Download presentation
Presentation is loading. Please wait.

2
Magnetic Resonance and Computed Tomography in Pediatric Urology
Atoosa Adibi MD. Isfahan University Of Medical scienses

3
Ultrasound (US) is the most widely used and
primary imaging modality for the urinary tract in children. magnetic resonance (MR) imaging as second step, particularly in pediatric patients. an advanced pediatric radiology unit : most routine uroradiologic examinations can be performed with US and MR imaging
 imaging as second step, particularly in pediatric patients. an advanced pediatric radiology unit : most routine uroradiologic examinations can be performed with US and MR imaging.")
4
exception is: following an US, additional diagnostic imaging for urolithiasis is needed in the case of severe polytrauma,including blunt abdominal trauma. computed tomography (CT)
")
5
MR IMAGING OF THE URINARY TRACT

6
Indications: congenital anomalies,mainly pelvicaliectasis and/or ureterectasis, renal and bladder tumors. Infections and vascular anomalies of the urinary tract

7
precontrast, postcontrast, and dynamic postcontrast studies.
The precontrast sequences are optimal for depicting the urine-filled pelvicalyceal system and ureter and provide exquisite morphologic detail. After administering intravenous (IV) contrast, performing dynamic sequences is a better choice for the kidneys, as it provides the information of a non dynamic contrast study in addition to functional information with depiction of the arterial, venous, nephrographic, and urographic phases. The postcontrast dynamic study can be conducted as MR angiography (MRA).
 contrast, performing dynamic sequences is a better choice for the kidneys, as it provides the information of a non dynamic contrast study in addition to functional information with depiction of the arterial, venous, nephrographic, and urographic phases. The postcontrast dynamic study can be conducted. as MR angiography (MRA).")
8
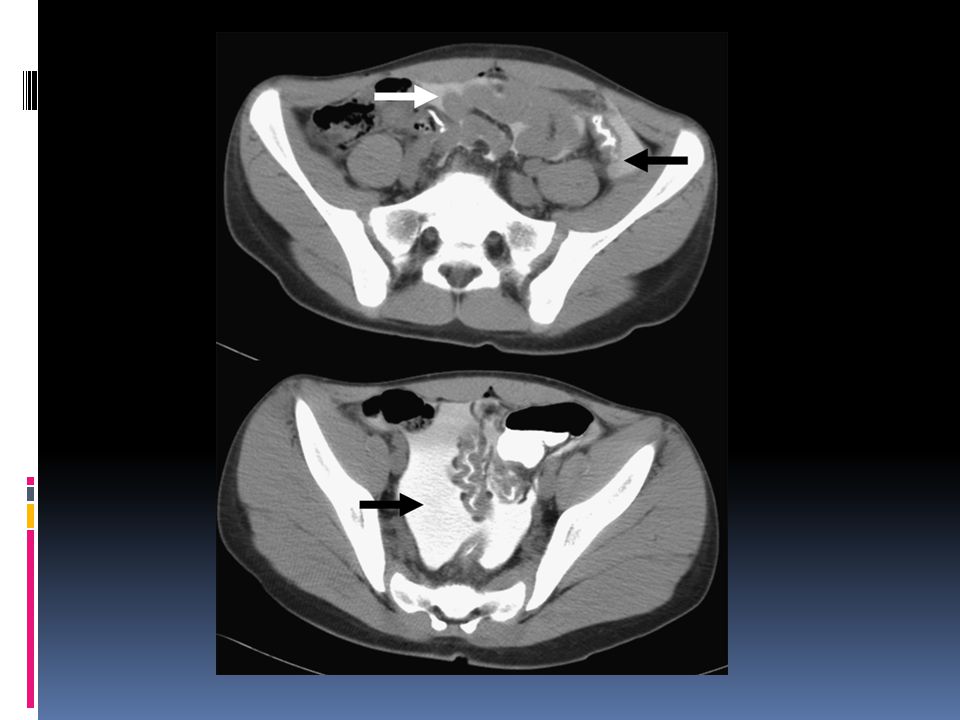
Precontrast MR urography demonstrating bilateral UVJO.

