Download presentation
Presentation is loading. Please wait.

1
Neuropsychological Aspects of Frontal Lobe Function Russell M. Bauer, Ph.D. February 27, 2006

2
Important Concepts Phylogenetically newest area of cortex Exquisite connectivity based on feedback loops Inhibitory/excitatory control Farthest removed from external environment (reflective, not reflexive) Highly preprocessed, convergent projections (emergent concepts) Only neocortical representation of the limbic system Motivational/emotional interaction (goal-direction)
 Highly preprocessed, convergent projections (emergent concepts) Only neocortical representation of the limbic system Motivational/emotional interaction (goal-direction)")
3
Symptoms of Frontal Lobe Damage Elementary Neurological Defects Skilled Movement Disorders Language/Speech Disorders Memory Disorders Executive Deficits Neuropsychiatric Disturbances

4
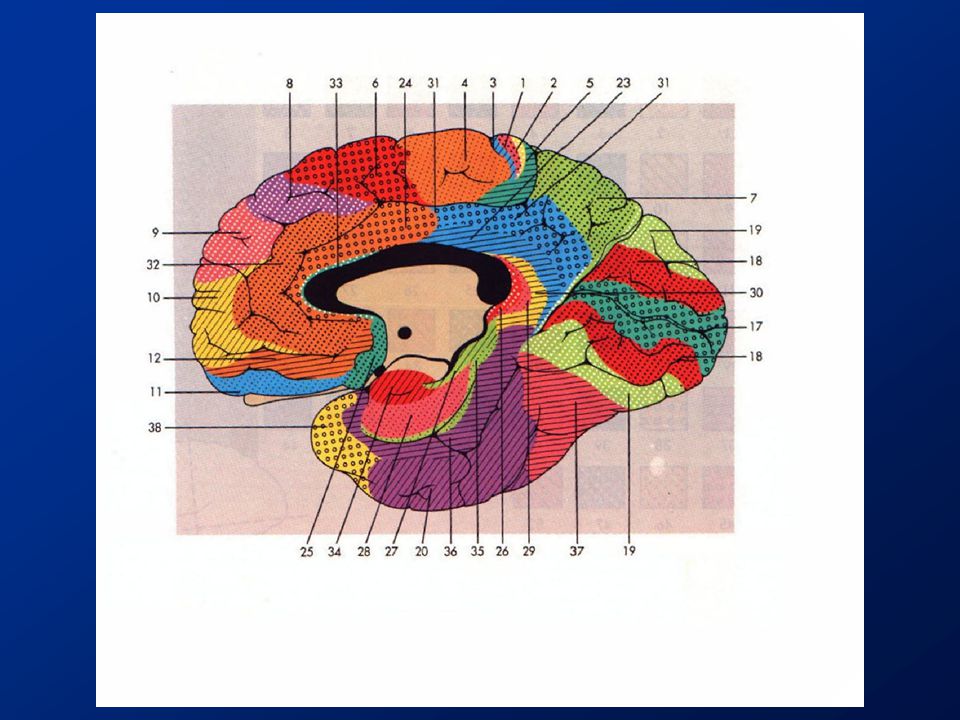
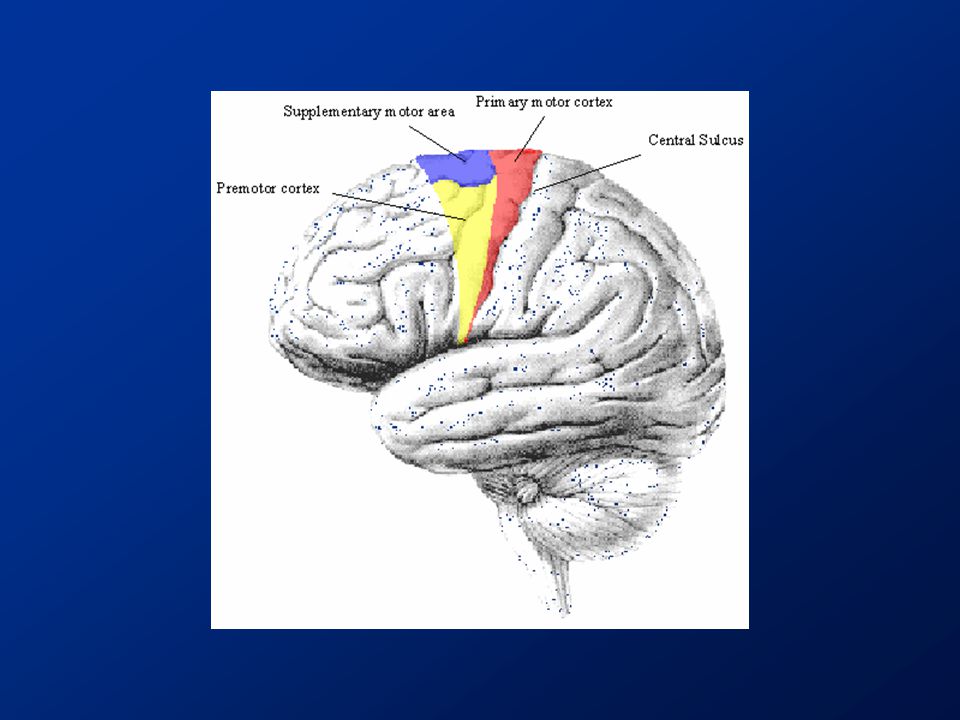
Frontal Lobe Cortex Functional subdivisions: –Lateral (4, 6, 8-10, 43- 47) –Medial (6, 8-12, 24, 25, 32, 22) –Inferior (11-15, 25, 47) Another division: –Motor (4) –Premotor (6, 8, 43, 44, 45) –Prefrontal (9-15, 46, 47)
 –Medial (6, 8-12, 24, 25, 32, 22) –Inferior (11-15, 25, 47) Another division: –Motor (4) –Premotor (6, 8, 43, 44, 45) –Prefrontal (9-15, 46, 47)")
5
Neuropsychological Manifestations of Frontal Lobe Lesions III Lateral Prefrontal Region (8,9,46) Lesions in this region produce impairment in a variety of “executive” skills that cut across domains. Some degree of material-specificity is present, but relatively weak. A) Fluency: impaired verbal fluency (left) or design fluency (right) B) Memory impairments: defective recency judgment, metamemory defects, difficulties in memory monitoring C) Impaired abstract concept formation and hypothesis testing D) Defective planning, motor sequencing E) Defective cognitive judgement and estimation Tranel, 1992
