Download presentation
Presentation is loading. Please wait.

2
Diabetic Foot An Overview Foot team Prof.Mamdouh El Nahas Prof.Hanan Gawish Dr. Manal Tarshoby Dr.Omnia State Prof.Mamdouh El Nahas. Hanan Gawish Dr Manal Tarshoby. Dr.Omnia State.

3
Put Feet First Prevent Amputations Diabetes and Foot Care World Diabetes Day 2005

4
2005: a Year-long Campaign

5
Campaign Objectives Inform people of the extent of diabetic foot problems worldwide. Persuade people that action is both possible and affordable. Warn people of the consequences of not taking action.

6
FOOT FACTS (1) Every 30 seconds a leg is lost to diabetes somewhere in the world. Up to 70% of all leg amputations happen to people with diabetes. DF problems are the commonest cause of hospital admission. (by us?)
.")
7
FOOT FACTS (2) Most amputations begin with a foot ulcer. One in every six people with diabetes will have a foot ulcer during their lifetime. Good News Up to 85% of amputations can be avoided.

8
Egypt Representative Mansoura University Prof.Mamdouh El Nahas. Dr.Hanan Gawish Dr. Manal Tarshoby Dr.Omnia Stat

9
Levels of foot management Level 1 General practitioner, diabetic nurse and podiatrist Level 2 Diabetologist, surgeon (general and/or vascular and/or orthopedic), diabetic nurse and podiatrist Level 3 Specialized foot center
, diabetic nurse and podiatrist Level 3 Specialized foot center")
10
Value of Podiatric Care KINGS COLLEGE HOSPITAL. 1984 establishment of DIABETIC FOOT CLINIC. Amputation decreased 50% in 3 years.

11
Diabetic Foot

12
Diabetic Foot Disease Ischaemia Neuropathy Infection Structural deformity Ulcer Amputation

13
Five cornerstones of the management of the diabetic foot Regular inspection and examination of the foot. Identification of the foot at risk. Education of patient, family and healthcare providers. Appropriate footwear. Treatment of non ulcerative pathology

14
Five cornerstones of the management of the diabetic foot Regular inspection and examination of the foot. Identification of the foot at risk. Education of patient, family and healthcare providers. Appropriate footwear. Treatment of non ulcerative pathology

15
Regular inspection and examination of the foot All diabetic patients should be examined at first presentation then at least once a year Patients with risk factors should be examined every 1-6 months Absent symptoms does not mean that the feet are healthy Examine the patient on lying down and standing up Shoe and socks should be inspected

16
History Previous ulcer, amputation Previous foot education Bare-foot walking Poor access to healthcare Smokimg, alcohol Nephropathy,Retinopathy Hypertension Ischemic heart disease

17
Foot examination 1.Nails Thick too long ingrown fungal infection wrongly cut nails

18
Foot Examination 2.Foot deformity:

19
Foot Examination 2.Foot deformity: Toe deformity Hammer toeHammer toe Claw toeClaw toe

20
Toe Deformity:– Hammer Toe Increased pressure on 2 nd metatarsal head Increased pressure on prox. IPJ Increased pressure on distal IPJ Increased pressure on apex Increased pressure on nail fold

21
Foot Examination 2.Foot deformity: Toe deformity Forefoot deformity Hallux valgus Hallux valgus Hallux rigidus Hallux rigidus

22
Hallux Valgus

23
Hallux Rigidus Osteoarthritic Degeneration 1 st MTP Joint Limitation of Dorsiflexion Overloading 2 nd MTP Joint / 1 st IPJoint

24
Foot Examination 2.Foot deformity: Toe deformity Forefoot deformity Wholefoot Deformities Wholefoot Deformities Pes Cavus - High arched foot Pes Cavus - High arched foot Pes Planus - Flat foot Pes Planus - Flat foot Charcot foot Charcot foot

25
Diagnosis of Acute Charcot Painless Redness, swelling, and more than 2°C skin temperature difference when compared with the contralateral foot. Dorsalis pedis pulses are often bounding. The patient is afebrile unless a systemic infection is present.

