Download presentation
Presentation is loading. Please wait.

1
Congenital renal anomalies
CONGENITAL RENAL DISEASE IMAGING Congenital renal anomalies F.Hallaji MD radiologist f.

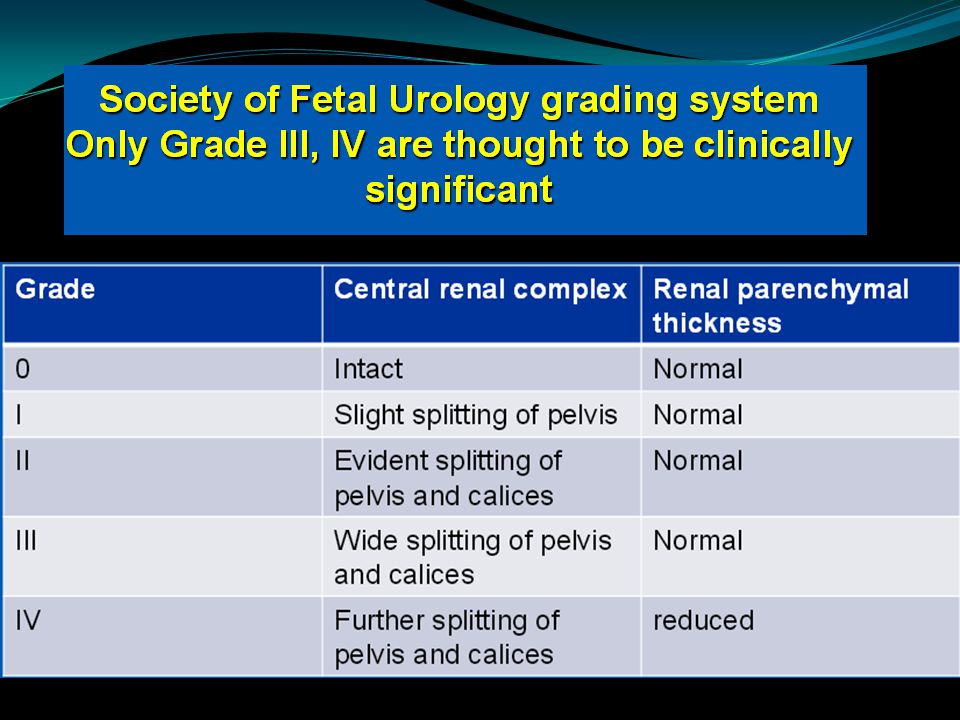
2
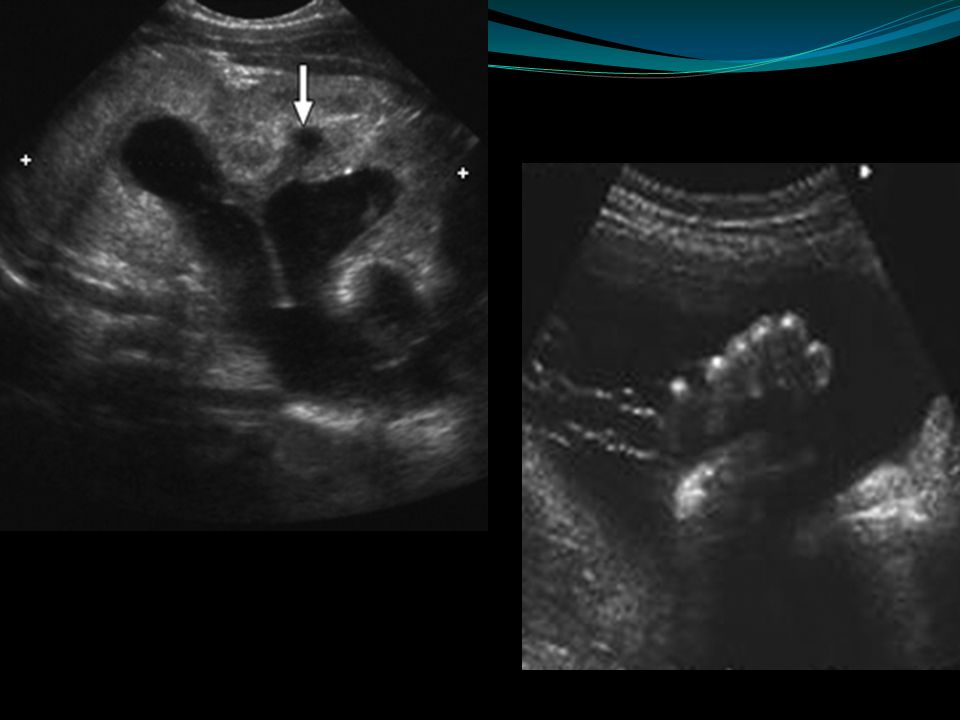
HYDRONEPHROSIS

8
Pregnancy in fetuses with unilateral or bilateral ANH should proceed to term, except if complicated by severe oligohydramnios or major structural anomalies. Early delivery is not indicated, and carries risks of prematurity and low birth weight.