 Fluency: impaired verbal fluency (left) or design fluency (right) B) Memory impairments: defective recency judgment, metamemory defects, difficulties in memory monitoring C) Impaired abstract concept formation and hypothesis testing D) Defective planning, motor sequencing E) Defective cognitive judgement and estimation Tranel,")
6
Neuropsychological Manifestations of Frontal Lesions I Frontal Operculum (44,45,47) A) Left: Broca’s aphasia B) Right: ‘expressive’ aprosodia Superior Mesial (mesial 6, 24) A) Left: akinetic mutism B) Right: akinetic mutism Bilateral lesions of mesial SMA (6) and anterior cingulate (24) produce more severe form of akinetic mutism Tranel, 1992
 A) Left: Broca’s aphasia B) Right: ‘expressive’ aprosodia Superior Mesial (mesial 6, 24) A) Left: akinetic mutism B) Right: akinetic mutism Bilateral lesions of mesial SMA (6) and anterior cingulate (24) produce more severe form of akinetic mutism Tranel, 1992")
7
Neuropsychological Manifestations of Frontal Lobe Lesions II Inferior Mesial Region A) Orbital Region (10, 11) Lesions in this region produce disinhibition, altered social conduct, “acquired sociopathy”, and other disturbances due to impairment in fronto-limbic relationships B) Basal Forebrain (posterior extension of inferior mesial region, including diagonal band of Broca, nucleus accumbens, septal nuclei, substantia innominata) Lesions here produce prominent anterograde amnesia with confabulation (material specificity present, but relatively weak) Tranel, 1992
 Orbital Region (10, 11) Lesions in this region produce disinhibition, altered social conduct, acquired sociopathy , and other disturbances due to impairment in fronto-limbic relationships B) Basal Forebrain (posterior extension of inferior mesial region, including diagonal band of Broca, nucleus accumbens, septal nuclei, substantia innominata) Lesions here produce prominent anterograde amnesia with confabulation (material specificity present, but relatively weak) Tranel, 1992")
11
General Organization of Frontal cortical- striatal-pallidal-thalamic-cortical loops

