Download presentation
Presentation is loading. Please wait.

1
Hydrocephalus and Neuro Shunting
Sales Training April 2001

2
Hydrocephalus: From the Greek
word hydro (water) & cephalo (head). A pathological condition where there is a disturbance in production, circulation and/or absorption of CSF, with subsequent accumulation of CSF in the fluid-filled compartments of the brain (ventricles).
 & cephalo (head). A pathological condition where there. is a disturbance in production, circulation and/or absorption of CSF, with subsequent accumulation of CSF. in the fluid-filled compartments of the. brain (ventricles).")
3
About CSF (Cerebrospinal Fluid)
Clear, colorless fluid Bathes, nourishes & protects brain and spinal cord. Average CSF production-20ml/hr adults and 8ml/hr children 400 to 500cc produced daily contains 15 to 45mg/100ml protein,some glucose, salts, urea and WBC’s

4
Ventricular System 2 Lateral Third Fourth Foramen of Monro
Fluid filled cavities deep in cerebrum w/ pressure of mmH2O Four ventricles 2 Lateral Third Fourth Connected by Foramen of Monro Aqueduct of Sylvius

6
Choroid Plexus Very vascular Found throughout but mostly in lateral
Responsible for ICP waveform/ follows arterial pulse

7
Brain Layers/CSF Absorption
A. - Arachnoid A.G. - Arachnoid Granulation B. - Bone C.A. - Cerebral Artery C.V. - Cerebral Vein D. - Dura Mater F.C. - Falx Cerebri P.M. - Pia Mater S. - Skin S.A.S. - Sub-Arachnoid Space S.D.S. - Sub-Dural Space S.S.S. - Superior Sagittal Sinus

8
CSF Flow-path CSF flows in a caudal direction through the lateral, third and fourth ventricles Exits through foramina of Luschka and Magendie into subarachnoid space around spinal cord and brain. Absorption occurs through the arachnoid granulations into the venous system.

9
Types of Hydrocephalus
Communicating Non-communicating or Obstructive Normal Pressure Hydrocephalus Congenital Acquired

10
CT Scan Showing severe hydrocephalus Normal CT Scan

11
Etiology of Hydrocephalus
Communicating Overproduction/underabsorption of CSF Choroid Plexus Papilloma-overproduces CSF SAH Infection Neoplasms affecting the meninges Trauma

12
Etiology of Hydrocephalus
Non-Communicating (Obstructive) Aqueductal Stenosis Arnold-Chiari Malformation (Cerebellar tonsils protrude into Foramen Magnum) Cysts Myelomeningocele IVH Tumors (particularly posterior fossa)
 Aqueductal Stenosis. Arnold-Chiari Malformation (Cerebellar tonsils protrude into Foramen Magnum) Cysts. Myelomeningocele. IVH. Tumors (particularly posterior fossa)")
13
Normal Pressure Hydrocephalus
Usually present in elderly Ventricular dilation despite normal CSF pressure Triad of symptoms 1) dementia 2) gait disturbances (usually earliest) 3) urinary incontinence
 dementia. 2) gait disturbances (usually earliest) 3) urinary incontinence.")
14
Signs & Symptoms Associated with Hydrocephalus
Infants Increased head size Bulging Fontanels Separation of Cranial Sutures Prominent Scalp Veins Persistent Vomiting Lethargy or irritability “Setting Sun” eyes Seizures Delayed Development

16
S/S Associated with Hydrocephalus, cont.
Toddlers Increased head size Persistent vomiting Headache Lethargy or irritability “Setting Sun” eyes Blurred Vision Seizures Delayed Development

17
Hydrocephalus “SETTING SUN” EYES

18
S/S Associated with Hydrocephalus, cont.
Older Children & Adults Persistent Vomiting Headache** Visual Problems Lethargy Behavior Changes Difficulty with schoolwork Seizures

19
Diagnosis Clinical Evaluation
Ultrasound (Intrauterine & through Fontanels. CT Scan MRI

20
Treatment Modalities Surgical Procedures
Remove obstruction (Blood Clots, Tumors) Endoscopic Third Ventriculostomy Septal Fenestrations (Endoscopic) Cyst Fenestrations (Endoscopic) Shunt Insertion
 Endoscopic Third Ventriculostomy. Septal Fenestrations (Endoscopic) Cyst Fenestrations (Endoscopic) Shunt Insertion.")
21
Interventions for Hydrocephalus
If untreated: *50-60% die of complications If treated: *40% normal intelligence *70% live beyond infancy

