Download presentation
Presentation is loading. Please wait.

1
TYPHOID FEVER AND PARATYPHOID FEVER
Guoli Lin Department of Infectious Diseases The Third Affiliated Hospital of SYSU

2
Typhoid and Paratyphoid
Definition Etiology Pathogenesis Epidemiology Clinical manifestations The laboratory and other examinations Complications Diagnosis and differential diagnosis Prognosis Treatment Preventions Paratyphoid Fever

3
Definition of Typhoid fever
Acute enteric infectious disease caused by Salmonella typhi (S.Typhi). prolonged fever, Relative bradycardia, apathetic facial expressions, roseola, splenomegaly, hepatomegaly, leukopenia. intestinal perforation, intestinal hemorrhage
. prolonged fever, Relative bradycardia, apathetic facial expressions, roseola, splenomegaly, hepatomegaly, leukopenia. intestinal perforation, intestinal hemorrhage.")
4
Etiology Serotype: D group of Salmonella Gram-negative rod non-spore
flagella Culture characteristics

5
Antigens: located in the cell capsule
H (flagellar antigen). O (Somatic or cell wall antigen). Vi (polysaccharide virulence) “widel test”
. O (Somatic or cell wall antigen). Vi (polysaccharide virulence) widel test")
6
A schematic diagram of a single Salmonella typhi cell showing the locations of the H (flagellar), 0 (somatic), and Vi (K envelope) antigens.
, 0 (somatic), and Vi (K envelope) antigens.")
7
Endotoxin A variety of plasmids Resistance: Live 2-3 weeks in water. 1-2 months in stool. Die out quickly in summer Resistance to drying and cooling

8
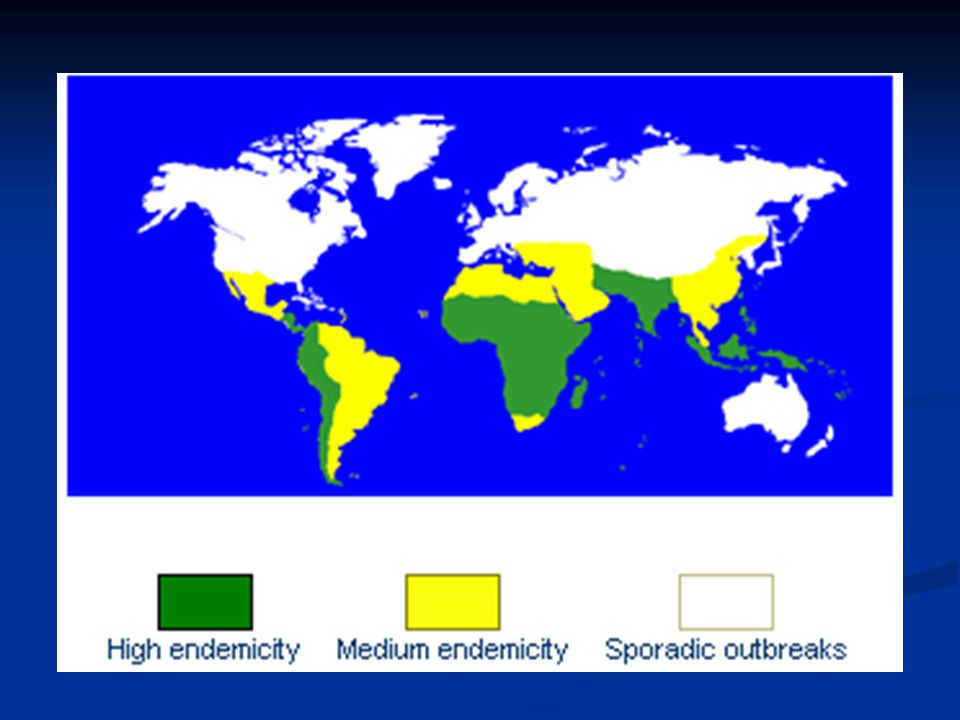
Epidemiology continues to be a global health problem
areas with a high incidence include Asia, Africa and Latin America affects about people with more than deaths a year. 80% in Asia . sporadic occur usually, sometimes have epidemic outbreaks.