12
Dorsolateral Loop Critical for executive function Damage produces –Inflexibility –Planning –Problem-solving –Goal-directed behavior

13
Orbitofrontal Loop Involved in social and emotional functioning Damage produces: –Disinhibition –Hyperactivity –Emotional lability –Aggressiveness –Reduce self- awareness

14
Medial Frontal Loop Important in behavioral activation Damage results in –Akinetic mutism –Abulia –Impairments in spontaneous initiation of behavior

15
Neuropsychological Domains motor activity attention personality/emotion perceptual organization spatial/visual function memory cognitive skills executive skills

16
Elementary Neurological Deficits in Frontal Syndromes Contralesional hemiparesis Re-emergence of primitive reflexes Gaze abnormalities (spontaneous eye- movements, conjugate gaze)
")
17
Frontal Lesions and “Personality” (overall ‘emotional tone’) orbital syndrome –emotional lability –disinhibition –exaggeration of pre-existing personality traits medial/lateral syndrome –abulia/apathy –depression-like presentation –defects in self-initiation
 orbital syndrome –emotional lability –disinhibition –exaggeration of pre-existing personality traits medial/lateral syndrome –abulia/apathy –depression-like presentation –defects in self-initiation")
18
Phineas Gage (Harlow, 1868) “Prior to his accident, he was a religious, family-loving, honest and hard-working man who was described after his frontal injury as ‘fitful, irreverent, indulging at times in the grossest profanity…impatient of restraint or advice when it conflicts with his desires…obstinate, devising many plans of operation, which are no sooner arranged than they are abandoned in turn for others appearing more feasible’” (Benson, 1994)
 Prior to his accident, he was a religious, family-loving, honest and hard-working man who was described after his frontal injury as ‘fitful, irreverent, indulging at times in the grossest profanity…impatient of restraint or advice when it conflicts with his desires…obstinate, devising many plans of operation, which are no sooner arranged than they are abandoned in turn for others appearing more feasible’ (Benson, 1994)")
19
Frontal Lobe Symptoms Relevant to Emotion and Personality NOT independent of cognitive impairments Poor self-monitoring and self-reflection Defective arousal and orienting responses Affective changes –Witzelsucht and Moria (Oppenheim) –Depression with lack of concern “Acquired sociopathy” (Damasio) – unconcern for punishment
 –Depression with lack of concern Acquired sociopathy (Damasio) – unconcern for punishment")
21
Somatic Marker Hypothesis Biasing signals from body are integrated in the decision- making and emotional parts of the brain (VMPFC) and used to regulate decision-making under uncertainty Markers signal value and bolster attention and working memory Case EVR (tumor of VMPFC) – became unable to make decisions despite good NP performance; unsuitable choices for business partners, friends, etc. EVR impaired in psychophysiological responses to positive and threatening information Much of the data for SM hypothesis is based on the Iowa Gambling Task

