Download presentation
Presentation is loading. Please wait.

1
Selecting Younger or Older Living Kidney Donors based on ‘Normal for Now’ or ‘At Future Risk’ Reference: Steiner RW. ‘Normal for Now’ or ‘At Future Risk’: A double standard for selecting young and older living kidney donors. Am J Transplant. 2010;10:737–741.

2
Introduction Potential living kidney donors are medically evaluated by transplant centers, to determine their baseline remaining lifetime risk for end-stage renal disease (ESRD). Several centers are likely to refuse a donor when an isolated medical abnormality (IMA) like mild hypertension, nephrolithiasis, idiopathic isolated microscopic hematuria or low-grade dipstick negative proteinuria is uncovered in the donor evaluation. However, a normal medical evaluation in a young donor may provide little assurance of reduced baseline lifetime risk of ESRD, because overt renal disease or medical findings that are risk factors for renal disease (IMAs) may not be apparent 30 or 40 years before ESRD develops.
 like mild hypertension, nephrolithiasis, idiopathic isolated microscopic hematuria or low-grade dipstick negative proteinuria is uncovered in the donor evaluation. However, a normal medical evaluation in a young donor may provide little assurance of reduced baseline lifetime risk of ESRD, because overt renal disease or medical findings that are risk factors for renal disease (IMAs) may not be apparent 30 or 40 years before ESRD develops..")
3
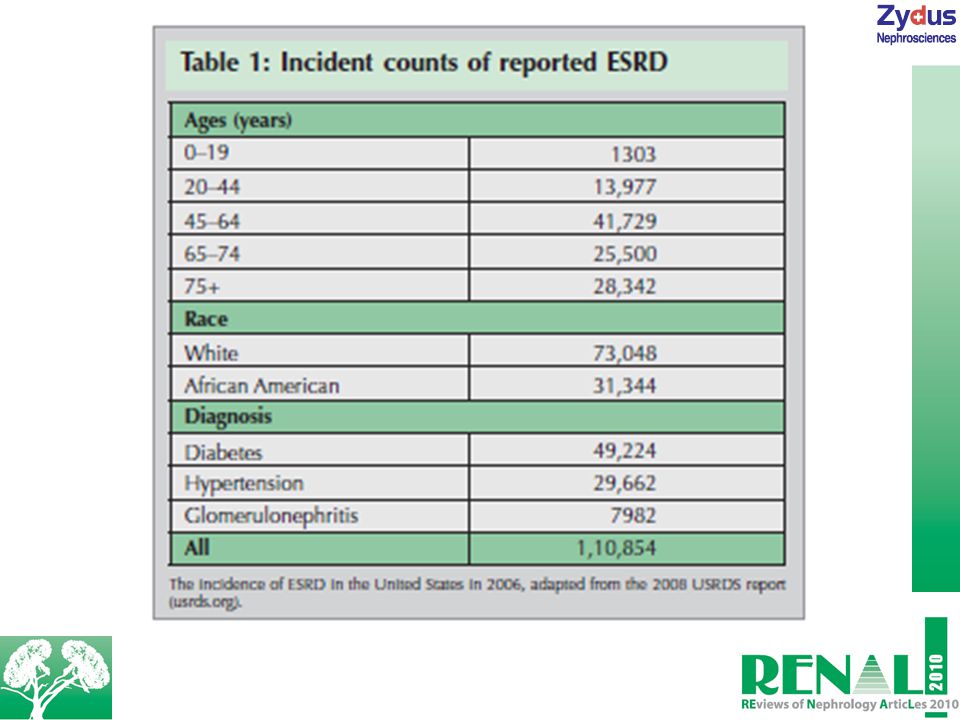
United States Renal Disease System: Data Pool for Donor Risk Appreciation A basis for donor risk appreciation is available from the United States Renal Disease System (USRDS) data on the yearly incidence of ESRD in the US. Here, diabetes accounted for about half (45%) of the incident cases of ESRD, both before and after the age of 65 years, with 90% of cases from type II diabetes; ESRD was attributed to hypertension in an additional 27%, with glomerulonephritis in third place at 8%. However, the median ages at diagnosis of ESRD for these three categories were 64, 71 and 58, respectively, in the 2002–2006 cohort. Overall, the USRDS data suggest that most individuals, who will have normal donor medical evaluations at the age of 25 years, will go on to develop diabetes and diabetic nephropathy in later life; which is similar to those who will typically develop other kinds of ESRD in later life. The strong infl uence of older age and particularly type II diabetes suggests a signifi cant later-life risk for young ‘normal’ donor candidates and for young black donors in particular (see Table 1).
 of the incident cases of ESRD, both before and after the age of 65 years, with 90% of cases from type II diabetes; ESRD was attributed to hypertension in an additional 27%, with glomerulonephritis in third place at 8%. However, the median ages at diagnosis of ESRD for these three categories were 64, 71 and 58, respectively, in the 2002–2006 cohort. Overall, the USRDS data suggest that most individuals, who will have normal donor medical evaluations at the age of 25 years, will go on to develop diabetes and diabetic nephropathy in later life; which is similar to those who will typically develop other kinds of ESRD in later life. The strong infl uence of older age and particularly type II diabetes suggests a signifi cant later-life risk for young ‘normal’ donor candidates and for young black donors in particular (see Table 1)..")
5
The starting point for individual risk estimation is the lifetime risk for ESRD for the general population. This risk is reportedly increasing, but historically it has been estimated by complex methodology to be 2–2.5% in whites and 7–8% in blacks. According to the Minnesota study, only about a one-third reduction occurred in ESRD in former donors whose age averaged 40 years at the time of donation compared to the general population. Thus a normal donor evaluation may reduce the risk in some donor candidates, but cannot completely protect against the epidemiological determinants for ESRD, most of which occurs in later life.

