Download presentation
Presentation is loading. Please wait.

1
Evaluation and Management of Sports Injuries in Children
Michelle Sirak, MD Division Director Pediatric Physical Medicine and Rehabilitation Goryeb Children’s Hospital

2
Disclosure None

3
Learning Objectives Identify acute and chronic sports injuries in the child athlete Evaluate and triage acute and chronic sports injuries Discuss issues and concerns that are unique to the child athlete

4
Common Acute Sports Injuries
Bruises/Contusions Injury after a fall or a bump Swelling and inflammation of soft tissue, muscle, bone Abrasion Injury after a scrape Injury to skin/cut Basic first aid Laceration Tearing/breaking of skin Medical Attention

5
Common Acute Sports Injuries
Sprain Ligament Bone to Bone Overstretched/partially torn Strain Muscle Irritation/Inflammation/P artial Tear with in Muscle Ligament Tear Dislocation Bone moves out of joint Fracture Broken Bone Growth Plate Injuries & Fractures

6
Evaluate Situation Safety Immobilize Talk to the child Once over
Cervical Spine Limb Talk to the child Once over Above and below suspected injury

7
Management - RICE {R} Rest {I} Ice {C} Compression {E} Elevation
Rest the injury Encourage activity with uninjured parts Alternate sports {I} Ice 48 hrs 15 – 20 min on/45 – 60 min off Ice after activity/end of day x several months until symptoms gone {C} Compression Bandage, taping, brace Early When weight bearing {E} Elevation Above the heart to prevent pooling and swelling 4 – 5 x/day while icing

8
Case 1 A 13 year old girl complains of "twisting" her left ankle while playing field hockey. She was running on the field towards the goal. She does not recall exactly in which direction her ankle twisted. She did not feel or hear any "snaps," "pops," or "clicks." She denies sustaining any other injuries and has not sustained any previous injury to her left ankle. On exam she is able to bear some weight on the ankle but it is starting to swell and is painful. Distally, her toes are pink, with brisk capillary refill and intact sensation to light touch. Tenderness can be elicited by palpation over the anterior aspect of the ankle joint.

9
Lateral Ankle Sprain “Rolling over” the ankle
Stretch or tear of 1 or more ligaments in the ankle joint Graded I, II, III based on severity

10
Evaluate Weight Bear Range of Motion Pulses & Capillary Refill
Anterior Draw >5mm Talar Tilt >5-10 degrees

11
Evaluate Higher Up the Leg Syndesmosis Injury Maisonneuve Fracture

12
Lateral Ankle Sprain RICE Crutches until weight bear without pain
Early Mobilization X-ray? Conservative Physical Therapy ROM, Strength, Pain Free activities Grade 3 = Surgical

13
Case 2 A 15 year old boy complains of sharp pain in the back of his right leg. He was running towards the goal while playing soccer. He felt a “pop” and burning sensation in the leg at the time of the injury. It is worse when he tries to actively bend his knee and with walking. On exam he is able to bear weight on his right leg. The back of his thigh is tender to palpation. Pain is elicited when trying to stretch the right leg and when actively bending the right knee against resistance.

14
Hamstring Strain Forceful hamstring contraction (concentric) or knee extension (eccentric) Stretch or tear of muscle or tendon “pulled” muscle Grade I strain – Grade III complete tear

15
Evaluate Swelling Bruising Tenderness to palpation over muscle belly
Pain when stretching the muscle Pain with resisted contraction of the muscle

16
Hamstring Strain RICE Weight-bearing reduction if needed Imaging
Gentle Stretching Strengthening Thigh Wrap for support

17
Case 3 A 16 year old girl complains of sharp pain in the left knee. She was “cutting” to the left to avoid her opponent when she felt and heard a loud painful “pop” in her knee. Her knee immediately began to swell and feels stiff. When she tries to bear weight on her left leg she feels that the knee will give way. On exam she has visible swelling of the left knee. There is tenderness along the joint line of the knee. She is unable to fully bend or straighten her knee.

