Download presentation
Presentation is loading. Please wait.

1
Coagulation Disorders
Corrina Mc Mahon

3
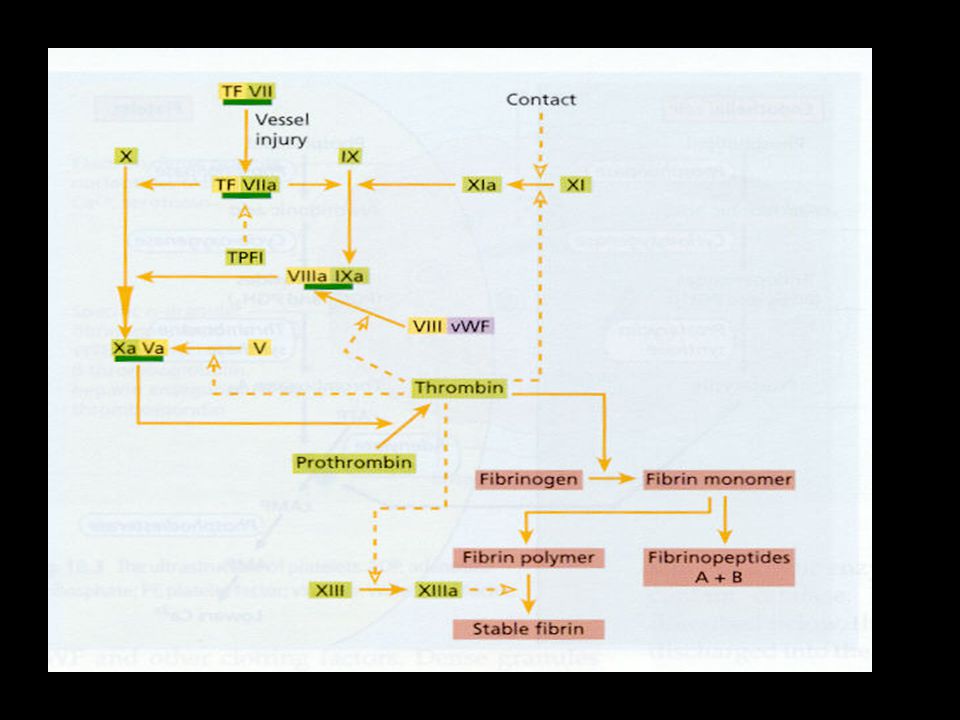
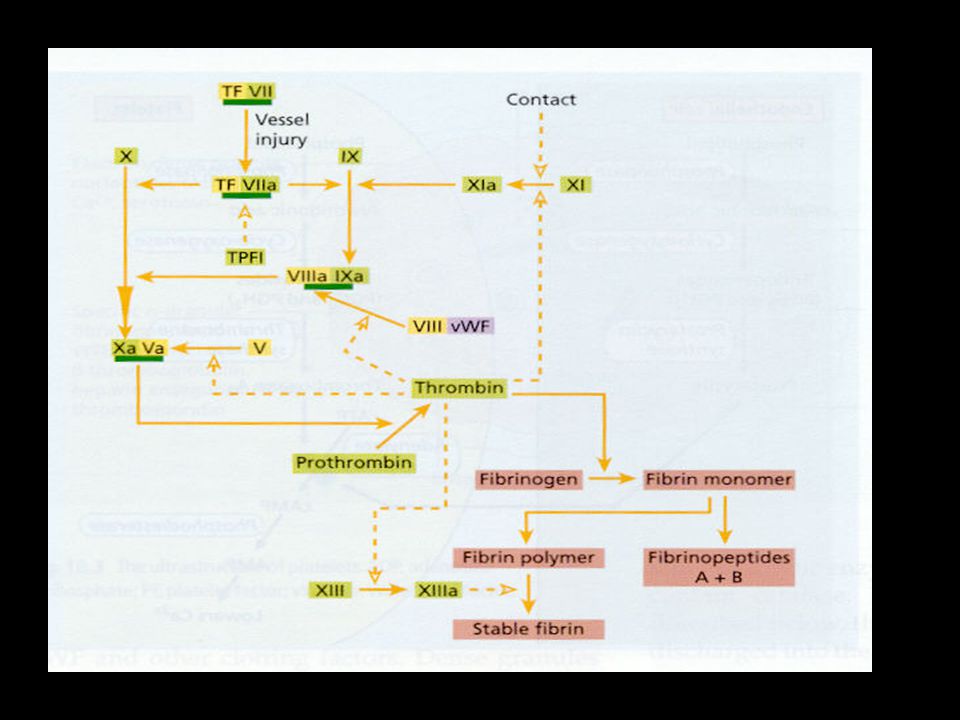
Laboratory investigations
PT: VII, X, V APTT; XII, XI, IX, VIII TT; Fibrinogen D dimers; fibrin breakdown