22
Questions???

23
Historical Treatment of Hydrocephalous
Hippocrates recognizes water accumulation in the brain. 1545-Thomas Phaire-1st non-surgical treatment--Herbal plasters, head wraps 18th Century--ventricular puncture--death from meningitis common 1800’s-Variety of materials used to “wick” CSF from ventricles to subarachnoid space (i.e., linen threads, glass wool, rubber tube) 1898-first lumboperitoneal shunt
 1898-first lumboperitoneal shunt.")
24
Historical Treatment of Hydrocephalous, con’t
1922-Dandy-third ventriculostomy through subfrontal approach 1923-Mixter-1st endoscopic 3rd Vent., choroid plexectomy (L’Espinasse, Hildebrande, Dandy, Putnam and Scarff) 1950’s-First effective CSF diversion with a one-way valve using biocompatible synthetic materials. John Holter-1st Silicone Valve Robert Pudenz-Silicone distal slit valve Peritoneum chosen as better absorptive site than the vascular system
 1950’s-First effective CSF diversion with a one-way valve. using biocompatible synthetic materials. John Holter-1st Silicone Valve. Robert Pudenz-Silicone distal slit valve. Peritoneum chosen as better absorptive site than the. vascular system.")
25
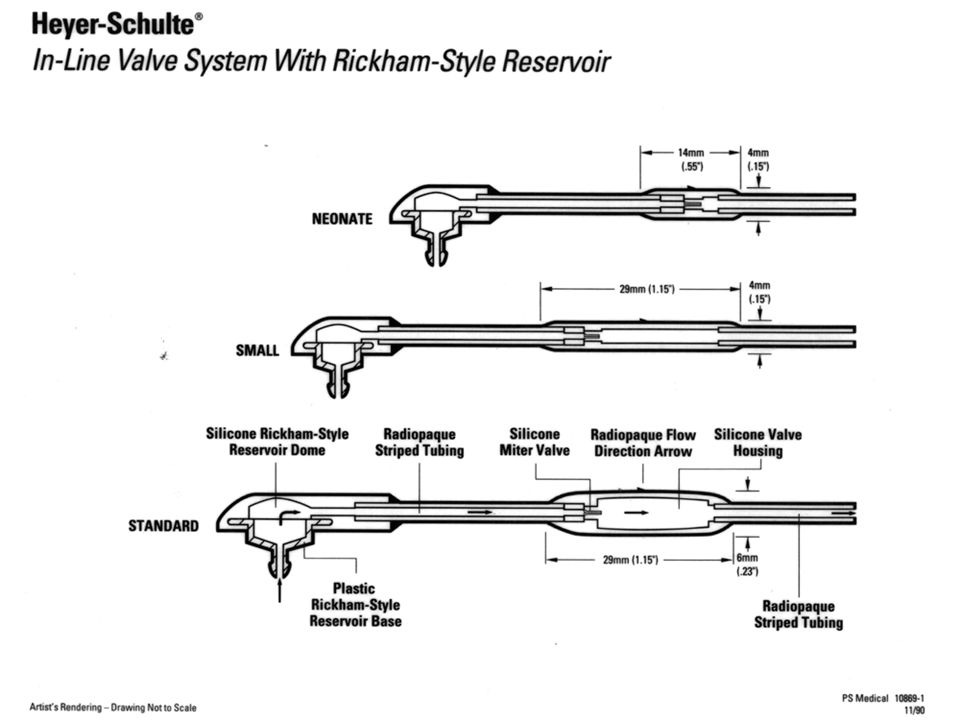
Heyer Schulte and Shunt Industry History
1953: Dr. Robert Pudenz and W.T. (Ted) Heyer team up on hydrocephalus research 1955: Pudenz ventriculo-atrial shunt is developed 1959: Rudy Schulte joins Heyer and Pudenz 1959: Pudenz flushing valve is developed 1960: Codman distributes Heyer-Schulte products 1960: Holter valve is created 1965: Cordis begins U.S. presence 1965: Extra-Corporeal buys Holter 1973: Codman dropped as Heyer-Schulte distributor
 Heyer team up on hydrocephalus research. 1955: Pudenz ventriculo-atrial shunt is developed. 1959: Rudy Schulte joins Heyer and Pudenz. 1959: Pudenz flushing valve is developed. 1960: Codman distributes Heyer-Schulte products. 1960: Holter valve is created. 1965: Cordis begins U.S. presence. 1965: Extra-Corporeal buys Holter. 1973: Codman dropped as Heyer-Schulte distributor.")
26
Heyer Schulte and Shunt Industry History
1974: American Hospital Supply buys Heyer-Schulte 1975: Codman introduces their own product line 1977: Anasco, PR manufacturing facility is built 1978: Codman buys Extra-Corporeal 1983: AHS folds Heyer-Schulte into V. Mueller 1984: Dr. Pudenz and Rudy Schulte found P-S Medical 1986: Baxter-Travenol acquires AHS

27
Heyer Schulte and Shunt Industry History
The 90’s NeuroCare Group acquires Heyer-Schulte Radionics introduces full shunt line Medtronic acquires P-S Medical Phoenix Biomedical enters the market Codman acquires Cordis Elekta acquires Cordis NMT acquires Cordis Integra acquires Heyer-Schulte

28
What is a Shunt? A shunt is a device that diverts CSF from the CNS (usually the lateral ventricle or the lumbar subarachnoid space) to an alternate body cavity (usually the peritoneum or the right atrium) where it is reabsorbed.
 to an alternate body cavity (usually the peritoneum or the right atrium) where it is reabsorbed.")
29
How Shunts Work Divert CSF from the CNS to another body cavity (R atrium, peritoneum) for absorption. Mechanical device that regulates flow out of the ventricle. One-way valve opens when the sum of the forces acting on it exceed some threshold. (the difference between the inlet or ventricular pressure and outlet or peritoneal pressure.