9
Procedure Preparation:Hydration with IV fluid administration starting a half hour before the scan A bladder catheter is placed.( A distended bladder may have a negative effect on the excretion of urine) The urine bag is placed below the level of the scanner table Furosemide (Lasix) is administered IV at a dose of 1 mg/kg (maximum 20 mg), 10 minutes before the procedure.
 The urine bag is placed below the level of the scanner table. Furosemide (Lasix) is administered IV at a dose of 1 mg/kg (maximum 20 mg), 10 minutes before the procedure.")
10
It is best to place the patient in the prone position if we are evaluating the contrast excretion into the pelvicaliceal system. Gadolinium-DTPA (Magnevist), has higher (1.208) specific gravity than urine (1.002– 1.030) and settles in the dependent position.
, has higher (1.208) specific gravity than urine (1.002– 1.030) and settles in the dependent position.")
11
a sagittal T2 sequence An axial T2 with fat saturation A 3D T2 with fat saturation The T1 fa tsaturated +post contrast

12
axial plane in T2 with fat saturation
The sagittal T1sequence with fat saturation

15
Procedural and scan modifications
1. Ectopic ureter: the precontrast series may suffice to depict the morphologic findings and the postcontrast part needs to be added only if functional evaluations of the kidneys are requested

16
2. Cyst versus diverticulum: Calyceal diverticulum fills with contrast in a retrograde manner later than the calyces or renal pelvis. The delay(sometimes needs to be 1 hour or longer)
.")
19
CT OF THE URINARY TRACT: URO-CT

20
the main attractions for using uro-CT in pediatrics are availability, fast speed, less frequent/no need for sedation, and lesser cost. CT may be used as a confirmatory secondary modality, as in the case of CT for urolithiasis.

21
try to find alternative modalities,completely avoiding potential radiation exposure.
uro-CT needs to be considered as a secondary option if US and/or MR imaging are inadequate, unavailable,or cannot be performed and the clinical suspicion warrants further imaging clarification.

23
It is important to note that in blunt abdominal
trauma in children, renal lesions are more frequent. than in adults because of a nonossified thoracic cage, thin abdominal wall, and paucity of perirenal fat. try not to overdo CT, even in the setting of pediatric trauma

24
Procedure preceded at least by US
A multiphase study has rarely any place in pediatric uro-CT

25
arterial phase: a bolus triggering , or a delay of 8 to 20 seconds
Nephrographic phase: delay of 70 to 100 seconds the excretory phase: delay can be 5 to 15 minutes. Additional CT angiography and/or urography are not routinely performed. For renal trauma, mostly a nephrographic phase acquisition will suffice.

26
splitting the contrast bolus and injecting at 2 different time points can produce both nephrographic and urographic phases simultaneously on one scan

27
Diagnostic Utility In trauma cases, a meticulously conducted abdominal US and Doppler study is adequate to exclude major renal injury in children. In the follow-up of traumatic renal findings, US is also the imaging modality of choice

28
uroCT and urolithiasis
Suspected stone of the urinary tract when an US with color Doppler does not depict a stone, but secondary signs are present, or an US is inconclusive/ negative, and high clinical suspicion remains

29
a well-hydrated patient is optimal.
The patient is placed in prone position to be able to differentiate an impacted stone at the ureterovesical junction from that of a mobile bladder calculus

32
Assessment: …… Diagnostic Utility: difference in usefulness between the 2 tests may not be clinically significant.

33
CT ANGIOGRAPHY Indications: Renovascular hypertension
traumatic renovascular injury other less common renovascular disorders

34
(neonate, 24 G; infant, 22/24 G; >1 year, 20/22 G).
For optimal power injection of the contrast, a suitable size of peripheral IV catheter is necessary (neonate, 24 G; infant, 22/24 G; >1 year, 20/22 G). The IV access is first tested with saline at the same flow rate planned for contrast injection.
. The IV access is first tested with saline at. the same flow rate planned for contrast injection.")
35
The scan extends from the supraceliac aorta to the upper external iliac arteries
Alternatively, a split-bolus technique may be used, injecting one third to one-half of the contrast volume beforehand and the other two- thirds to one-half for an arterial phase scan. This allows a combination of an arterial and a urographic phase in one single acquisition.

36
Assessment In renovascular hypertension, the focus is on morphologic changes of the renal arteries (stenoses,aneurysms, beadings) and secondary signs (poststenotic dilatation, collateral formation, focal parenchymal perfusion defects, asymmetric nephrogram, parenchymal scarring)
 and secondary signs (poststenotic dilatation, collateral formation, focal parenchymal perfusion defects, asymmetric nephrogram, parenchymal scarring)")
37
a 3-year-old patient with hypertension and neurofibromatosis type I demonstrates a
short-segment high-grade stenosis

38
CT CYSTOGRAPHY Active contrast filling of the urinary bladder, to detect extraluminal contrast, which is an indicator of rupture. Direct CT cystography entails retrograde filling of the bladder and indirect CT cystography passive antegrade filling of the bladder after IV contrast administration.