7
Case 1 4 yr old boy URTI 2 weeks ago Sudden onset bruising/petechiae
PH: Nil FH: Nil Physical examination:

8
Investigations FBC: Hb 11g/dl; WCC 8x10^/l; Platelets <10x10^9/l
PT 14 sec ; APTT 33 sec; Fibrinogen 2.0g/l Treatment options: Nil; IVIg; Steroids Outcome: 90% recovery; 10% chronic

10
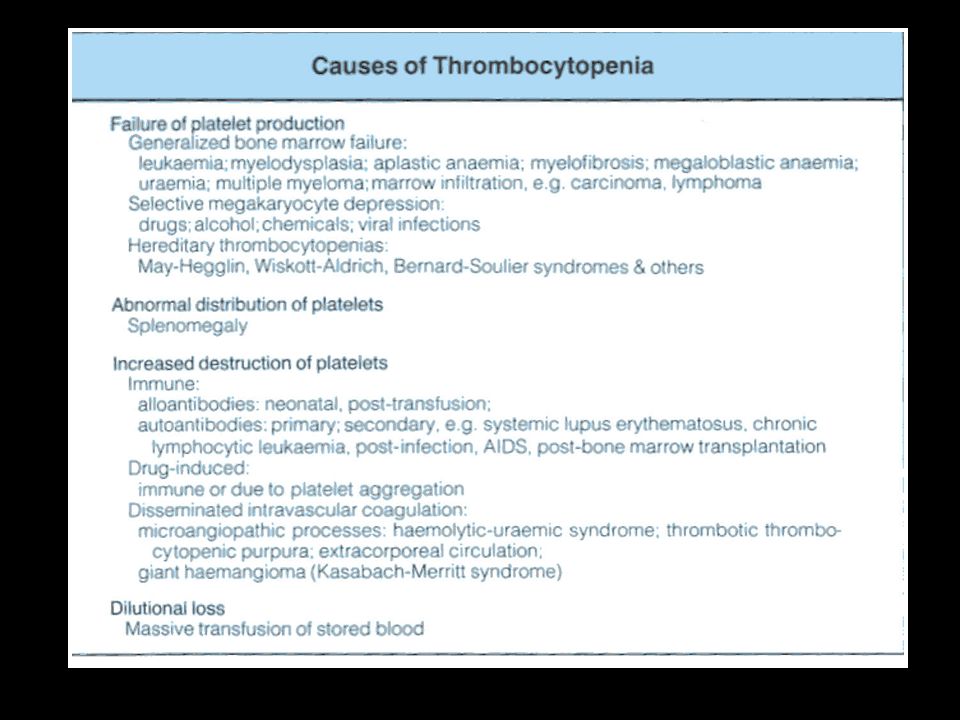
Congenital Thrombocytopenia
Dysfunctional platelets Bernard Soulier Grey platelet syndrome Wiskott-Aldrich syndrome Normal Platelet function May-Hegglin TAR