30
Shunt Systems Ventriculo-peritoneal Ventriculo-atrial
Lumbar-peritoneal

32
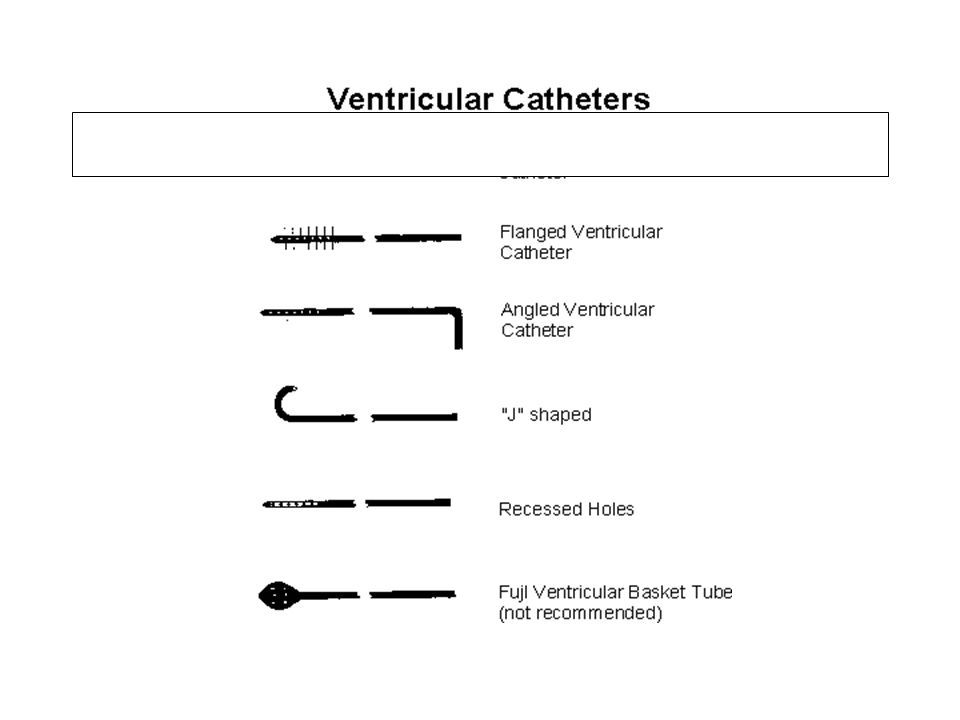
Shunt Components Primary Components Optional Components Accessories
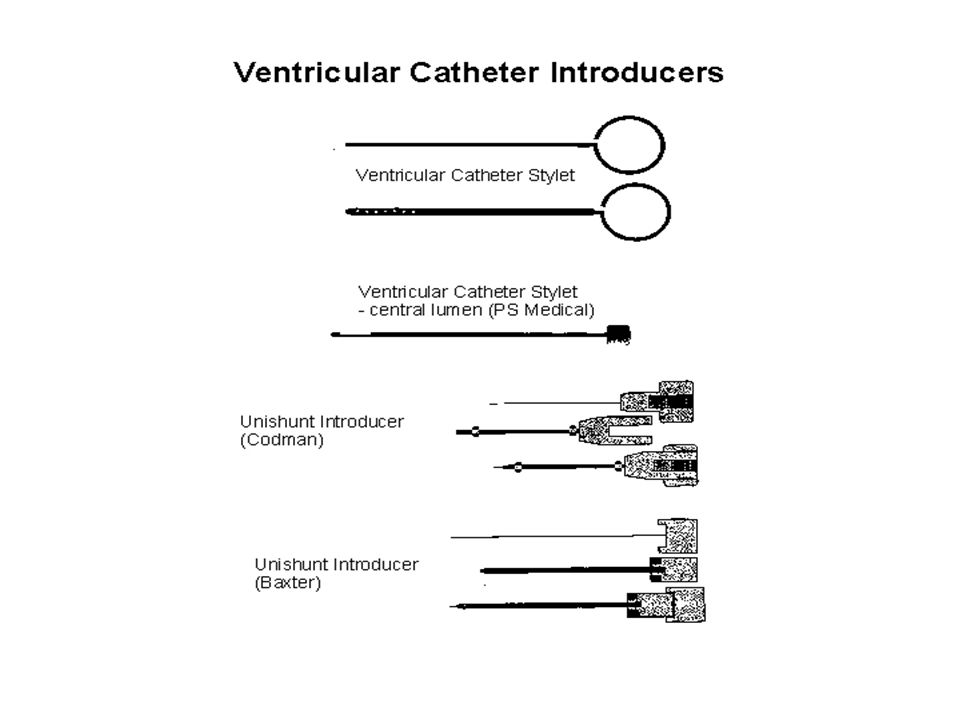
Proximal Catheter Valve (Proximal or Distal) Distal Catheter Optional Components Reservoir Siphon Limiting Mechanism (ASD, SCD, GCD) Accessories Connectors Guides Introducers/Stylets Catheter Passers
 Distal Catheter. Optional Components. Reservoir. Siphon Limiting Mechanism (ASD, SCD, GCD) Accessories. Connectors. Guides. Introducers/Stylets. Catheter Passers.")
35
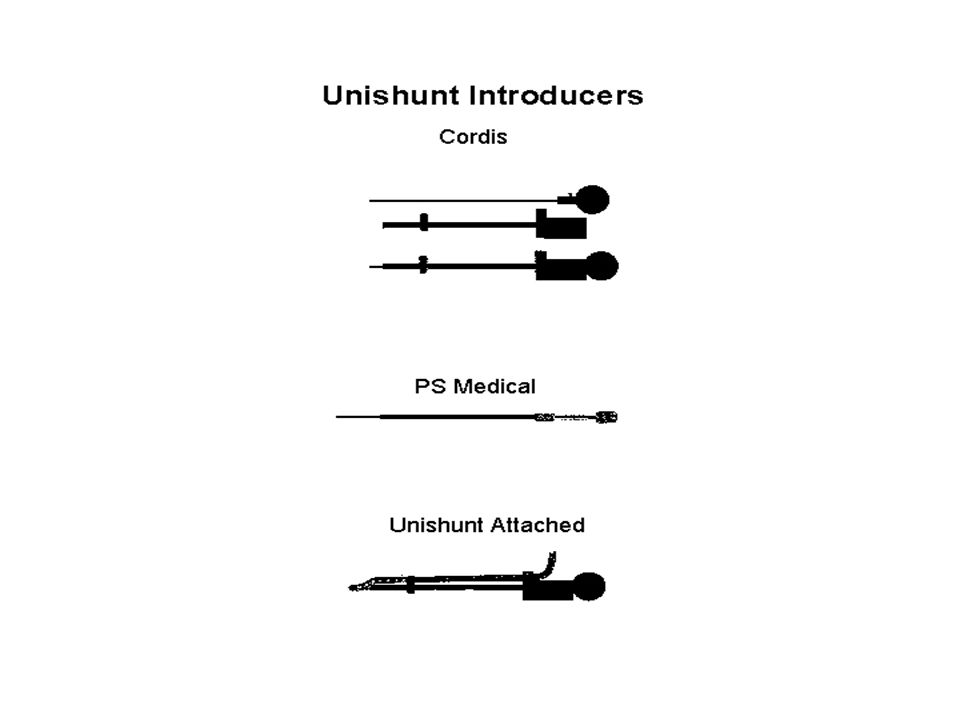
SHUNT ACCESSORIES Proximal catheter stylet (can use endoscope)
Stylets for unitized shunts Shunt passers Connectors and Right angle guides Shunt tap kits Manometers

