotein produced by endothelial cells and megakaryocytes Mediates platelet to endothelial adhesion Mediates platelet to platelet interaction Carrier protein for Factor VIII

46
Von Willebrand Disease MILD/MODERATE BLEEDING TENDANCY mucocutaneous bleeding easy bruising epistaxis menorrhagia recurrent iron deficiency family history

47
VWD Treatment Avoid NSAIDs Avoid IM injections Vaccinate against Hepatitis A and B Treat anaemia Dental hygiene Very few patients require treatment with clotting factor concentrate

48
VWD TREATMENT -Specific measures Fandhi –plasma derived product DDAVP Cyclokapron

49
DDAVP Promotes release of VWF and factor VIII from endothelial cells 0.3ug/kg in 100mls N/Saline over 30 mins Average response is a threefold rise in VWF and FVIII Treatment of choice in responsive patients for spontaneous bleeding, trauma or minor surgery Intra nasal DDAVP

50
VWD TREATMENT -Specific measures Cyclokapron – Antifibrinolytic agent – Stabilises clot – Given orally – Provides adequate cover for minor procedures or dental work

51
Recognition of Bleeding Disorders

52
The Bleeding History Personal history – Epistaxis – Bleeding post surgery – Bleeding post dental extraction – Menorrhagia – History of anaemia – Easy bruising Family history NB

53
The Bleeding history Coag. Deficiencies Prolonged bleeding after trauma and surgery (>24 hrs). Haemarthroses Muscle bleeding. Platelet defects and VWD: Bruising. Petechiae or purpura. Epistaxis. Menorrhagia Prolonged post- trauma bleeding

54
Investigations

56
TISSUE FACTOR +TF VII TISSUE FACTOR COMPLEX XI IX X VIII V PROTHROMBIN THROMBIN VIIVIIa FIBRINOGEN Va VIIIa XIa IXa Xa TRIGGER FIBRIN

57
Investigation of bleeding disorders FBC - platelet count Prothrombin time (PT) - factors V, VII, X Activated partial thromboplastin time (APTT)- factors VIII, IX, XI, XII Fibrinogen
 - factors V, VII, X Activated partial thromboplastin time (APTT)- factors VIII, IX, XI, XII Fibrinogen")
58
Tissue Damage Tissue Factor Exposure / Thromboplastin FVIIFVIIa FX FXa IIIIa FibrinogenFibrin Fibrin Polymer Fibrin Clot FVFVa Tissue factor (Extrinsic) Pathway IIa
 Pathway IIa")
59
KallikreinPrekallikrein FXII FXIIa FXI FXIa FIX FIXa FX FXa IIIIa FibrinogenFibrin Fibrin Polymer Fibrin Clot FVIIIFVIIIa FVFVa Contact factor (Intrinsic) Pathway IIa
 Pathway IIa")
60
VWD diagnosis Coag screen often normal VWF - quantiative assays VWF Ricof - functional assay

61
VWD - diagnosis Levels increased by menstrual cycle, OCP, pregnancy, smoking, stress, inflammatory disorders Repeat sampling recommended equivocal results minor abnormalities strong personal or family history

Similar presentations