10
fetuses with unilateral hydronephrosis :
at least one follow-up ultrasound be performed in the third trimester . fetuses with bilateral hydronephrosis : frequent monitor The frequency of monitoring varies from 4 to 6 weeks, depending on gestation at which ANH was detected, its severity and presence of oligohydramnios.

11
Dilated thick wall urinary bladder POSTERIOR URETHREAL VALVE

12
POST NATAL FOLLOW UP

13
Detailed ultrasound examination:
1- renal size 2- defining cortex echogenicity ( hyper/iso /hypoechoid compared with liver and spleen ) 3- medulla ( hypo/ anechoic / hyper) 4- assessing the CMD ( present / absent / reversed ). 5- evaluating for cysts ( numbers, size , location ) 6- calcifications 7- assessing the pelvicaliceal system .
 3- medulla ( hypo/ anechoic / hyper) 4- assessing the CMD ( present / absent / reversed ). 5- evaluating for cysts ( numbers, size , location ) 6- calcifications. 7- assessing the pelvicaliceal system .")
14
Medullary nephrocalcinosis

15
q Question 1 : A baby with prenatal mild hydronephrosis in 2nd trimester which resolved in third trimester of pregnancy Post natal follow up ?

16
All newborns with a history of ANH, including those in whom it had resolved prenatally, should undergo postnatal evaluation . 1 week & 6 weeks sonography

17
Time of post natal sonography A baby with mild prenatal hydronephrosis
Question 2 Time of post natal sonography A baby with mild prenatal hydronephrosis A baby with moderate to severe hydronephrosis

18
We recommend that all newborns with history of ANH should have postnatal ultrasound examination within the first week of life( days).
.")
19
In neonates with suspected posterior urethral valves, oligohydramnios or severe bilateral hydronephrosis, ultrasonography should be performed within h of birth

20
Since there is a risk that a proportion of patients might be lost to follow-up, we propose that neonates with unilateral or mild to moderate bilateral hydronephrosis be screened by ultrasonography prior to hospital discharge.

21
A baby with prenatatl hydronephrosis . Normal post natal sonography
Question 3: A baby with prenatatl hydronephrosis . Normal post natal sonography We recommend that neonates with normal ultrasound examination in the first week of life should undergo a repeat study at 4-6 weeks

22
Since progression might occur in the first 2-years of life, and occasionally until 5-6 years, follow-up studies are scheduled at 3-6 months, and then 6-12 monthly until resolution.

23
Recommended VCUG : in patients with unilateral or bilateral hydronephrosis with renal pelvic APD > 10 mm, SFU grade 3-4 or ureteric dilatation . VCUG can be performed early, within h of life, in patients with suspected lower urinary tract obstruction . In other cases, the procedure should be done at 4-6 weeks of age

24
infants with moderate to severe unilateral or bilateral hydronephrosis (SFU grade 3-4, APD >10 mm) who do not show VUR should undergo diuretic renography We suggest that diuretic renography be performed after 6-8 weeks of age . The procedure may be repeated after 3-6 months in infants where ultrasound shows worsening of pelvicalyceal dilatation .

31
RENAL CYSTIC DISEASES

32
The liver and genital tract should be evaluated whenever possible .
After birth in cases of antenatal diagnosis an abdominal ultrasound survey is recommended . Clinical informatin and familial history are essential for the differential diagnosis . Whenever cystic kidneys are suspeced it is useful to perform a sonographic examination of the parents to check for unknown familial disease .

33
Two main sonographic features:
CYSTS HYPERECHOGENICITY Renal cysts can develop in fetal life but more classi cally develop after birth . They develop anywhere in the kideny and can occur in one or both kidneys . Renal hyperechogenicity can be visualized in the entire kideny , only the cortex or only the medulla .

34
Once renal cystic disease is suspected
The first step is to rule out dysplasia associated with obstructive uropathy : Obstructive dysplasia is the most common cause of hyperechoic cortex with or without cysts . It can be bilateral or unilateral. The affected kidneys are of variable size The cortex is usually hyperechoic , thinned and irregular and the CMD is absent . These findings are related to the inflammatory infiltration , disorganized renal architecture and dystrophic calcification .