41
Valve Mechanisms Differential Pressure Valves Flow regulating devices

42
Valve Mechanisms Differential Pressure Valves
Valves open when difference between the ventricular pressure and the peritoneal pressure exceeds some threshold. Pressure difference at which a valve opens is called the opening pressure. Pressure difference at which a valve closes is called the closing pressure.

43
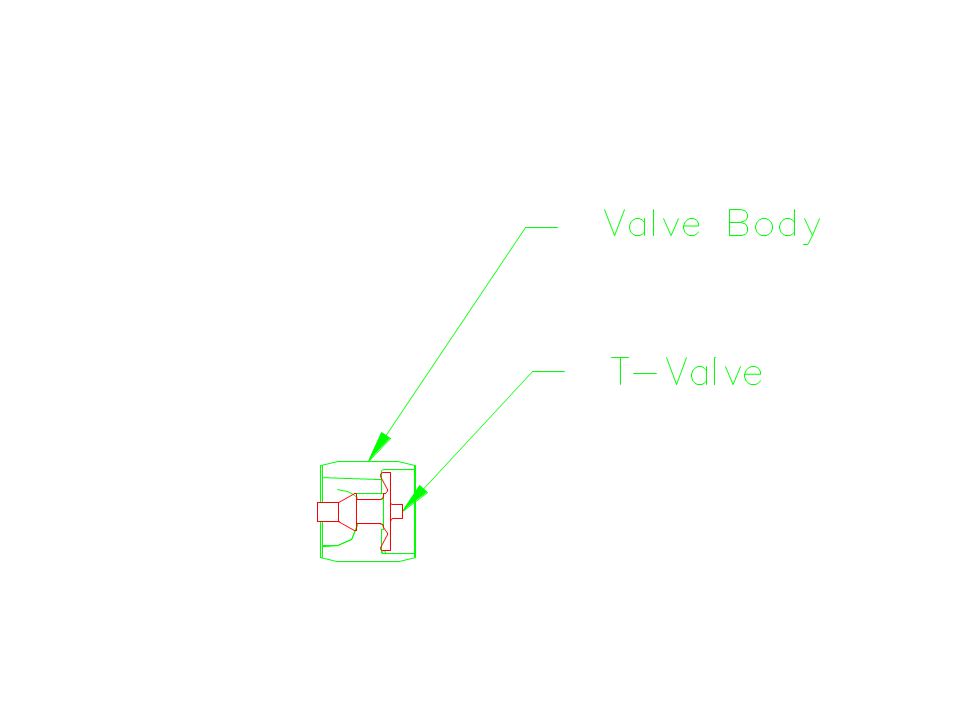
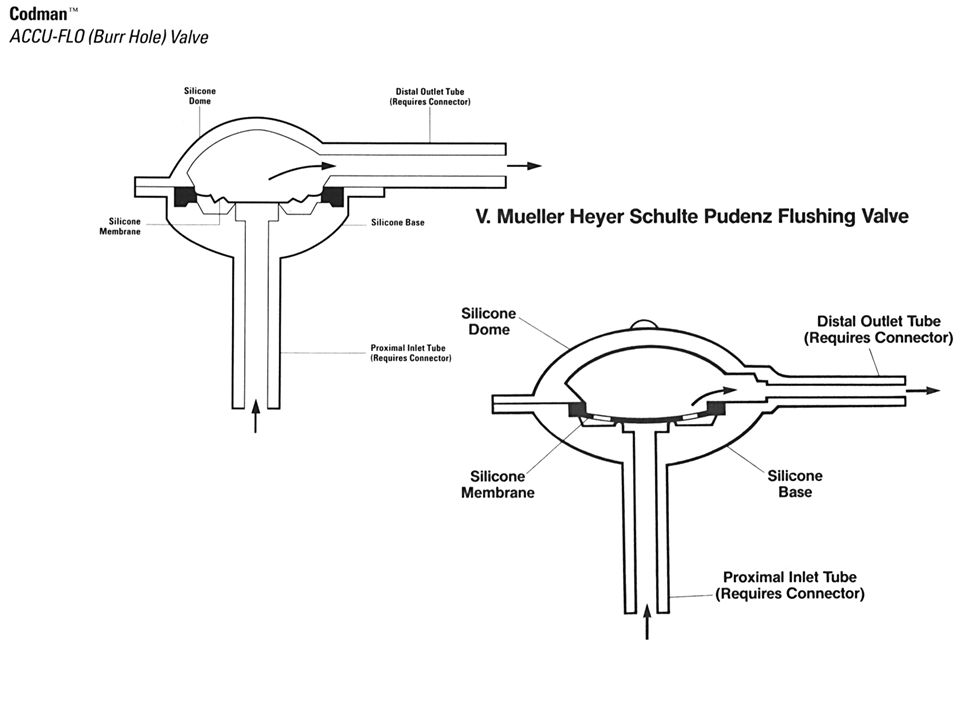
Valve Types Burr Hole - shaped to fit the hole made in the skull.
The reservoir is an integral part e.g. Pudenz Flat Bottom - rests flat against the skull distal to the ventricular catheter e.g. LPV II, Novus Cylindrical/In Line - appears “seamless” between the ventricular and peritoneal catheters e.g.. Ultra VS