25
Activation during anticipation (risky decisions – safe decisions) superimposed on T1 image for all subjects. Overall score on IGT was correlated with the amount of activity in medial frontal lobe during risky decisions. Fukui, et al. (2005). Neuroimage, 24, 253-259.
. Neuroimage, 24,")
28
Motor Deficits in Frontal Syndromes Two dominant behavioral syndromes: –hyperactivity –apathy/abulia Contralesional hemiparesis; in less severe form, contralateral reduction in speed or dexterity Ideomotor apraxia – impaired skilled movement in nonhemiparetic hand/extremity Motor impersistence- failure to maintain motor activity; test with eye closure, tongue protrusion Impaired verbal control over conscious motor acts - inability to invoke verbal rules(e.g., Go-No Go); inability to use verbal intentions to guide behavior (e.g., don’t drink the water)
; inability to use verbal intentions to guide behavior (e.g., don’t drink the water)")
29
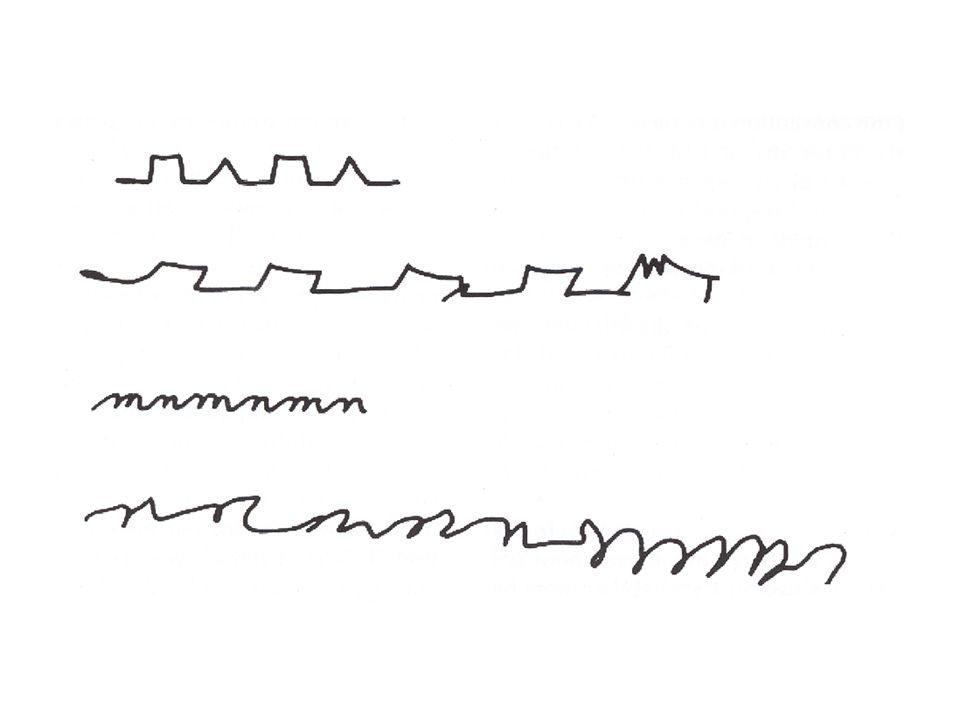
Motor Deficits (cont’d) Defects in motor programming and sequencing - recursive writing sequences Impaired guidance and error correction Poverty of movement without weakness, hemiparesis, or abnormality in tone (intentional disorder)
 Defects in motor programming and sequencing - recursive writing sequences Impaired guidance and error correction Poverty of movement without weakness, hemiparesis, or abnormality in tone (intentional disorder)")
33
Tests of Frontal Motor Function hand-grip strength finger tapping speed static steadiness manual dexterity maze coordination complex tests of praxis

34
Frontal Lobes and Attention Inhibition/gating of sensory transmission through thalamic interaction

38
Attentional Defects in Frontal Disease attention-focusing attention-maintenance attention-selectivity –interference susceptibility –Poor goal-dependent filtering of irrelevant stimuli attention-shifting

39
Tests of Attentional Function span tests (DS, Sentence Rep) cancellation tasks (simple and conditional) sustained attention –PASAT –Trail Making Test –Digit Symbol qualitative features from other tests
 cancellation tasks (simple and conditional) sustained attention –PASAT –Trail Making Test –Digit Symbol qualitative features from other tests")
40
Frontal Lobes and Memory Classic studies of delayed response (DR) and delayed alternation (DA) Dorsolateral and frontal polar lesions produce greatest deficits DR = dorsal? DA = ventral?

41
Human Frontal Memory Defects Short-term memory –deficits in working memory Learning –susceptibility to proactive interference –shallow semantic encoding –impairment in “voluntary memorizing” –impaired “directed forgetting” Long-term memory –recall deficits relative to recognition –impaired memory for temporal order –impaired recency judgments –Contamination of “true memory” with “inert stereotypes”

45
Table Grill Ounce Crayon Fable Pencil Grill Fable

46
Human Frontal Memory Deficits (cont’d) Impairments in “metamemory” –failure of emergent awareness –poor self-monitoring and self-correction –poor knowledge of content of memory system (e.g., poor connection between search and FOK) –deficits in source memory –poor strategy use –impaired memory for self-generated responses
 Impairments in metamemory –failure of emergent awareness –poor self-monitoring and self-correction –poor knowledge of content of memory system (e.g., poor connection between search and FOK) –deficits in source memory –poor strategy use –impaired memory for self-generated responses")
48
Frontal “Executive” Skills a working definition of “executive” skill relevant skill domains –planning –goal establishment –anticipation –cognitive estimation –hypothesis testing (TOTE)
")
49
An MBA’s Model of the Brain

