Download presentation
Presentation is loading. Please wait.

1
Effect of Obesity on Kidney Transplantation Reference: Potluri K, Hou S. Obesity in kidney transplant recipients and candidates. Am J Kidney Dis. 2010;56:143–156.

2
The rate of obesity in patients starting dialysis therapy has outpaced the frequency of obesity and morbid obesity in the population as a whole. Several transplant centers have set a body mass index (BMI) limit for patients being accepted for transplant at 30 or 35 kg/m2. This is because it is believed that obese patients have more complications and, shorter transplant and patient survival than ideal-weight patients.
 limit for patients being accepted for transplant at 30 or 35 kg/m2. This is because it is believed that obese patients have more complications and, shorter transplant and patient survival than ideal-weight patients..")
3
Consequences of Obesity at the Time of Transplant Obese organ transplant recipients are at a higher risk owing to immunosuppressive drugs, which can further delay wound healing and increase the risk of infection in the postoperative period. At the time of transplant, obesity is associated with lower patient and transplant survival and a higher risk of coronary artery disease. However, despite the reluctance of transplant centers to perform transplant on obese patients, the percent-age of transplant recipients with BMI 30 kg/m2 increased from 11.6% in 1987–1989 to 25.1% in 2000–2001. One of the most frequently reported problems in obese kidney transplant recipients include wound complications. Some of the possible explanations for wound complications include longer surgical times, less resistance of adipose tissue to infection, and hyperglycemia from insulin resistance. Hypertension, hyperlipidemia, and type 2 diabetes seen at higher incidence in obese patients, are important risk factors that are responsible for transplant loss. Posttransplant diabetes mellitus is a common complication of kidney transplant and increasing risk of developing diabetes in obese transplant patients has been reported in multiple studies.

4
‘Lose Weight’ or ‘No Transplant’? Although, weight loss is desirable, it is often difficult to achieve weight loss in dialysis patients as in the general population. This is particularly seen in peritoneal dialysis patients, who get an extra caloric load from the dialysis fluid. Preferably, dialysis patients with BMI 35 kg/m2 should lose weight before transplant; however, often this is not the case. Providing transplant in obese individuals should be framed in terms of benefit for the individual patient or in terms of the best use of limited resources. It must be considered that when an obese patient with a directed living donor is refused a transplant based solely on BMI, a patient who potentially will have greater success long term with transplant is denied of such an advantage.

5
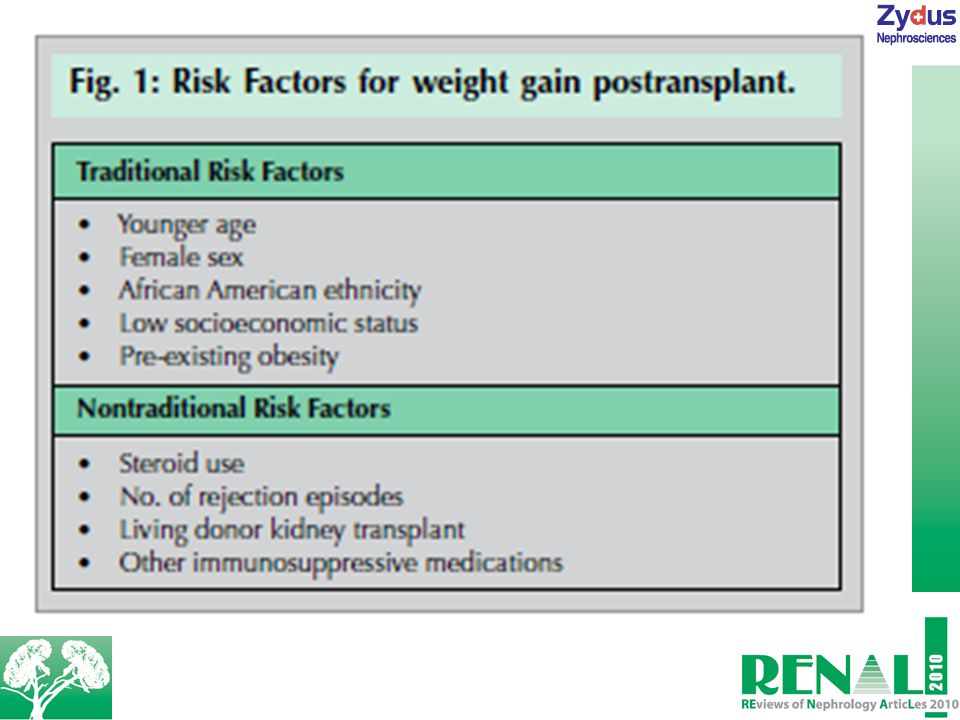
Posttransplant Weight Gain Weight gain post-kidney transplant is relatively common, with an average weight gain reported to be 8–14 kg, 1 year posttransplant. An adverse effect of long-term steroid use in the general population is excessive weight gain and redistribution of fat to undesired areas. Doses of steroids currently used in transplant recipients are much lower than in the past and generally lower than doses used to treat kidney diseases. Other factors may also have a role in weight gain (see Fig. 1).
..")
7
Drug Monitoring in Obese Patients In the first few years after transplant, close monitoring of blood levels of some immunosuppressive medications are required owing to the narrow toxic therapeutic ratio and drug interactions. However, the pharmacokinetics of some drugs is changed in obese patients. It has been reported that higher cyclosporine concentrations occurred in obese patients when it was dosed per kilogram of body weight.