45
Pudenz Pudenz

46
Mishler Dual Chamber Mishler Dual-Chamber

47
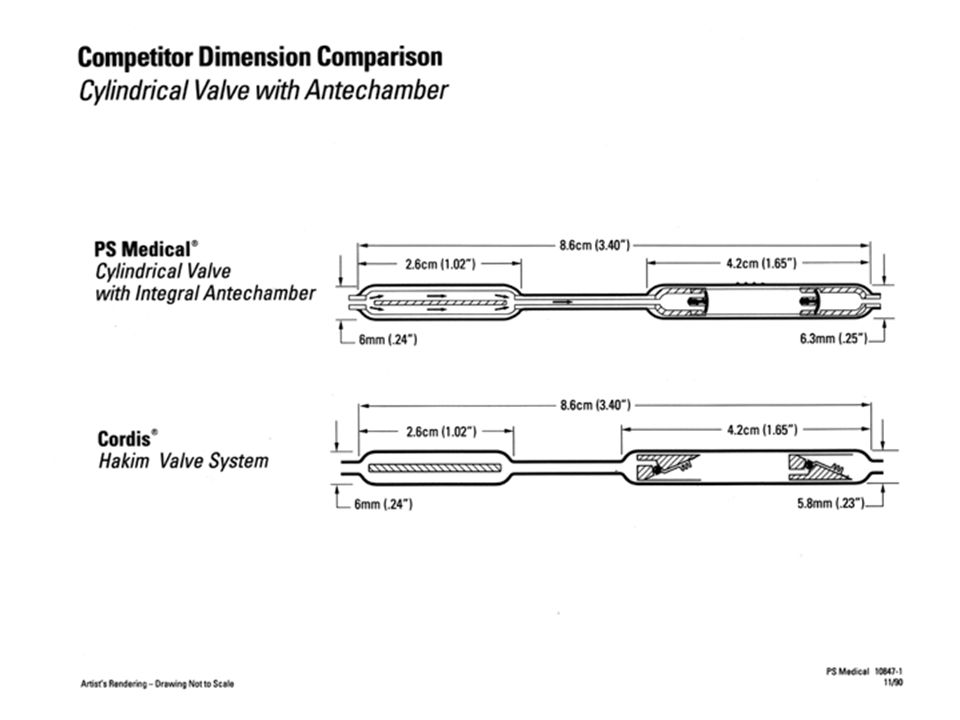
Ultra VS Ultra VS Cylindrical

48
One Piece One Piece Hydro Shunt

49
Ommaya Resevoirs Ommaya

51
Internal Valve Components
Slit Ball and Spring Miter Diaphragm

52
Valve Mechanisms Slit Miter

53
Valve Internal Mechanisms
High spring rate valves- open slowly, close quickly (miter, slit) Low spring rate valves- open quickly, close slowly (diaphragm, ball & spring, prone to siphon)