11
Case 2 Newborn infant Intracranial Haemorrhage No dysmorphic features
1st child No liver/spleen palpable FBC Hb 18.5g/dl WCC 10 x x 109/l /l Platelets 10 x 109/l /l Coagulation screen PT 15 sec. (13-16) APTT 41 sec (28-36)
 APTT 41 sec (28-36)")
12
Differential diagnosis
Infection DIC Immune Thrombocytopenia Alloimmune Isoimmune Congenital Thrombocytopenia TAR syndrome Wiscott Aldrich Syndrome Von Willebrands disease Type 2B A-V malformations

13
Alloimmune Thrombocytopenia
Incidence 1: births IgG antibodies HPA1a 80% HPA5b 15% 50% occur in 1st pregnancy Bleeding can be in utero or after birth Treatment Platelets IVIg ?Steroids

14
Isoimmune Thrombocytopenia
Maternal anti-platelet IgG Placental Passage Thrombocytopenia nadir ~5days post-partum History & examination of mother Treatment IvIg ± steroids

15
Disseminated Intravascular Coagulopathy
Infection Symptoms and Signs Petechiae Bruising Bleeding Laboratory results Anaemia Thrombocytopenia ↑PT/ ↑APTT/↓Fibrinogen/ ↑d dimers

17
Haemophila Inherited Bleeding Disorder Factor VIII/FIX deficiency
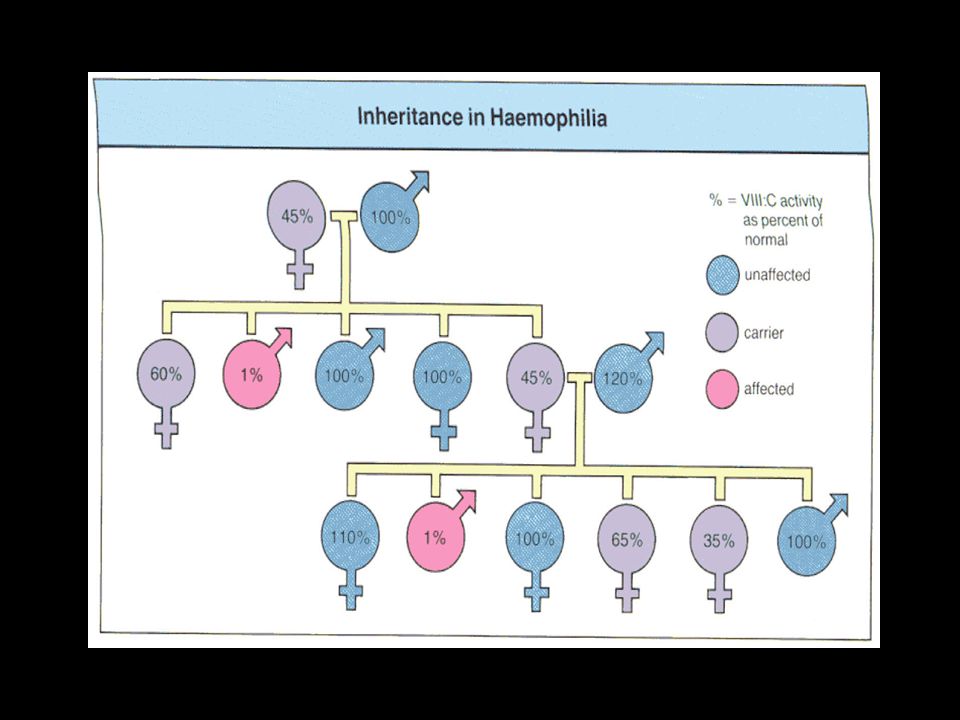
X-Linked Inheritance Carrier XX may have low levels Spontaneous mutation

18
Inheritance of Haemophilia

20
Life Expectancy In Haemophilia

21
Bleeding problems in Haemophilia
Factor Level Type of Bleed <1% Spontaneous/severe 2%-5% Mild trauma/ occasionally spontaneous >5% Trauma/Surgery

22
Intracranial Bleeds At Birth Injury Admission Factor Concentrate
Scanning Observation Neurosurgery

23
Forearm Bleed

24
Joint bleed Synovial inflammation and hyperaemia Synovial overgrowth and Bone resorption Further Bleed Joint Destruction