10
Source of infection Cases and chronic carriers Cases discharge from incubation, more in 2~4 weeks after onset, a few (about 2~5%) last longer than 3 months chronic carrier Typhoid Mary
 last longer than 3 months. chronic carrier Typhoid Mary.")
12
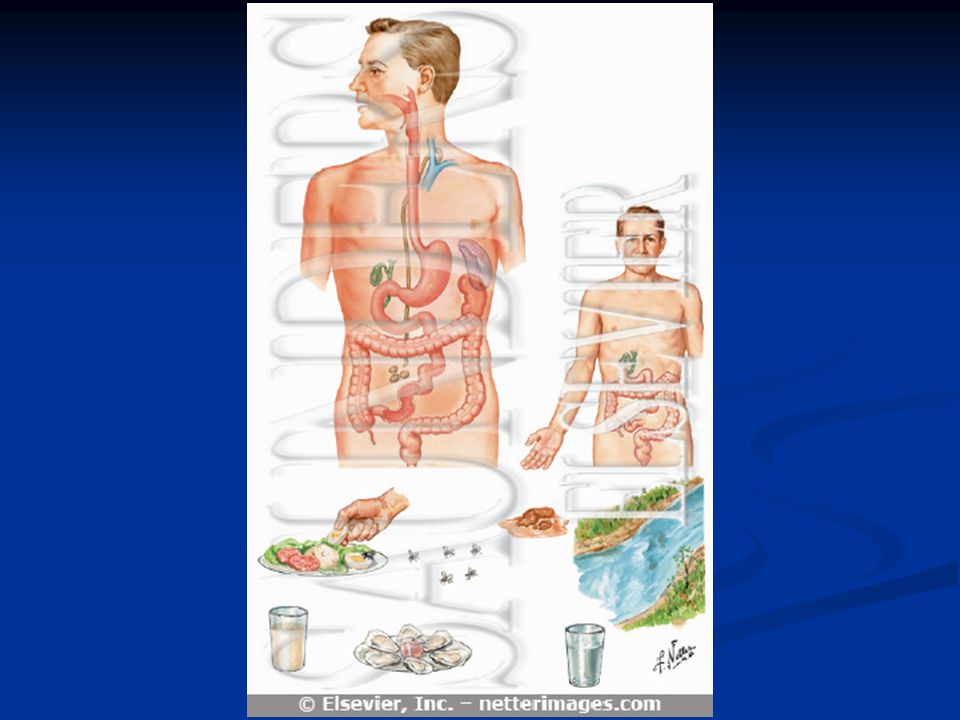
Transmission fecal-oral route close contact with patients or carriers
contaminated water and food flies and cockroaches.

14
Susceptibility and immunity
all people equally susceptible to infection acquired immunity can keep longer, reinfection are rare immunity is not associated with antibody level of “H”, “O”and “VI”. No cross immunity between typhoid and paratyphoid.

15
Susceptibility and immunity
All seasons, usually in summer and autumn. Most cases in school-age children and young adults. both sexes equally susceptible.