35
2-day-old boy with normal kidney
1-day-old boy with obstructive dysplasia of left kidney.

36
MCKD Second diagnosis to consider Multiple cysts of variable size without connections between thme and wiho ro nor little renal parnechyma Unilateral ( bilateral involving the upper or lower poles of duplex kidney or affect an ectopic kidney .) Can be associated with genital malformation both in girls and boys .
 Can be associated with genital malformation both in girls and boys .")
37
Both obstructive dysplasia & MCDK should be differentiated from complex cysts which include cystic tumors , renal lymphangioma and segmental cystic dysplasia . 7-day-old girl with probable segmental dysplasia of left kidney.

38
fe Fetus at 28 weeks gestation . Coronal ltrasound scanof both kidneys shows striking hyperechognicity of cortex and no CMD .

39
Recurrence of glomerulocystic kidney disease
2 –year –old boy . Sagital ultrasound scan shows left fetal kidney is hyperechoic without CMD bit with cysts , some subcapsular .

40
Recurrence of glomerulocystic kidney diseae .
35 –year-old man , patient`s father , with glomerulocystic kidney disease . Ultrasound scan shows kidney is small and has thick and hyperechoid cortex.

41
Oligohydramnios is present
Fetus at 30 weeks` gestation with autosomal recessive ploycystic shows both kidneys are markedly enlarged ( 8 cm ) and hyperechoic with no CMD . Oligohydramnios is present
 and hyperechoic with no CMD . Oligohydramnios is present.")
42
Renal anomalies are isolated findins
Renal anomalies are isolated findins . In fetus the finding of bilateral verey large ( >4 SD ) ,diffusely hyperechoic kidneys without CMD with or without evidenct cysts most likely corresponds to ARPKD The kidneys are diffusely affected but the extent of disease can be vatieble and evolves . Oligohydramnios is the rule . Very large hyperechoic kidneys with hyperechoic medulla ( reversed CMD ) is another typical patern establishing ARPKD in a fetus .
 ,diffusely hyperechoic kidneys without CMD with or without evidenct cysts most likely corresponds to ARPKD. The kidneys are diffusely affected but the extent of disease can be vatieble and evolves . Oligohydramnios is the rule . Very large hyperechoic kidneys with hyperechoic medulla ( reversed CMD ) is another typical patern establishing ARPKD in a fetus .")
43
Heptic changes are not detected until complications occur later in childhood .
-

44
Fetus at 34 weeks gestation with AR PKD with reversed CMD .

45
Glomerular cysts correspnd to distention of the Bowman spaces .
The kidneys are diffusely hyperechoic and enlarged ( +2 SD ) without CMD but with multiple subcapsular cysts. Additional cysts are evident throught the cortex .
 without CMD but with multiple subcapsular cysts. Additional cysts are evident throught the cortex .")
46
1 day-old boy with autosomal dominant polycystic kidney disease
1 day-old boy with autosomal dominant polycystic kidney disease. Ultrasound scan in partial sagittal view shows glomerulocystic kidney measuring 6 cm. Parenchyma is hyperechoic without corticomedullary differentiation, and multiple tiny cysts, mainly subcapsular, are visible.

47
2-day-old boy with glomerulocystic kidneys
2-day-old boy with glomerulocystic kidneys. moderately enlarged hyperechoic right kidney with one very large and many tiny cysts. Cortico medullary differentiation is absent .

48
2-day-old boy with HNF1β (TCF2) mutation and glomerulocystic kidneys
2-day-old boy with HNF1β (TCF2) mutation and glomerulocystic kidneys. B, Close-up view of right kidney shows hyperechoic parenchyma with multiple subcapsular cysts and no corticomedullary differentiation
 mutation and glomerulocystic kidneys. B, Close-up view of right kidney shows hyperechoic parenchyma with multiple subcapsular cysts and no corticomedullary differentiation.")
49
6-year-old boy with mild renal failure, anemia, and nephronophthisis
6-year-old boy with mild renal failure, anemia, and nephronophthisis. Kidneys are of normal or small and hyperechoic without corticomedullary differentiation. Cysts are evident at corticomedullary junction.

Similar presentations





















 Incidence: 1:188 Approximately 50% of antenatal scans are normal postnatally Posterior urethral.>")






 are variable, occur in 1 of 500 newborns; predisposing to development of hypertension,>")