18
Anterior Cruciate Ligament (ACL) Tear
Most commonly injured knee ligament in athletics One of major ligaments in middle of the knee Connects femur to tibia Keeps the knee stable Cutting, deceleration, hyperextension

19
ACL Tear Noncontact injuries most common
Contact injuries may involve other structures MCL Medial Meniscus Increased Female Lax ligaments Knock Knee

20
Evaluate Swelling Tenderness along the joint lines of the knee
Range of Motion Anterior Drawer test

21
ACL Tear RICE Partial Weight Bearing Imaging Physical Therapy Surgery?
Goal complete rehab in 1 year

22
Case 4 A 14 year old boy presents to the emergency room having jammed his middle finger during a basketball game. There is significant swelling at his PIP joint with displacement of his middle phalanx in relation to the proximal phalanx. He is unable to flex or extend his finger secondary to pain. Sensation on the medial and lateral border of the digit is intact with normal capillary refill.

23
Dislocation Moves out of joint Finger Immediate pain
Jammed force to end of joint Twisting Hyperextension Immediate pain

24
Shoulder & Knee/Patella

25
Evaluate Deformity Unable to bend/straighten dislocated joint
SPLINT AS IS!!!

26
Finger Dislocation X-ray Realignment Splint/Buddy Tape 3 – 6 weeks
Fracture Realignment Splint/Buddy Tape 3 – 6 weeks RICE Occupational Therapy Stretching/ROM Strengthening

27
Case 5 A 17 year old girl slides into second base while playing softball and collides with the second baseman. She immediately hears a snap and feels pain in her leg. She is unable to stand or weight bear on the leg and there is an obvious deformity of the lower leg. She has sensation throughout the leg but is unable to move the leg.

28
Fracture Broken Bone = Emergency Care EMS/9-1-1 Splint AS IS
Severe Pain Hear/feel snap Difficult to move/weight bear on injured part Injured part moves unnaturally Visible Deformity EMS/9-1-1 Splint AS IS

29
Fracture Simple Comminuted Closed Open (Compound)
One fracture line, bone is broken into 2 pieces Comminuted More than one fracture line with more than 2 bone fragments at the fracture site Closed Skin in fracture area is not broken, break is not exposed to the outside Open (Compound) Skin over the fracture is broken, exposing the broken bone
 Skin over the fracture is broken, exposing the broken bone.")
30
Fracture

31
Growth Plate Injuries/Fractures
Where bone is growing Weakest during growth spurt Female 10 – 11 yo → 15 – 17 yo up to 3”/yr Male yo → 16 – 17 yo up to 4”/yr Cessation of growth Limb length discrepancies

32
Acute Injuries Eye Injury Dental Emergency DENTIST
Cover with Paper Cup Doctor/ED Dental Emergency Lost/Broken tooth Sterile gauze moisten with saline/milk Out from socket Rinse with saline/milk Place back in socket DENTIST

33
Chronic Injuries Overuse Newer Phenomenon
Repetitive action with too much stress on musculoskeletal system without adequate recovery time Newer Phenomenon Used to play different sports/season Now year round training

34
Causes of Overuse Injuries
#1Training Errors Too much, too soon, too fast Problem with equipment - growth Environmental Conditions Hot Dehydration → muscle dehydrated = increase risk of injury Cold Decrease blood flow to muscle

35
Causes of Overuse Injuries
Poor Nutrition Inadequate Hydration Anatomic Misalignment Knock kneed, bow legged, flat feet, high arches Muscle Imbalance Growth Spurt Tighter muscles decrease flexibility Prior Injury Deconditioning or Out of Shape!