9
Therefore, dosing based on ideal body weight has been suggested. Similarly, another study reported achieving similar cyclosporine levels at 0 and 2 h in obese patients with lower cyclosporine doses than used in normal-weight adults. Older and obese transplant patients were also prone to higher tacrolimus trough levels when the drug was dosed by body weight. It has been suggested that drug exposure to mycophenolic acid correlated with weight and recommends dosing mycophenolic acid at 12 mg/kg of body weight to attain adequate levels.

10
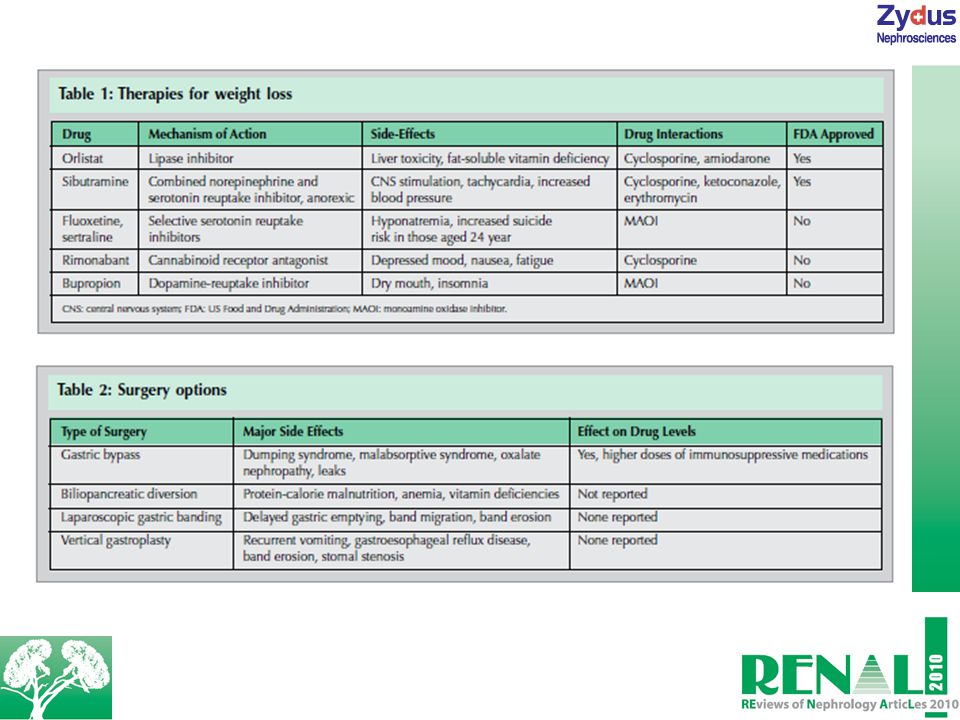
Treatment Alternatives for Obese Kidney Transplant Patients Although sustained weight loss through conservative lifestyle intervention is difficult to achieve and awaits some new hypothalamic insight, prevention of weight gain is a more feasible goal. Indeed, intensive emphasis on lifestyle modifications at the time of transplant is reported to prevent weight gain. As an adjunctive to lifestyle modifications, pharmacological treatment for weight loss can be utilized, particularly in patients with BMI>30 kg/m2. Although, drug therapy is limited in its effectiveness, a weight loss of 10–15% is considered a very good response. However, maintaining weight loss is always challenging. Despite the consequences, these drugs provide alternative options for obese patients who cannot lose weight with dietary restriction alone (see Table 1). Surgical options like those listed in Table 2 can be considered for highly motivated patients who are morbidly obese, as nonsurgical therapies fail in such patients. In the general population, bariatric surgery is recommended for morbidly obese patients with BMI>35 kg/m2 with comorbid conditions and BMI>40 kg/m2 regardless of co-morbid conditions.
. Surgical options like those listed in Table 2 can be considered for highly motivated patients who are morbidly obese, as nonsurgical therapies fail in such patients. In the general population, bariatric surgery is recommended for morbidly obese patients with BMI>35 kg/m2 with comorbid conditions and BMI>40 kg/m2 regardless of co-morbid conditions..")
11
Conclusion Obesity at the time of transplant is a major risk factor for complications posttransplant. Moreover, weight gain posttransplant is a frequent complication, increasing the risk of obesity-related complications in previously normal-weight people. Besides encouragement of lifestyle modification, available pharmacological and surgical options should be evaluated in appropriate patients. Close monitoring of immunosuppressive medications after pharmacological and/or surgical interventions is also another important factor owing to variability in drug absorption in obese patients.

Similar presentations












 and Drug Therapy in Different Risk Categories Risk Category LDL Goal (mg/dL)>")