16
Pathogenesis gastrointestinal tract host-pathogen interactions
The amount of bacilli infection (>105baeteria).
.")
17
Pathogenesis ingested orally Stomach barrier (some Eliminated)
enters the small intestine Penetrate the mucus layer enter mononuclear phagocytes of ileal peyer's patches and mesenteric lymph nodes proliferate in mononuclear phagocytes spread to blood. initial bacteremia (Incubation period).
.")
18
Pathogenesis enter spleen, liver and bone marrow (reticulo-endothelial system) further proliferation occurs A lot of bacteria enter blood again. (second bacteremia). Recovery
. Recovery.")
19
LN Proliferate,swell necrosis defervescence stage
S.Typhi. liver、spleen、gall、 BM ,ect early stage&acme stage (1-3W) 2nd bacteremia S.Typhi eliminated convalvescence stage (4-5w) Bac. In gall Bac. In feces stomach (mononuclear phagocytes ) Lower ileum peyer's patches & mesenteric lymph nodes 1st bacteremia (Incubation stage) 10-14d LN Proliferate,swell necrosis defervescence stage (3-4w) thoracic duct Enterorrhagia,intestinal perforation
 2nd bacteremia. S.Typhi eliminated. convalvescence stage. (4-5w) Bac. In gall. Bac. In feces. stomach. (mononuclear phagocytes ) Lower ileum. peyer s patches & mesenteric lymph nodes. 1st bacteremia. (Incubation stage) 10-14d. LN Proliferate,swell necrosis defervescence stage. (3-4w) thoracic duct. Enterorrhagia,intestinal perforation.")
20
proliferation of RES (reticuloendothelial system )
Pathology essential lesion: proliferation of RES (reticuloendothelial system ) specific changes in lymphoid tissues and mesenteric lymph nodes. "typhoid nodules“ Most characteristic lesion: ulceration of mucous in the region of the Peyer’s patches of the small intestine
 specific changes in lymphoid tissues. and mesenteric lymph nodes. typhoid nodules Most characteristic lesion: ulceration of mucous in the region of the Peyer’s patches of the small intestine.")
21
回肠: 集合淋巴结(PEYER’SPATCHES)增生
增生")
22
伤寒小结(TYPHOID NODULE)
")
23
Major findings in lower ileum
Hyperplasia stage(1st week): swelling lymphoid tissue and proliferation of macrophages. Necrosis stage(2nd week): necrosis of swelling lymph nodes or solitary follicles.
: swelling lymphoid tissue and proliferation of macrophages. Necrosis stage(2nd week): necrosis of swelling lymph nodes or solitary follicles.")
24
Major findings in lower ileum
Ulceration stage(3rd week): shedding of necrosis tissue and formation of ulcer intestinal hemorrhage, perforation . Stage of healing (from 4th week): healing of ulcer, no cicatrices and no contraction
: shedding of necrosis tissue and formation of ulcer intestinal hemorrhage, perforation . Stage of healing (from 4th week): healing of ulcer, no cicatrices and no contraction.")
25
Incubation period: 3~60 days(7~14). The initial period (early stage)
Clinical manifestations Incubation period: 3~60 days(7~14). The initial period (early stage) First week. Insidious onset. Fever up to 39~400C in 5~7 days chills、ailment、tired、sore throat、cough ,abdominal discomfort and constipation et al.
. The initial period (early stage) First week. Insidious onset. Fever up to 39~400C in 5~7 days. chills、ailment、tired、sore throat、cough ,abdominal discomfort and constipation et al.")
26
The fastigium satge second and third weeks. Sustained high fever、partly remittent fever or irregular fever. Last 10~14 days. Gastro-intestinal symptoms: anorexia、abdominal distension or pain、diarrhea or constipation Neuropsychiatric manifestations: confusion、blunt respond even delirium and coma or meningism

27
Circulation system: relative bradycardia or dicrotic pulse. splenomegaly、hepatomegaly toxic hepatitis. roseola :30%, maculopapular rash a faint pale color, slightly raised round or lenticular, fade on pressure 2-4 mm in diameter, less than 10 in number on the trunk, disappear in 2-3 days.

29
fatal complications: intestinal hemorrhage intestinal perforation
severe toxemia

30
defervescence stage convalescence stage
fever and most symptoms resolve by the forth week of infection. Fever come down, gradual improvement in all symptoms and signs, but still danger. convalescence stage the fifth week. disappearance of all symptoms, but can relapse

31
图 典型伤寒自然病程示意图

32
Clinical forms: Mild infection: very common seen recently
symptom and signs mild good general condition temperature is 380C short period of diseases recovery expected in 1~3 weeks seen in early antibiotics users young children mild more easy to misdiagnose

33
Persistent infection:
diseases continue than 5 weeks Ambulatory infection: mild symptoms,early intestinal bleeding or perforation.

34
Fulminate infection: rapid onset, severe toxemia and septicemia. High fever,chill,circulation failure, shock, delirium, coma, myocarditis, bleeding and other complications, DIC et all.

35
Special manifestations In children
Often atypical sudden onset with high fever. Respiratory symptoms and diarrhea, dominant. Convulsion common in below 3. relative bradycardia rare. Splenomegaly, roseola and leucopenia less common.

36
In the aged temperature not high, weakness common.
More complications.high mortality.

37
Recrudescence clinical manifestations reappear
less severe than initial episode It’s temperature recrudesce when temperature start to step down but abnormal in the period of 2-3 weeks and persist 5~7 days then back to normal. seen in patients with short therapy of antibiotics.