40
Indications Bladder trauma with or without known pelvic
fracture and hematuria workup for suspected delayed spontaneous rupture of augmented bladder

41
Procedure For direct CT cystography before bladder catheterization:
exclude urethral injury An age appropriate Foley catheter is placed; the balloon is not inflated. A precontrast scan is performed from the diaphragm to the ischial tuberosity. A drip infusion is prepared with diluted (10%) water-soluble contrast (eg, 50 mL in 450 mL 0.9% NaCl solution). The bladder is filled until the patient starts to void or the maximal bladder capacity ([age 1, 2] 30, mL) is reached. Wait for about 5 minutes and rescan the abdomen and pelvis. If no contrast extravasation is visualized, it may be necessary to perform further delayed scan of just the pelvis
 water-soluble. contrast (eg, 50 mL in 450 mL 0.9% NaCl solution). The bladder is filled until the patient starts. to void or the maximal bladder capacity ([age 1, 2] 30, mL) is reached. Wait for about 5 minutes and rescan the abdomen and. pelvis. If no contrast extravasation is visualized, it. may be necessary to perform further delayed. scan of just the pelvis.")
42
Indirect CT cystography is performed after IV contrast administration and antegrade filling, particularly in the setting of polytrauma. This includes occlusion of the Foley catheter, if present, when the patient arrives in the CT suite and a delay of 5 to 10 minutes after the IV contrast administration before rescanning the abdomen and pelvis. However,the indirect cystography is much less reliable in the diagnosis of bladder rupture.

44
KEY POINTS: Ultrasound is the primary imaging modality for the pediatric urinary tract. Magnetic resonance (MR) imaging needs to be the second imaging option after ultrasound in children. Functional MR urography (fMRU) provides comprehensive morphologic and functional information. Computed tomography (CT) is the imaging choice in children only in the following circumstances: (1) inadequate ultrasound for urolithiasis, and (2) blunt abdominal trauma in the setting of polytrauma. The choice of CT over MR for uroradiologic imaging is mainly for ancillary reasons: availability, fast speed, no sedation, and low cost. In children, CT angiography (CTA) of the urinary tract is primarily performed for evaluation of therenal arteries for suspected stenosis. Direct CT cystography may be necessary for evaluation of bladder rupture.
 imaging needs to be the second imaging option after ultrasound in children. Functional MR urography (fMRU) provides comprehensive morphologic and functional information. Computed tomography (CT) is the imaging choice in children only in the following circumstances: (1) inadequate ultrasound for urolithiasis, and (2) blunt abdominal trauma in the setting of polytrauma. The choice of CT over MR for uroradiologic imaging is mainly for ancillary reasons: availability, fast speed, no sedation, and low cost. In children, CT angiography (CTA) of the urinary tract is primarily performed for evaluation of therenal arteries for suspected stenosis. Direct CT cystography may be necessary for evaluation of bladder rupture.")
46
Diagnostic examination of the child with urolithiasis or nephrocalcinosis

47
Stones of all composition, with the exception of drugs (e. g
Stones of all composition, with the exception of drugs (e.g. indinavir) and matrix (protein), have distinguishing characteristics of echogenicity and shadowing on ultrasonography. Ultrasonography has the additional advantages of wide availability, avoidance of ionizing radiation, ready detection of hydronephrosis, and ability to define some aspects of the anatomy of the urinary tract.
 and matrix (protein), have distinguishing characteristics of echogenicity and shadowing on ultrasonography. Ultrasonography has the additional advantages of wide availability, avoidance of ionizing radiation, ready detection of hydronephrosis, and ability to define some aspects of the anatomy of the urinary tract.")
48
stones as small as only 1.5–2 mm in diameter can be visualized on ultrasonography (US), the success of this imaging method clearly depends on inter-observer and intra- observer variability and skills.
, the success of this imaging method clearly depends on inter-observer and intra- observer variability and skills.")
49
For the detecting and monitoring of nephrocalcinosis,high-resolution ultrasonography is the optimal imaging method .Nephrocalcinosis is classified according to the anatomic area involved.