27
Foot Examination 2.Foot deformity: Toe deformity Forefoot deformity Whole foot Deformities Whole foot Deformities Prominent metatarsal heads Prominent metatarsal heads

28
Foot Examination 3.Skin condition: Callus Bunions Callus Bunions Redness Warmth Redness Warmth Fissure Dryness Fissure Dryness Swelling Maceration Swelling Maceration Fungal infection Fungal infection

29
Callus Presence of callus is a significant marker for the development of foot ulceration The hyperkeratosis is a result of hypertrophy under the influence of intermittent compression. the callus is either a reaction to abnormal pressure or an abnormality of the area to handle normal pressure.

30
Tenia Pedis

31
Foot Examination 4.Vascular assessment: History Intermitent claudication Intermitent claudication Rest pain Rest pain Colour of the skin Temperature gradient

32
Foot Examination 4.Vascular assessment: Pedal pulse Dorsalis pedis Dorsalis pedis Posterior tibial Posterior tibial

33
Foot Examination 4.Vascular assessment: Pedal pulse Dorsalis pedis Dorsalis pedis Posterior tibial Posterior tibial Ankle Brachial Pressure Index

34
Foot Examination 5.Neurological assessment: Tempreature Vibration Sense Touch and Pressure Light Touch Proprioception (Romberg’s Sign) Superficial Pain Reflexes
 Superficial Pain Reflexes")
35
Neurologic assessment Temperature Vibration Sense Pressure Sense Light Touch Proprioception Reflexes

36
Neurologic assessment

37
Temperature Vibration Sense Pressure Sense Light Touch Proprioception (Romberg’s Sign) Superficial Pain Reflexes
 Superficial Pain Reflexes")
38
TEMPERATURE TESTING Two test tubes, hot/cold. Therm-tip Subjective, crude tests

39
Neurologic assessment Temperature Vibration Sense Pressure Sense Light Touch Proprioception Superficial Pain Reflexes

40
VIBRATION SENSE

41
NEUROTHESIOMETER

42
Neurologic assessment Temperature Vibration Sense Pressure Sense Light Touch Proprioception Superficial Pain Reflexes

43
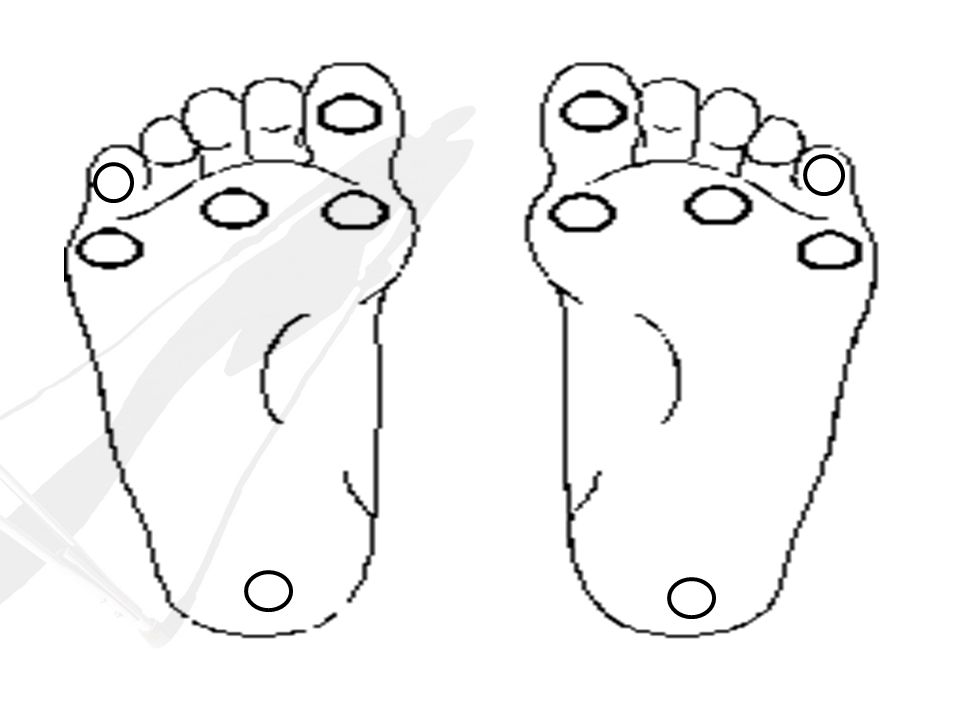
MONOFILAMENTS 10 gm Sites tested Technique Significance