50
Cognitive Deficits in Frontal Syndromes impaired abstract thinking –tendency to interpret abstract concepts concretely (e.g., proverbs, similarities) –tendency to be “pulled” to more immediately available sensory information impaired verbal reasoning impairments in memory –organizational role –informational - specific memory capacities of frontal lobe (e.g., working memory; retrieval)
 –tendency to be pulled to more immediately available sensory information impaired verbal reasoning impairments in memory –organizational role –informational - specific memory capacities of frontal lobe (e.g., working memory; retrieval)")
54
Design Fluency Examiner Patient

56
Utilization Behavior

57
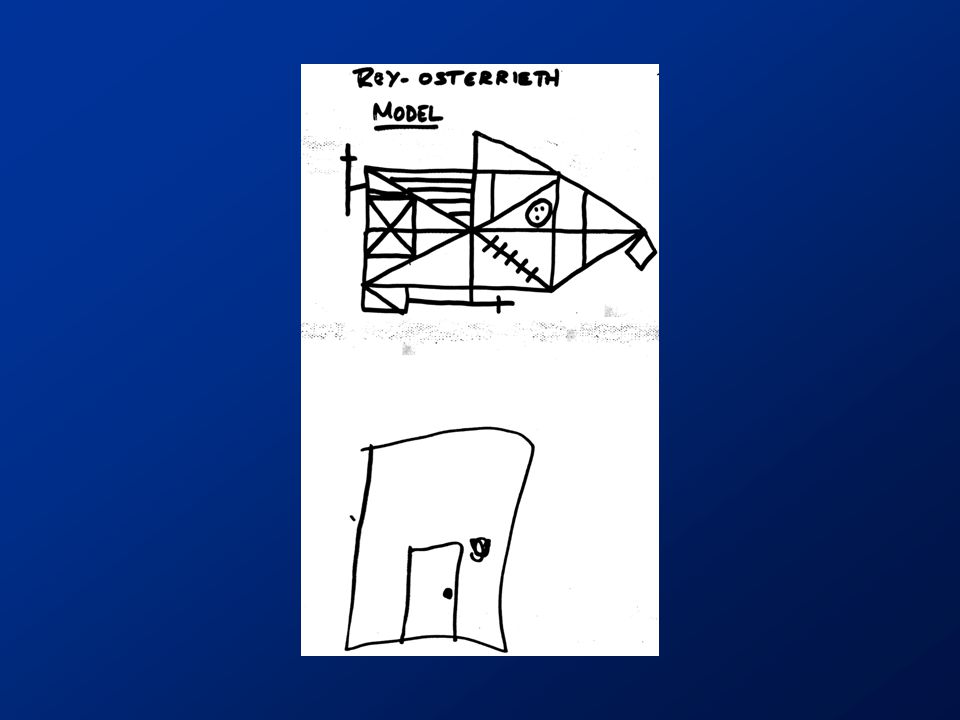
Tests Tapping ‘Frontal’ Cognitive Defects Wisconsin Card Sorting Test Halstead Category Test Shipley-Hartford Analogic Reasoning Trail-Making A and B Porteus Mazes (planning) Constructional Tasks (ROCF, BD) practically any other test calling for response production and organization!
 Constructional Tasks (ROCF, BD) practically any other test calling for response production and organization!")
61
Theories of Frontal Lobe Function Pribram (1960): Feedback Teuber (1964): Corollary discharge Nauta (1971): interoceptive (limbic) and exteroceptive (sensory, association) connectivity Fuster (1980): temporal organization Shallice (1978): information processing Luria (1973): hierarchical model
: Feedback Teuber (1964): Corollary discharge Nauta (1971): interoceptive (limbic) and exteroceptive (sensory, association) connectivity Fuster (1980): temporal organization Shallice (1978): information processing Luria (1973): hierarchical model")
Similar presentations






























 Dived down the middle lengthwise into two halves called.>")


 space,time, motion, planning, decision making, emotional reactivity,>")







 Mental Activity-Attention and speed of information processing Filtering, focusing, shifting tracking Filtering, focusing,>")