 Low spring rate valves- open quickly, close slowly (diaphragm, ball & spring, prone to siphon)")
54
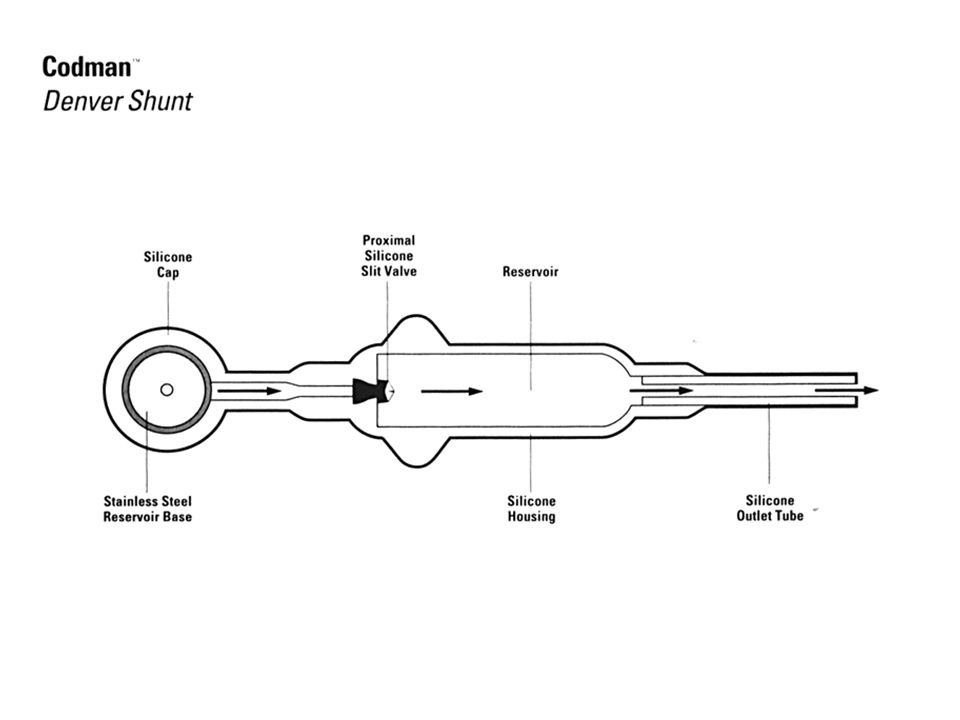
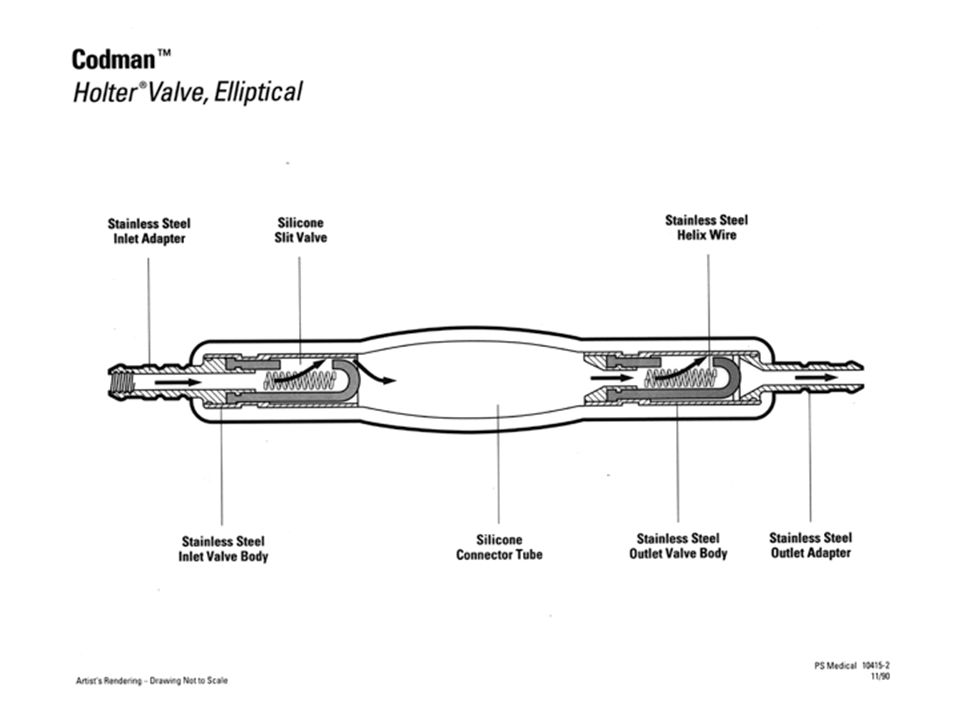
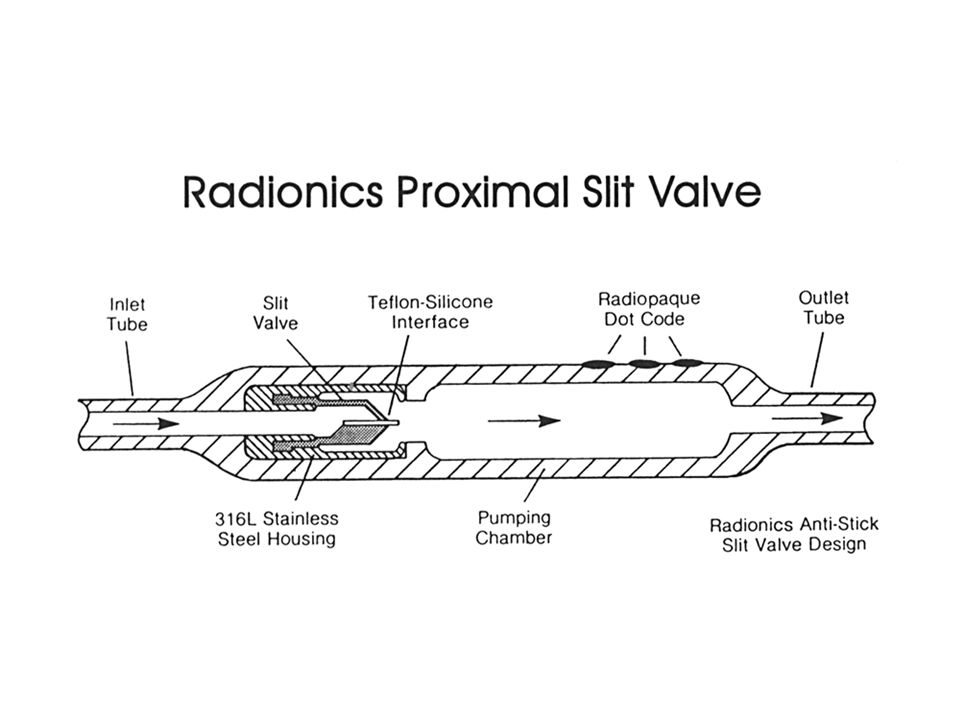
Valve Mechanisms Slit valves - a slit in a curved rubber layer. The flow arriving from the concave side opens slit, size of opening relating to the upstream pressure Can be proximal or distal Disadvantage: ”stickiness” of silicone rubber can affect opening Precision? Varies with age of valve?