36
Shin Splints Microscopic tearing of muscle attaching to bone on shins
Pain, inflammation & irritation along leg Repeated running on hard surface/hills Tx: RICE Arch Support Stretching Strengthening Decrease mileage

37
Osgood-Schlatter Disease
Pain at Tibial Tuberosity where tendon attaches from patella Rapid growth 10 – 15 years old Overuse Tight quads, hamstring, calf muscles Painful bump below knee

38
Osgood-Schlatter Disease
RICE Pain Free Activities Strengthening Stretching 6 – 24 months from start of pain to resolve Return when Bump not painful Pain free ROM Jog, sprint, cut, jump pain free

39
Patellofemoral Pain Syndrome (Runner’s Knee)
Pain around/behind the kneecap Walk, run, sit long period of time, downhill, downstairs Intermittent knee swelling RICE Knee Brace/Shoe Orthotic Physical Therapy Strengthen VMO

40
Growth Plate Overuse Injuries
Little Leaguer’s Shoulder Proximal Humeral Epiphysitis Overuse of growth area of the humerus with widening of growth plate Little Leaguer’s Elbow Medial Apophysitis Medial epicondyle pain Muscles that bend the wrist attach to medial epicondyle

41
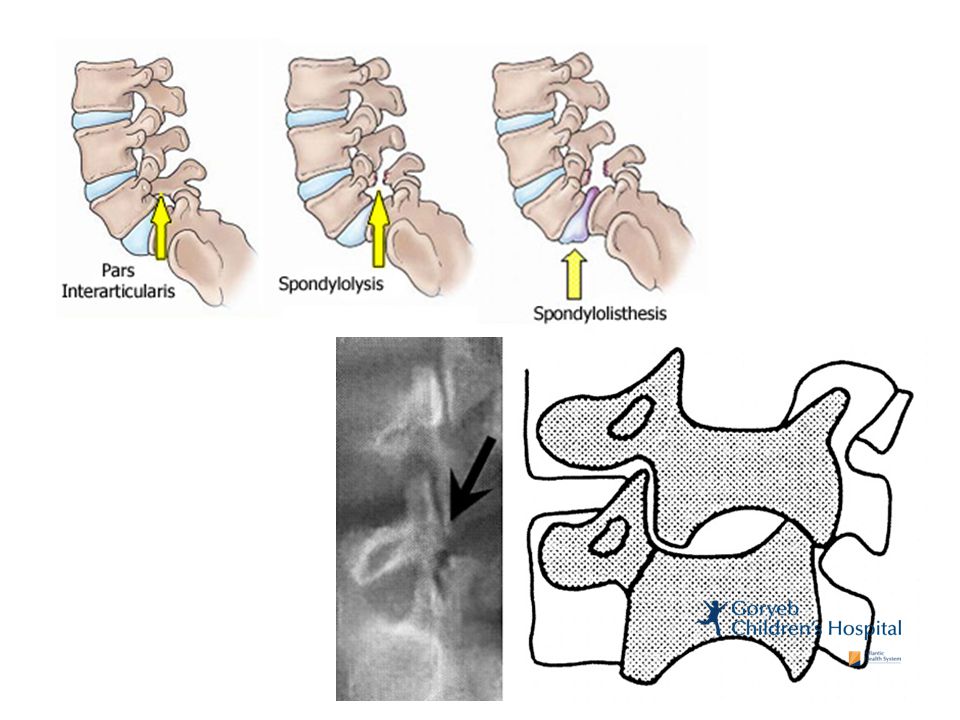
Stress Fracture Lower Body Injury without insufficient recovery
Shin Foot Toes Injury without insufficient recovery Avoid Impact Boot to quicken healing Back (Spondylolysis) Fracture of pars interarticularis Hyperextension Twisting Gymnastics, dancing, skating, football Bracing 3 – 9 months PT
 Fracture of pars interarticularis. Hyperextension. Twisting. Gymnastics, dancing, skating, football. Bracing 3 – 9 months. PT.")
43
Prevention Re injury most common injury Proper warm up/stretching
Return to sport before sufficient healing and recovery is not complete Increase risk of injury to adjacent body part Proper warm up/stretching Pace self, ease back into sport Proper Equipment Safe playing surface Adequate adult supervision & safety Prepare child for sport training/conditioning