25
Joint Bleeding

26
Chronic Joint Bleeding

27
The role of prophylaxis in the prevention of joint injury
Lofqvist, Nilsson et al ( Journal Int. Medicine May 1997): 34 patients aged 7-22yrs. Age at commencement of prophylaxis yrs. 79% had no joint problems and the rest had no deterioration in joint abnormalities. Liesner,Khair, Hann, ( BJH Mar 1996) 27 children aged yrs. No. of bleeds/yr pre-prophylaxis-14.5 and post children had evidence of arthropathy which improved on prophylaxis.
: 34 patients aged 7-22yrs. Age at commencement of prophylaxis yrs. 79% had no joint problems and the rest had no deterioration in joint abnormalities. Liesner,Khair, Hann, ( BJH Mar 1996) 27 children aged yrs. No. of bleeds/yr pre-prophylaxis-14.5 and post children had evidence of arthropathy which improved on prophylaxis.")
28
Prophylaxis The Irish Data (1992-1997)
Bleeds/yr, pre-prophylaxis, (mean 38) Bleeds/yr, post-prophylaxis, 0-9 (mean 3.5) Development of inhibitors, 2 - low level (<1Bu) and transient (< 1 year)
 Bleeds/yr, post-prophylaxis, 0-9 (mean 3.5) Development of inhibitors, 2 - low level (<1Bu) and transient (< 1 year)")
29
Prophylaxis Factor VIII T½ = 8 hours Frequency – three times/week
Dose – 20-40iu/kg Factor IX T½ = 18 hours Frequency – twice/week Dose – 50iu/kg

30
Dose Adjustment Growth Break through bleeds

31
Management of Acute Bleeds
Rest Factor Concentrate FVIII; 35-50iu/kg FIX; % (7-10iu/ml) Wt x desired rise x 1.25 Continuous infusion FVIII 50iu/kg bolus; infusion 4iu/kg/hr FIX 100% bolus; infusion 6-8iu/kg/hr
 Wt x desired rise x Continuous infusion. FVIII. 50iu/kg bolus; infusion 4iu/kg/hr. FIX. 100% bolus; infusion 6-8iu/kg/hr.")
32
Mild Factor VIII Deficiency
DDAVP 0.3mcg/kg/30 min Antifibrinolytic therapy

33
Haemophilia The problems
Bleeding Destructive arthropathy Addiction Infection Inhibitors

34
Inhibitors Anti-FVIII Antibodies - IgG Incidence: 10-20%
High responding or lowlevel/transient Familial incidence (x6) Majority <10yrs Occur within first 25 treatment days Bleeding
 Majority <10yrs. Occur within first 25 treatment days. Bleeding.")
35
Management of Inhibitors
Acute Bleeding episodes FVIIa Immune Tolerance High Dose iu/kg/d x 1-3 yrs Cyclophosphamide/FVIII/IVIg 50iu/kg/d x 1->12m 25iu/kg/d x 1->12m