55
Slit Valves Codman Radionics Phoenix Holter (proximal catheter/valve)
Denver (proximal catheter) Accuflo (distal catheter) Uni-shunt (distal catheter) Radionics Proximal slit valve Phoenix Holter-Hausner valve
 Accuflo (distal catheter) Uni-shunt (distal catheter) Radionics. Proximal slit valve. Phoenix. Holter-Hausner valve.")
56
One Piece One Piece Hydro Shunt

58
Valve Mechanisms “stickiness” of silicone rubber can affect opening
Mitre valves - the leaves of the “duckbill” part in response to the pressure differential. Pressure characteristics of mitre valve are related to size,shape, thickness and length of leaves. Disadvantage : “stickiness” of silicone rubber can affect opening

59
Mitre Valves Heyer-Schulte Ultra-VS(cylindrical)
Mishler Dual Chamber (flat bottom) Spetzler in-line Lumbar - Peritoneal valve (cylindrical)
 Spetzler in-line Lumbar - Peritoneal valve (cylindrical)")
61
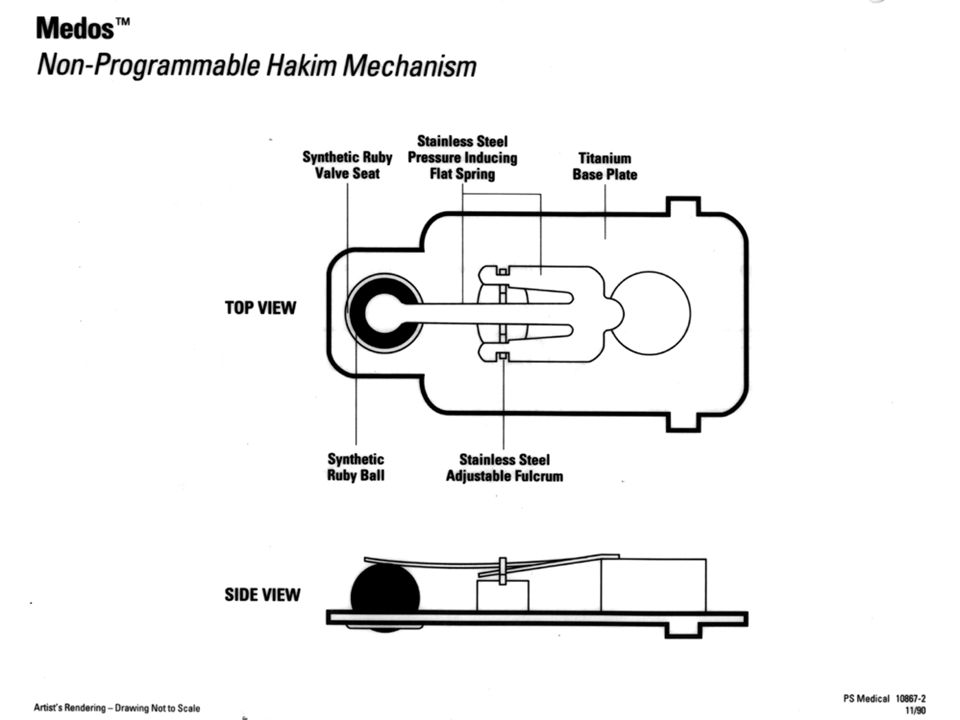
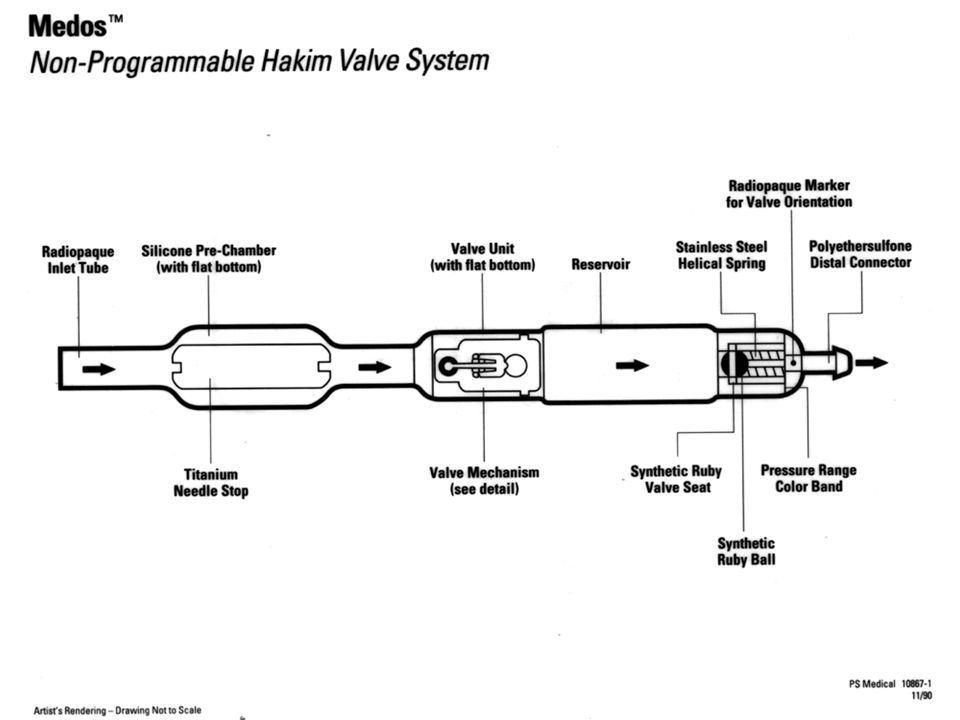
Valve Mechanisms Spring valves/Ball in cone - a metallic spring which applies force to a ball (usually ruby or sapphire) located in an orifice. Opening pressure is defined by spring stiffness Disadvantage: prone to obstruction from CSF debris or high protein content subject to siphoning
 located in an orifice. Opening pressure is defined by spring stiffness. Disadvantage: prone to obstruction from CSF debris or high protein content. subject to siphoning.")
62
Ball-in-Cone Valves Codman Medos Hakim NMT/Cordis Sophysa
Medos Programmable NMT/Cordis Atlas Hakim Orbis Sigma II Sophysa Sophy Programmable