45
Neurologic assessment Temeprature Vibration Sense Pressure Sense Light Touch Proprioception Superficial Pain Reflexes

46
LIGHT TOUCH TEST

47
Neurologic assessment Temperature Vibration Sense Pressure Sense Light Touch Proprioception Superficial Pain Reflexes

48
PROPRIOCEPTION TEST Tested by dorsiflexing and plantarflexing the hallux. Can the patient determine the position of the hallux?

49
Neurologic assessment Temperature Vibration Sense Pressure Sense Light Touch Proprioception Superficial Pain Reflexes

50
SUPERFICIAL PAIN TEST

51
Neurologic assessment Temperature Vibration Sense Pressure Sense Light Touch Proprioception Superficial Pain Reflexes

52
ANKLE REFLEX

53
Five cornerstones of the management of the diabetic foot Regular inspection and examination of the foot. Identification of the foot at risk. Education of patient, family and healthcare providers. Appropriate footwear. Treatment of non ulcerative pathology

54
Risk Categorization

55
Risk categorization system Check- up frequency Risk profile Category once a yearno sensory neuropathy0 once every 6 months sensory neuropathy1 once every 3 months sensory neuropathy and signs of peripheral vascular disease and/or foot deformities. 2 once every month previous ulcer3

56
Five cornerstones of the management of the diabetic foot Regular inspection and examination of the foot. Identification of the foot at risk. Education of patient, family and healthcare providers. Appropriate footwear. Treatment of non ulcerative pathology

57
Five cornerstones of the management of the diabetic foot Regular inspection and examination of the foot. Identification of the foot at risk. Education of patient, family and healthcare providers. Appropriate footwear. Treatment of non ulcerative pathology

58
Five cornerstones of the management of the diabetic foot Regular inspection and examination of the foot. Identification of the foot at risk. Education of patient, family and healthcare providers. Appropriate footwear. Treatment of non ulcerative pathology

59
What is going on??

60
Foot care team ??Podiatrists Orthotists. Diabetologists. Vascular Surgeon. Educators. Microbiologist.

61
Ulcer assessment 1.Establish the ulcer's etiology 2.Measure its size 3.Establish its depth and involvement of deep structures 4.Examine it for purulent exudates, necrosis, sinus tracts, and odor 5.Assess the surrounding tissue for signs of edema, cellulitis, abscess, and fluctuation 6.Exclude systemic infection 7.Perform a vascular evaluation. 8.The ability to gently probe through the ulcer to bone has been shown to be highly predictive of osteomyelitis. ( should be recorded at base line and every subsequent visits ± digital photo)
.")
62
A multidisciplinary approach providing debridement, meticulous wound care, adequate vascular supply, metabolic control, antimicrobial treatment and relief of pressure (offloading) is essential in the treatment of foot ulcer.
 is essential in the treatment of foot ulcer.")
63
Dressing Do not put anything on the ulcer that you wouldn’t put in your eye!! No evidence from large trials

64
Debridement Sharp Larval Enzymatic (Lytic) Indication & Contraindication??
 Indication & Contraindication")
65
Offloading

66
Offlaoding What is meant by offloading Different offloading modalities

67
Key Message Of all late complications of diabetes, foot problems are the most easily detectable and easily preventable. Relatively simple interventions can reduce amputations by 50 - 80%. (Bakker et al 1994). Strategies aimed at preventing foot ulcers are cost effective and cost saving. Only champions willing to act are needed.
. Strategies aimed at preventing foot ulcers are cost effective and cost saving. Only champions willing to act are needed..")
68
Don’t Forget to take your copy!

69
Thanks for sharing!!!!

Similar presentations


 (Physicians Name Here) (Practice Name Here) (Practice Address Here) (Practice Phone Number Here) (Practice Website Here)>")














 MBAPO SR P/O Senior Orthotist IDS Cappagh Hospital.>")