36
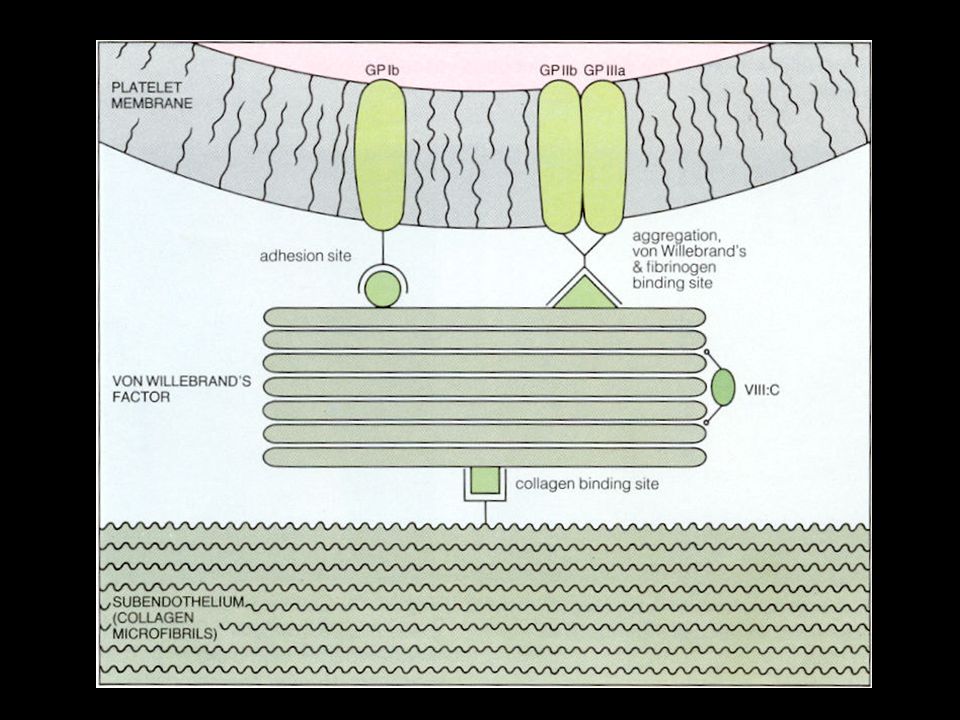
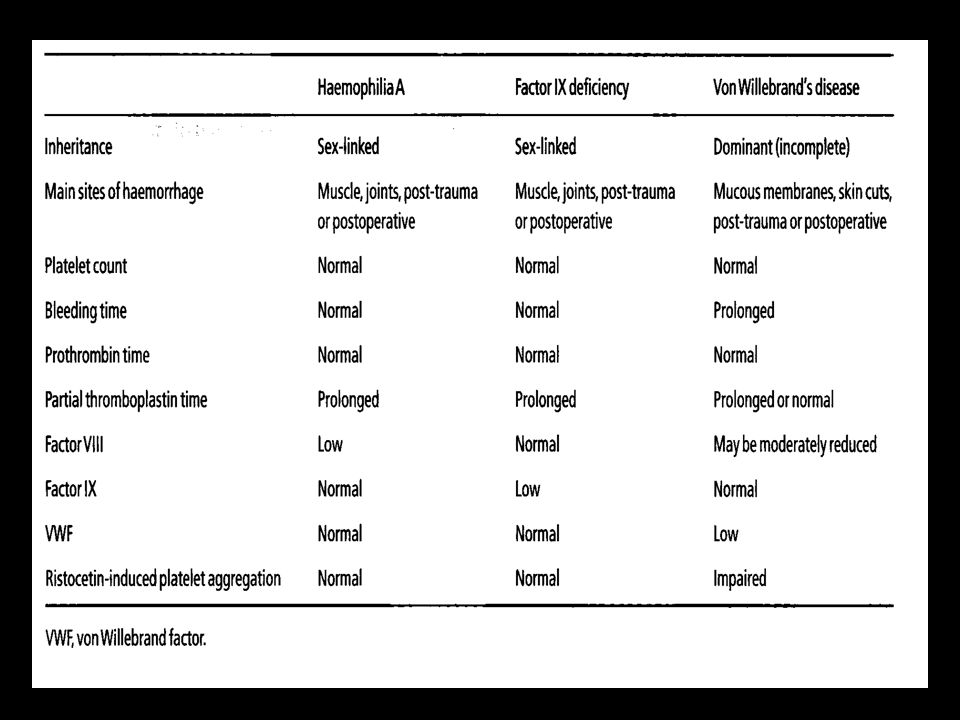
Von Willebrands Disease
Autosomal Inheritance Abnormal VWF S/S: easy bruising, mucosal bleeds, heavy periods Treatment: antifibrinolytic agents DDAVP Plasma derived factor (Fanhdi) Lab Investigations FVIIIc VWF:Ag VWF:RCF Bleeding time VWF Multimers
 Lab Investigations. FVIIIc. VWF:Ag. VWF:RCF. Bleeding time. VWF Multimers.")
Similar presentations