Download presentation
Presentation is loading. Please wait.

1
Assistant Professor Department of Paediatrics ANMC

2
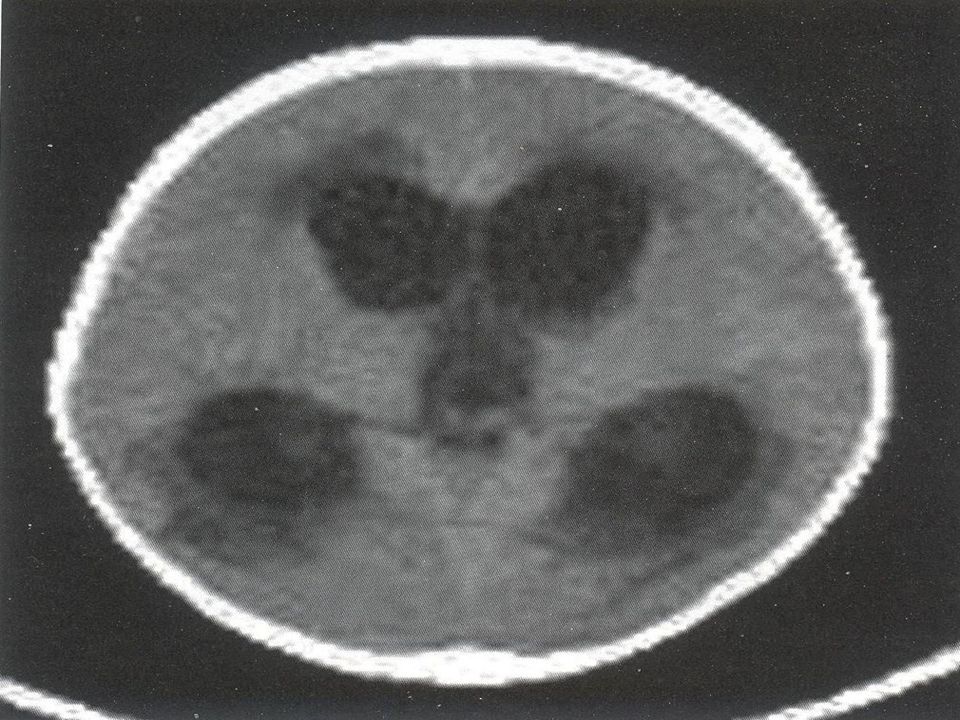
Hydrocephalus Hydrocephalus is the buildup of too much cerebrospinal fluid in the brain Normally, this fluid cushions the brain Hydrocephalus can be congenital present at birth, or acquired present after birth Congenital hydrocephalus Acquired hydrocephalus

3
Hydrocephalus CSF is formed primarily in the ventricular system by choroid plexus which is situated in the lateral, 3 rd and 4 th ventricles. In a normal child 20ml/hr CSF is produced Total volume of CSF in an infants is 50ml In adults 150ml

4
Types of hydrocephalus Obstructive or non communicating hydrocephalus Obstruction within the ventricular system. Nonobstructive or communicating hydrocephalus Hydrocephalus resulting from the obliteration of subarachnoid cisterns or malfunction of arachnoid villi

5
Causes of hydrocephalus Obstructive hydrocephalus Aqueductal stenosis Malformations Tumors Arnold chiari malformation Dandy walker malformation

6
Non obstructive hydrocephalus Meningitis Encephalitus Papilloma Subarachnoid hemorrhage

7
Symptoms include Headache Vomiting and nausea Blurry vision Balance problems Bladder control problems Thinking and memory problems

8
How is hydrocephalus diagnosed Typically hydrocephalus is discovered by the child’s parents or pediatrician when the child’s head begins to rapidly swell and enlarge Depending on child’s age (before six months), X ray skull Cranial Ultrasound CT scan brain MRI brain
, X ray skull Cranial Ultrasound CT scan brain MRI brain")
9
Treatment Medical management including; Acetazolamide and furosemide may provide temporary relief by reducing the rate of CSF production

10
Treatment for hydrocephalus Most often, hydrocephalus is treated surgically with the placement of a shunt to bypass the blockage that is causing the buildup, or to create a better flow of CSF Types of shunt VP shunt VA shunt VT shunt

11
Follow-up care is extremely important in tracking the progress of a child’s recovery. Pediatric neurosurgeon will schedule follow-up appointments to make sure your child is making a full recovery.