6
Medical Evaluation for Risk Stratification It is diffi cult to estimate how much reassurance can be expected from a normal medical evaluation in a young donor candidate. Medically, normal older donor candidates have relatively less remaining lifetime risk for ESRD. In the case of the donor medical evaluation identifying all the nondiabetic 55-year-old donor candidates who would not develop ESRD over only the next 10 years, their remaining lifetime risk would be about 25% of the baseline. This is owing to the reason that half of lifetime ESRD will occur before the age of 65 years, and about half of ESRD after the age of 65 years occurs after around 25 years of diabetes. This makes it possible for looking successfully 10 years into the future to reduce the lifetime risk of these 55-year-olds by 75%. However, it would also require looking 20 years into the future just to reduce the 24-year-old donor’s risk by about 10%. In a nutshell, younger the donor, greater is the remaining baseline lifetime risk for ESRD.

7
About 25% of the US population is diagnosed with hypertension, and its prevalence is proportional with age. It is seen that several of the incidence of renal disease is mistakenly diagnosed and reported to the USRDS as primarily hypertensive, whereas hypertension occurs secondary to and exacerbates various renal diseases. As a result, it has been questioned whether essential hypertension ought to be considered as a signifi cant cause of ESRD in the general population. Moreover, besides being infrequent, the progression of hypertension is characteristically indolent when hypertensive renal impairment occurs. Kidney donation always sacrifi ces glomerular fi ltration rate (GFR), and consequently it will speed the onset of eventual ESRD for young and old donors alike. Profi ling health effects of the reduction in post donation GFR in all donors and predicting the rate of progression of newly developed, postdonation kidney disease are independent and diffi cult issues. The latter risk is most often cited when IMA donors are refused, because of uncertainty about the added risk of nephrectomy, as well as an ethical concern about knowingly accepting donors at an identifi able risk for ESRD.
, and consequently it will speed the onset of eventual ESRD for young and old donors alike. Profi ling health effects of the reduction in post donation GFR in all donors and predicting the rate of progression of newly developed, postdonation kidney disease are independent and diffi cult issues. The latter risk is most often cited when IMA donors are refused, because of uncertainty about the added risk of nephrectomy, as well as an ethical concern about knowingly accepting donors at an identifi able risk for ESRD..")
8
Donor Risk Estimation Defi nitely foretelling whether the remaining baseline lifetime risk of ESRD for several middle-aged donors with hypertension or some other IMA is marginally greater, the same or marginally less than the risks for many younger ‘normal for now’ candidates is not possible. However, there is no ethical justifi cation for accepting younger donors and categorically refusing all older IMA donors, because risks can be shown to be similar with the other factors being equal. Moreover, middle-aged donors as a group may be in a better position to make realistic, mature judgments on the impact of eventual ESRD on their remaining lifetimes than are donors in their 20s, who may well not face ESRD for the next 40 years. As a result, transplant centers have very defi nite choices to make as they select their donors to remain ethically consistent. When young normal donors are accepted, middle-aged mildly hypertensive donors cannot be categorically rejected as ‘too risky,’ while in fact they have the same or less risk as normal young donors. Similarly, if older donors are categorically refused owing to the reason that their baseline lifetime risk for ESRD is ‘too high,’ any younger donors cannot be ethically accepted as well.

9
Conclusion At present, transplant centers may not be adequately assessing baseline ESRD risk of young ‘normal for now’ donor candidates and may have inadvertently adopted internally inconsistent donor selection standards. Based on the continuum of risk and the multiplicity of risk factors, categorically refusing young donors ‘at diabetic risk’ would be difficult to defend. Obviously, almost 50% of the baseline lifetime risk for ESRD would remain even if all the young donors who would eventually develop diabetic ESRD were improbably identified and excluded. Finally, the answer does not rest in necessarily giving up the young donors or discontinuing living donor kidney transplants altogether, but could rather be for centers to impartially and dispassionately quantify risks, decide what risks are reasonable, teach donors what these risks are and test them to see that they understand. As more individuals in the field apply themselves to this task, the risk estimates will certainly improve. Yet, the basic imperative to always define and explain risk in living kidney donor selection will remain the same.

Similar presentations







 of organ donors:>")



. Comparison of the effects of losartan and enalapril on renal function in adults with chronic kidney disease at.>")







 A joint program of NIH and CDC Diabetes: The Numbers Revised.>")