44
Prevention Trust Body Cues Listen to “I’m Tired” Rest Days
Pain/sore Listen to “I’m Tired” Rest Days Vary intensity of the workout Vary the type of physical activity Hydration 8 oz. beyond thirst prior to game 4 – 8 oz. every min during activity

45
? Concussion ? 18 yo Female falls off bicycle
17 yo Male falls off skateboard and lands on knees 16 yo Female hits head on metal bed frame 10 yo Male is hit in the head with books when opening his locker

46
Does your management change if:
Feels totally fine Is dizzy, but really wants to play because today is the final practice before decision is made on who makes the team Feels fine, but on exam balance is terrible Mom is standing right behind you giving you the stink eye

47
Concussion May be caused by a direct blow to the head, face, neck or elsewhere on the body with an “impulsive” force transmitted to the head

48
Biokinetics of Concussion
Acceleration-deceleration and rotational forces Helmet?

49
Typically results in the rapid onset of short-lived impairment of neurologic function that resolves spontaneously May result in neuropathological changes, but the acute clinical symptoms largely reflect a functional disturbance NOT a structural injury

50
Pathophysiology of Concussion
Brain obligate aerobic organ fueled by glucose delivered via blood circulation Brain activity increases = blood flow to brain increases Coupled relationship of oxygen and glucose

51
Consequences Mismatch of metabolic supply and demand may = cell dysfunction, increased cell vulnerability to second traumatic insult/stress Each insult need to consider if insult initiated above chemical cascade No abnormality on STANDARD structural neuroimaging studies is seen Newer imaging is showing evidence of injury Functional MRI

53
Classification of Concussions
Consensus Statement Zurich 2012: ABANDONED Simple vs. Complex & Grading terminology Majority 80 – 90% resolve in a short (7 – 10 day) period Recovery time frame may be LONGER in children and adolescents
 period. Recovery time frame may be LONGER in children and adolescents.")
54
Epidemiology 8.9% of all reported high school athletic injuries
F > M in similar sports ? F weaker neck muscles and smaller head mass? ? M more reluctant to report injury? Football, F Soccer, M Lacrosse, M Soccer, F Basketball, Wrestling, F Lacrosse, Softball, M Basketball, M & F Volleyball, Baseball

55
Pre-season Baseline Testing
Standard Pre-participation Sports Physical Concussion History including any head, face, or cervical spine injuries where concussions may have been missed Identify athletes that fit into a high risk category = education/prevention opportunity Neurocognitive Testing - baseline

56
“My cat’s OK I can play, I got my cat scanned”

57
Symptoms Immediate Sleep Disturbance Headache Dizziness Double Vision
Nausea Light/Sound Sensitivity Feeling Foggy LOC Amnesia Behavioral Changes Cognitive Impairment Sleep Disturbance

58
On-field/Sideline Evaluations
Cervical Assessment on Field Address first aid issues Any Suspicion of concussion REMOVE NFL Docs “eye in the sky” SCAT3 – rapid sideline screening 3_(2013).pdf Serial monitoring for deterioration over next few hours
.pdf. Serial monitoring for deterioration over next few hours.")
59
Management Physical and Cognitive REST until symptom RESOLUTION
Do NOT need to awaken throughout the night, observe for normal breathing pattern “Cocoon Therapy” AKA a whole list of what you CANNOT do VS. Do what you can tolerate/does not worsen symptoms “fastest way to recovery and stop spending time with me is to listen to your symptoms. You cannot push through a concussion”

60
Management Wear sunglasses if photophobia
Sleep in a dark room as much as possible 2 – 3 days, then try to resume normal sleep/wake hours and nap 15 – 20 minutes Gradually increase exposure to telephone, music, TV by 15 minute intervals as long as symptom free Feeling better danger zone Light Activity Over Sleeping

61
Management: Medications
Avoid and let symptoms be your guide Extreme headache Rx or OTC but avoid over use Masking symptoms Rebound headaches Melatonin Sleep Headaches

62
School Considerations
Attendance Visual Stimulus Workload Physical Exertion Breaks Audible Stimuli Testing Concussion Team at School?