38
relapse serum positive of S.typhi after 1~3 weeks of temperature down to normal. Symptom and signs reappear the bacilli have not been completely removed Some cases relapse more than once

39
Leukocytopenia(specially eosinophilic leukocytopenia).
Laboratory findings Routine examinations: white blood cell count is normal or decreased. Leukocytopenia(specially eosinophilic leukocytopenia). recovery with improvement of diseases decreased in relapse
. recovery with improvement of diseases. decreased in relapse.")
40
Bacteriological examinations:
Blood culture: the most common use 80~90% positive during the first 2 weeks of illness 50% in 3rd week not easy in 4th week re-positive when relapse and recrudesce attention to the use of antibiotics

41
The bone marrow culture
the most sensitive test specially in patients pretreated with antibiotics. Urine and stool cultures increase the diagnostic yield positive less frequently stool culture better in 3~4 weeks The duodenal string test to culture bile useful for the diagnosis of carriers. Rose spots: Not use routinely

42
Serological tests(Vidal test): five types of antigens: somatic antigen(O),flagella(H) antigen, and paratyphoid fever flagella(A,B,C) antigen. Antibody reaction appear during first week 70% positive in 3~4 weeks and can prolong to several months in some cases, antibodies appear slowly, or remain at a low level, some(10~30%) not appear at all.
 not appear at all.")
43
"O" agglutinin antibody titer ≥1:80 and "H" ≥1:160 or "O" 4 times higher supports a diagnosis of typhoid fever "O" rises alone, not "H", early of the disease.Only "H" positive, but "O" negative, often nonspecifically elevated by immunization or previous infections or anamnestic reaction. Antibody level maybe lower when have used antibiotics early.

44
Some cross reaction between group “D” and “A”.
False positive in some infectious diseases. Some positive in blood culture ,but negative in vidal test. 'Vi" often useful for carrier (1:40) molecular biological tests: DNA probe or polymerase chain reaction (PCR)
 molecular biological tests: DNA probe or polymerase chain reaction (PCR)")
45
Complications Intestinal hemorrhage Commonly appear during the second-third week of illness difference between mild and greater bleeding often caused by unsuitable food, diarrhea et al serious bleeding in about 2~8% a sudden drop in temperature、 rise in pulse、and signs of shock followed by dark or fresh blood in the stool.

46
Intestinal perforation:
The more serious .Incidence,1-4% Commonly appear during weeks. Take place at the lower end of ileum. Before perforation,abdominal pain or diarrhea,intestinal bleeding . When perforation, abdominal pain, sweating, drop in temperature, and increase in pulse rate, then, rebound tenderness when press abdomen, abdomen muscle entasia, reduce or disappear in the sonant extent of liver, leukocytosis . Temperature rise .peritonitis appear. celiac free air under x-ray.

47
Toxic hepatitis: common,1-3 weeks hepatomegaly, ALT elevated get better with improvement of diseases in 2~3 weeks Toxic myocarditis. seen in 2-3 weeks, usually severe toxemia. Bronchitis, bronchopneumonia. seen in early stage

48
Other complications: toxic encephalopathy. Hemolytic uremic syndrome. acute cholecystitis、 meningitis、 nephritis et al.

49
图 典型伤寒自然病程示意图

50
Diagnosis Epidemiology data Typical symptoms and signs Laboratory findings.

51
Differential diagnosis Viral infections:
such as upper respiratory tract infection. abrupt onset with fever, headache, leucopenia, sore throat, cough, coryza. no rose spots, no enlargement of liver & spleen. The course of illness no more than 2 wks. differential diagnosis depends on typical manifestations and blood culture.

52
Malaria history of exposure to malaria. Paroxysms(often periodic) of sequential chill,high fever and sweating. Headache, anorexia, splenomegaly, anemia, leukopenia Characteristic parasites in erythrocytes,identified in thick or thin blood smears.
 of sequential chill,high fever and sweating. Headache, anorexia, splenomegaly, anemia, leukopenia Characteristic parasites in erythrocytes,identified in thick or thin blood smears.")
53
Leptospirosis Endemic area,contacted with urine of mice.
Abrupt fever,chills,severe headache,and myalgias, especially of the calf muscles. Leptospires can be isolated from blood,cerebrospinal fluid. Special agglutination titers develop after 7 days and may persist at high levels for many years.

54
Epidemic Louse-Borne typhus
prodromal of malaise and headache followed by abrupt chills and fever. headaches,prostration,persisting high fever. Maculopapular rash appears on the forth to seventh days on the trunk and in the axillas, spreading to the rest of the body but sparing the face,palms,and soles. Laboratory confirmation by proteins OX19 agglutination and specific serologic tests.