15
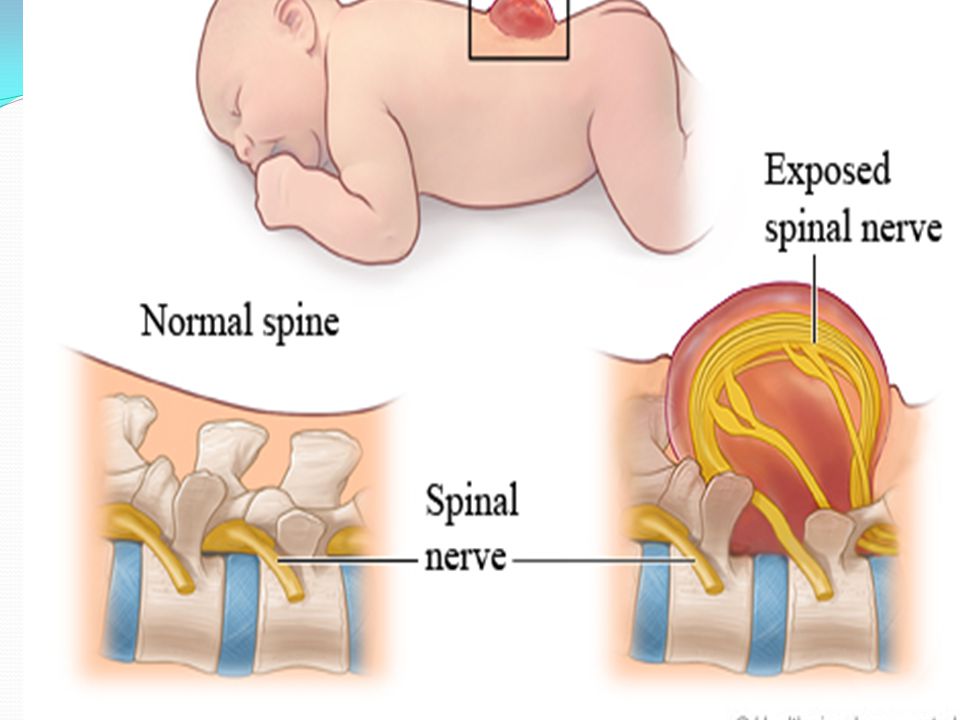
Spina bifida Spina bifida (Latin: "split spine") is a developmental congenital disorder caused by the incomplete closing of the embryonic neural tube Some vertebrae overlying the spinal cord are not fully formed and remain unfused and open If the opening is large enough, this allows a portion of the spinal cord to protrude through the opening in the bones
 is a developmental congenital disorder caused by the incomplete closing of the embryonic neural tube Some vertebrae overlying the spinal cord are not fully formed and remain unfused and open If the opening is large enough, this allows a portion of the spinal cord to protrude through the opening in the bones")
16
Spina bifida malformations fall into three categories: spina bifida occulta spina bifida cystica with meningocele spina bifida cystica with myelomeningocele The most common location of the malformations is the lumbar and sacral areas

17
Physical signs of spina bifida may include: Leg weakness and paralysis Orthopedic abnormalities (i.e., club foot, hip dislocation, scoliosis) Bladder and bowel control problems, including incontinence, urinary tract infections, and poor renal function Pressure sores and skin irritations Abnormal eye movement
 Bladder and bowel control problems, including incontinence, urinary tract infections, and poor renal function Pressure sores and skin irritations Abnormal eye movement")
18
Treatment There is no known cure for nerve damage caused by spina bifida To prevent further damage of the nervous tissue and to prevent infection, pediatric neurosurgeons operate to close the opening on the back

19
The spinal cord and its nerve roots are put back inside the spine and covered with meninges In addition, a shunt may be surgically installed to provide a continuous drain for the excess cerebrospinal fluid produced in the brain, as happens with hydrocephalus.

20
Surgeon Neurologist Urologist Opthalmoiogist Physical and occupational therapists

24
Prevention of spina bifida Primary prevention and secondary prevention Prognosis

Similar presentations








 or myelomeningocele (MY-eh-lo-me-NING-oh-seel )>")











 deep within the brain. The excess fluid increases the size of the ventricles and puts extra.>")