63
Return to Play (RTP) Symptom free & off medication
Exception: antidepressants Neurocognitive Testing Objectively evaluate condition, track recovery Measures symptoms, verbal & visual memory, processing speed, reaction time Gradual RTP Protocol: Proceed 1 level at a time if asymptomatic at current level 24 hrs per level = 1 week to proceed through full rehabilitation protocol Any symptoms = drop down to asymptomatic level x 24hrs before proceeding May stretch out RTP if < 13 years old

64
Pediatric & Adolescent Considerations
All recommendations are for ages 10 & up Less than 10 years old, report symptoms differently Need to include both child & parent input as well as teacher and school input when appropriate Neuropsychological testing & Neuropsychologists may play a larger role for school planning/academics Learning disabilities & ADHD May take longer to symptom free = prolonged RTP NO same day RTP Cognitive rest may require absence from school or modified work load HUGE STRESSOR!!!!!!!!

65
Prevention Helmets Do Not Prevent Concussions!
Helmets/Headgear New bike helmet following impact Football helmets reduce impact force to head but not concussion incidence Soccer head gear unclear utility, heading can be performed safe? & avoidance does not prevent concussion Headgear increasing head injuries: female lacrosse, soccer EDUCATION Athletes, Parents, Coaches, Athletic Trainers, Physicians, Health Care Providers, etc.

66
Long Term Effects Chronic Traumatic Encephalopathy
Seen in 18-year old multisport athlete with a history of concussions from football upon autopsy New football, soccer 3 or more concussions Increased LOC, post-amnesia, confusion 8 – 16 yo persistent deficits in processing complex visual stimuli Athletes with 2 or more concussions who are concussion free x 6 months performed similarly on NP testing as athletes with 1st concussion in last week 2 or more concussions lower GPA

67
Second-Impact Syndrome
Sustain an initial head injury then second injury before symptom free from first head injury Cerebral vascular congestion → diffuse cerebral swelling → death Pediatric & Adolescents at higher risk for rare condition All reported cases are of athletes < 20 yo. Catastrophic football head injuries 3x more likely in high school than in college athletes

68
Retirement From Sport Consider when sustained 3 concussions in an individual season or more than 3 months of symptoms

70
These Parents are Cray

71
Returning Too Soon “But I CANNOT fall behind in school!”
“But she HAS to take those tests tomorrow!” “But it’s a REALLY important game!” “But I am kinda a BIG DEAL!” “The coach is going to KILL me!” “The coach is going to kick her off the team!” “If he misses this season how can he become a professional _______ and I can retire?!?!”

73
Talking the Students and Parents off the Ledge:
If you are injured you are not going to perform your best You are not going to be the best contribution for your team You will take longer/not heal It is easier to reinjure yourself You are first a child then a student & athlete Your health is most important Believe it or not the world will go on!

74
References Kids & Sports by Eric Small, MD
Mild Traumatic Brain Injury in Children and Adolescents by Michael W. Kirkwood & Keith Owen Yeates The Sports Medicine Patient Advisor Third Edition by Pierre Rouzier, MD Consensus Statement on Concussion in Sport 4rd International Conference on Concussion in Sport Held in Zurich, November 2012 Physical Medicine and Rehabilitation Board Review Sports-Related Cervical Spine Injuries: On-Field Assessment & Management Effect of Amantadine on Post-Concussive Symptoms Poster Presentation Clinical Report – Sport-Related Concussion in Children and Adolescents

75
Thank You!

Similar presentations













>")


 >")