55
Tuberculosis continuous high or low fever,fatigue,weight loss,night sweats. Mild cough pulmonary infiltration on chest radiograph positive tuberculin skin test reaction(most cases) acid-fast bacilli on smear of sputum sputum culture positive for mycobacterium tuberculosis.
 acid-fast bacilli on smear of sputum. sputum culture positive for mycobacterium tuberculosis.")
56
Septicemia of Gram-negative bacilli
abrupt onset,high fever,symptom of toxemia. Chill,sweats. Shock. Positive of gram-negative bacilli from blood culture.

57
Prognosis: Case fatality 0.5~1%. but high in old ages、infant、and serious complications Have immunity for ever after diseases About 3% of patients become fecal carriers .

58
good nursing care and supportive treatment
General treatment isolation and rest good nursing care and supportive treatment close observation T,P,R,BP,abdominal condition and stool . suitable diet include easy digested food or half-liquid food.drink more water intravenous injection to maintain water and acid-base and electrolyte balance

59
Symptomatic treatment: for high fever:
physical measures firstly antipyretic drugs such as aspirin should be administrated with caution delirium,coma or shock,2-4mg dexamethasone in addition to antibiotics reduces mortality.

60
Etiologic and special treatment
1.Quinolones: first choice it’s highly against S.typhi penetrate well into macrophages,and achieve high concentrations in the bowel and bile lumens Norfloxacin (0.1~0.2 tid~qid/10~14 days). Ofloxacin (0.2 tid 10~14days). ciprofloxacin (0.25 tid) caution: not in children and pregnant
. Ofloxacin (0.2 tid 10~14days). ciprofloxacin (0.25 tid) caution: not in children and pregnant.")
61
2.Chloramphenicol: For cases without multiresistant S.typhi. Children in dose of 50~60mg/kg/per day. adult 1.5~2g/day. tid. Unable to take oral medication, the same dosage given introvenously after defervescence reduced to a half. complete a 10~14 day course. But ,drug resistance, a high relapse rate,bone marrow toxicity.

62
4.Treatment of complication.
3.Cephalosporines: Only third generation effective Cefoperazone and Ceftazidime. 2~4g/day .10~14 days. 4.Treatment of complication. Intestinal bleeding: bed rest, stop diet,close observation T,P,R,BP. intravenous saline and blood transfusion,and attention to acid-base balances. sometimes,operative.

63
Perforation: early diagnosis. stop diet. decrease down the stomach pressure. intravenous injection to maintain electrolyte and acid-base balances. use of antibiotics. sometimes operative.

64
bed rest, cardiac muscle protection drugs, dexamethasone, digoxin.
Toxic myocarditis: bed rest, cardiac muscle protection drugs, dexamethasone, digoxin. 5.Chronic carrier: Ofloxacin 0.2 bid or ciprofloxacin 0.5 bid, 4~6 weeks. Ampicillin 3~6g/day tid plus probenecid 1~1.5g/day. 4~6 weeks. TMP+SMZ 2 tabs. Bid. 1~3 months. Cholecystitis may require cholecystectomy.

65
Prophylaxis 1.control source of infection
Isolation and treatment of patients stool culture one time per 5 days. if negative continued two times ,without isolation. Control of carriers. observation of 25 days(15 days in paratyphoid) when close contact
 when close contact.")
66
2. Cut of course of transmission
key way avoid drinking untreated water and food. 3.Vaccination side-effect more, less use

67
Paratyphoid fever A,B,C Caused by Salmonella paratyphoid A,B,C.respectively. in no way different from typhoid fever in epidemiology, pathogenesis, pathology,clinical manifestations, diagnosis, treatment and Prophylaxis

68
Paratyphoid A,B: incubation period 2~15days, in genaral,8~10 days.
milder in severity fewer in complications. Better in prognosis, relapse more common in Paratyphoid A. Treatment same as in typhoid fever.

69
Paratyphoid C: Always sudden onset. Rapid rise of temperature.
Presented in different forms-- Septicemia, Gastroenteritis and Enteric fever Complications--arthritis, abscess formation, cholecystitis, pulmonary complications are commonly seen. Intestinal hemorrhage and perforation not as common as in typhoid fever.

70
Thank you!!!

Similar presentations
















. Members of this genus also.>")


, Hepatovirus Picornavirus, enterovirus 72 27 nm 1 serotype only, although there are 4 genotypes.>")