50
Some pitfalls in the renal ultrasonography of neonates, and especially preterm infants, have to be noted: Tamm–Horsfall protein (THP) deposits within the renal calyces may look like nephrocalcinosis . THP deposition,however, disappears within 1–2 weeks, and follow-up will show completely normal kidneys.
 deposits within the renal calyces may look like nephrocalcinosis . THP deposition,however, disappears within 1–2 weeks, and follow-up will show completely normal kidneys.")
51
the echogenicity of the renal cortex in neonates is physiologically increased, hence detection of cortical nephrocalcinosis can be difficult and may become evident only some weeks later when a rim of cortical calcification becomes visible.

52
Normal, still hyperechoic kidney of a preterm infant

53
Tamm–Horsfall kidney

54
medullary nephrocalcinosis (NC) grade 1
 grade 1")
55
medullary NC grade II (mild increase of echogenicity at whole pyramid)
")
56
medullary NC grade III (more severe hyperechogenicity of entire pyramid);
;")
57
Diffuse corticomedullary NC

59
vesicoureteral reflux in children
Imaging studies are the basis of diagnosis and management of VUR. The standard imaging tests include renal and bladder ultrasonography and voiding cystourethrography (VCUG).
.")
60
Indications for imaging studies are as follows:
Imaging after the first UTI is indicated in all children younger than 5 years, children of any age with febrile UTI, and boys of any age with UTI Children with prenatally identified hydronephrosis should be evaluated postnatally; however, ultrasonography performed during the first 3 days of life may have a high rate of false- negative results because of relative dehydration during the neonatal period

61
Although the traditional approach in children with UTI has been evaluation for VUR with VCUG or radionuclide cystography (RNC), some authorities now advocate that children with a history of febrile UTI undergo a dimercaptosuccinic acid (DMSA) renal scan, to assess for evidence of kidney involvement, kidney scarring, or both; if DMSA scan findings are positive, VCUG is recommended.
, some authorities now advocate that children with a history of febrile UTI undergo a dimercaptosuccinic acid (DMSA) renal scan, to assess for evidence of kidney involvement, kidney scarring, or both; if DMSA scan findings are positive, VCUG is recommended.")
62
One approach is to perform RNC as the initial screening test in girls and then to perform standard VCUG when VUR is observed. Other clinicians use VCUG for the initial diagnosis and use RNC for follow-up studies.

63
VCUG is the criterion standard in diagnosis of VUR, providing precise anatomic detail and allows grading of the reflux. The International Classification System for VUR is as follows[3] : Grade I - Reflux into nondilated ureter Grade II - Reflux into renal pelvis and calyces without dilation Grade III - Reflux with mild to moderate dilation and minimal blunting of fornices Grade IV - Reflux with moderate ureteral tortuosity and dilation of pelvis and calyces Grade V - Reflux with gross dilation of ureter, pelvis, and calyces, loss of papillary impressions, and ureteral tortuosity
![VCUG is the criterion standard in diagnosis of VUR, providing precise anatomic detail and allows grading of the reflux. The International Classification System for VUR is as follows[3] :](http://slideplayer.com/slide/4175314/13/images/63/VCUG+is+the+criterion+standard+in+diagnosis+of+VUR%2C+providing+precise+anatomic+detail+and+allows+grading+of+the+reflux.+The+International+Classification+System+for+VUR+is+as+follows%5B3%5D+%3A.jpg "Grade I - Reflux into nondilated ureter. Grade II - Reflux into renal pelvis and calyces without dilation. Grade III - Reflux with mild to moderate dilation and minimal blunting of fornices. Grade IV - Reflux with moderate ureteral tortuosity and dilation of pelvis and calyces. Grade V - Reflux with gross dilation of ureter, pelvis, and calyces, loss of papillary impressions, and ureteral tortuosity.")
64
In general, VCUG should be performed after the child has fully recovered from the UTI. However, some children demonstrate reflux only during an episode of cystitis.

65
Radionuclide cystography
Instillation of technetium-99m pertechnetate into the bladder and observation with a gamma camera is a highly sensitive test for VUR Advantages include substantially lower radiation doses than with VCUG and the potential for increased sensitivity because of the ability to conduct prolonged periods of observation Disadvantages primarily consist of the poor anatomic detail, especially of the male urethra Grade I reflux is poorly detected by this study, because the distal ureters are commonly obscured by the bladder Grading by nuclear cystography is limited to mild, moderate, and severe grades.