64
Valve Mechanisms Diaphragm valves - a round diaphragm rests on or under a valve seat. Pressure causes the diaphragm to be detracted from the seat allowing CSF to flow Disadvantage: prone to siphoning in some designs flow is not laminar making it prone to obstruction

65
Diaphragm Valves Heyer-Schulte PS Medical/Medtronic Pudenz (burr hole)
LPV II (flat bottom) Novus (flat bottom) PS Medical/Medtronic Delta (Burr hole, flat bottom) Button(flat bottom) Contour (flat bottom)
 Novus (flat bottom) PS Medical/Medtronic. Delta (Burr hole, flat bottom) Button(flat bottom) Contour (flat bottom)")
66
Diaphragm Valves Radionics Codman Contour Flex Equi-flow Burr hole
Accu-flo valve

68
Valve Mechanisms Flow regulating mechanisms
Maintains same flow rate at any differential pressure by increasing or lowering its resistance to pressure May be achieved by a solid conical cylinder inserted inside a ring attached to a pressure sensitive membrane

69
Valve Mechanisms Inner diameter of ring is greater than larger
outer diameter of conical cylinder By reducing surface area, mechanism restricts amount of fluid that can go through Outer cylinder moves to compensate for reduced surface area to maintain flow rate.

72
Valve Mechanisms At very low pressures acts like a DP valve
At high pressures the ring moves beyond the central cylinder to give a “blow off” valve.

73
Treatment for Siphoning
In a vertical position, negative pressure from hydrostatic column can cause overdrainage Siphoning control achieved by adding siphon resistive devices to the shunt system. Functions as a second valve in line that closes in response to peritoneal pressure

75
Shunt Failures and Complications
Shunt failure is at a maximum in first few months after surgery (25-40% at one year follow-up) Then falls to 4-5% The mean survival for a shunt is approx 5 years
. Then falls to 4-5% The mean survival for a shunt is approx 5 years.")
76
Shunt Failures and Complications
Shunt obstruction (about % of all failures) Infection(between %) Mechanical failure due to disconnection Valve failure Overdrainage Patient/shunt mismatch
 Infection(between %) Mechanical failure due to disconnection. Valve failure. Overdrainage. Patient/shunt mismatch.")
77
Shunt Placement Procedure
Skin Incision Placement of Burr Hole Sbcutaneous dissection Tunnel the peritoneal catheter Open dura & place ventricular catheter Connect valve, test & clean Distal catheter insertion & skin closure

78
Shunt Implantation Approaches
Occipital Approach Temporal Approach Frontal Approach

79
Metopic Suture Coronal Suture Anterior Fontanelle Sagittal Suture Posterior Fontanelle Lamboidal Suture Skull of a newborn seen from above Adult human skull seen from above

80
Indications For Use of a Lumbar-Peritoneal Shunt
Communicating Hydrocephalus - when ventricles are small and it would be difficult to cannulate with a ventricular catheter. Normal Pressure Hydrocephalus - shunting without necessitating a cranial procedure.

81
Goals of Shunt Design & Development
Restoration of “normal physiology” in the shunted individual Maximize the potential quality of life for each patient Expand the population of successfully treated patients

82
First Generation Diaphragm Valve

83
Second Generation Diaphragm Valve

84
Third Generation Diaphragm Valve

86
Integra NeuroSciences Consistency by Design

87
FLOW PATH DELTA VALVE

92
at High Flow Rates (45.8ml/hr) LPV II Valve Performance
LPV Valve Performance at High Flow Rates (45.8ml/hr) LPV II Valve Performance at High Flow Rates (45.8ml/hr)
 LPV II Valve Performance. at High Flow Rates (45.8ml/hr)")
93
at Low Flow Rates (4.6ml/hr) LPV II Valve Performance
LPV Valve Performance at Low Flow Rates (4.6ml/hr) LPV II Valve Performance at Low Flow Rates (4.6ml/hr)
 LPV II Valve Performance. at Low Flow Rates (4.6ml/hr)")
98
Silicon…….. Single Cavity pressure mold

99
Body… polysulfone…. Injection molding

100
Body and Housing made of Polysulfone

101
Cross linked silicone dome

102
All parts are glued together by technicians using Self Leveling RTV (room temperature vulcanizer)
")
103
Integral connectors made of nylon

104
Base made up of a Silicone “sandwich” with a Dacron center

105
Needle Guard is …polypropylene

106
Tantalum is added for radio opaque markings showing flow direction and pressures (L,M,H)
")
107
Competitive Matrix Medtronic P.S. Medical Cordis Codman Radionics
Sophysa Phoenix

136
Flat Bottom Diaphragm Competitive Matrix

137
Flat Bottom Diaphragm Competitive Matrix

138
Burr Hole Diaphragm Competitive Matrix

139
Neonatal Valve Systems Competitive Matrix

140
Product line strengths
Consistency and predictability Broad product line Clnical support History Manufacturing expertise Pricing flexibility

Similar presentations

























































 deep within the brain. The excess fluid increases the size of the ventricles and puts extra.>")