67
Pediatric Ureteropelvic Junction Obstruction Workup

68
Ultrasonography After the prenatal presumptive diagnosis UPJ obstruction or other conditions causing hydronephrosis is made, the neonate should undergo ultrasonographic evaluation, but the timing is controversial. Transient neonatal dehydration occurs hours after birth, so follow-up ultrasonography of mild-to-moderate cases of hydronephrosis should be performed after this period. In severe cases, such as very large renal pelvis, bilateral hydronephrosis, solitary kidney, or oligohydramnios, immediate evaluation within 48 hours must be performed; severe hydronephrosis in spite of the oliguric status of the child can suggest the need

69
Postnatal evaluation consists of a urinary tract study to determine whether the calyceal pelvic dilation with or without renal cortical thinning is present. The most widely used grading system of the severity of hydronephrosis on ultrasonography after birth is SFU system, rather than the anteroposterior diameter of the renal pelvis.

70
The SFU grading system for hydronephrosis is as follows[19] :
Grade 0 - No hydronephrosis, intact central renal complex seen on ultrasonography Grade 1 - Only renal pelvis visualized, dilated pelvis on ultrasonography, no caliectasis Grade 2 - Moderately dilated renal pelvis and a few calyces Grade 3 - Hydronephrosis with nearly all calyces seen, large renal pelvis without parenchymal thinning Grade 4 - Severe dilatation of renal pelvis and calyces with accompanying parenchymal atrophy or thinning
![The SFU grading system for hydronephrosis is as follows[19] :](http://slideplayer.com/slide/4175314/13/images/70/The+SFU+grading+system+for+hydronephrosis+is+as+follows%5B19%5D+%3A.jpg "Grade 0 - No hydronephrosis, intact central renal complex seen on ultrasonography. Grade 1 - Only renal pelvis visualized, dilated pelvis on ultrasonography, no caliectasis. Grade 2 - Moderately dilated renal pelvis and a few calyces. Grade 3 - Hydronephrosis with nearly all calyces seen, large renal pelvis without parenchymal thinning. Grade 4 - Severe dilatation of renal pelvis and calyces with accompanying parenchymal atrophy or thinning.")
71
Voiding cystourethrogram (VCUG)
Vesicoureteral reflux (VUR) has been found in as many as 40% of affected children. The degree of reflux is often low grade, not contributing to upper urinary tract obstruction, and it is likely to spontaneously resolve. However, UPJ obstruction may also be seen with severe VUR when the tortuous dilated ureter develops a kink in the UPJ area, which is relatively fixed to surrounding structures, and may cause secondary obstruction.
 has been found in as many as 40% of affected children. The degree of reflux is often low grade, not contributing to upper urinary tract obstruction, and it is likely to spontaneously resolve. However, UPJ obstruction may also be seen with severe VUR when the tortuous dilated ureter develops a kink in the UPJ area, which is relatively fixed to surrounding structures, and may cause secondary obstruction.")
72
Diuretic renography Diuretic renography is the most widely used noninvasive technique to determine the severity and functional significance of UPJ obstruction. Various protocols and techniques have been developed, resulting in significant variability in the interpretive criteria and results.

73
Doppler ultrasonography [
The development of Doppler ultrasonography has become another useful diagnostic modality in the assessment of kidneys with ureteropelvic junction (UPJ) obstructions. With duplex Doppler ultrasonography, intrarenal vasculature can be assessed to determine the resistive index. Normal kidneys reliably demonstrate resistive indices less than 0.7, and obstructed kidneys show higher values. Administration of diuretics can aggravate the preexisting obstruction, thereby aiding the diagnosis by Doppler ultrasonography. It is especially reliable in the preoperative diagnosis of aberrant-accessory blood vessels associated with UPJ obstruction.
 obstructions. With duplex Doppler ultrasonography, intrarenal vasculature can be assessed to determine the resistive index. Normal kidneys reliably demonstrate resistive indices less than 0.7, and obstructed kidneys show higher values. Administration of diuretics can aggravate the preexisting obstruction, thereby aiding the diagnosis by Doppler ultrasonography. It is especially reliable in the preoperative diagnosis of aberrant-accessory blood vessels associated with UPJ obstruction.")
74
Intravenous pyelography (IVP)
IVP has been used to evaluate UPJ obstruction, but IVP may not provide adequate information to determine the true obstruction, and it is especially difficult to interpret in children. IVP provides information about the obstruction and contralateral side and especially facilitates operative planning; however, infant urograms are compromised by the immature renal function, which impedes adequate visualization of the collecting system. Bowel gas and underlying bony structures also make interpretation of the urogram difficult.

Similar presentations















>")







>")






 are variable, occur in 1 of 500 newborns; predisposing to development of hypertension,>")