Download presentation
Presentation is loading. Please wait.

1
AM Report- Thursday, July 28 th 2011

8
Clue: This patient was recently treated with Ampicillin

9
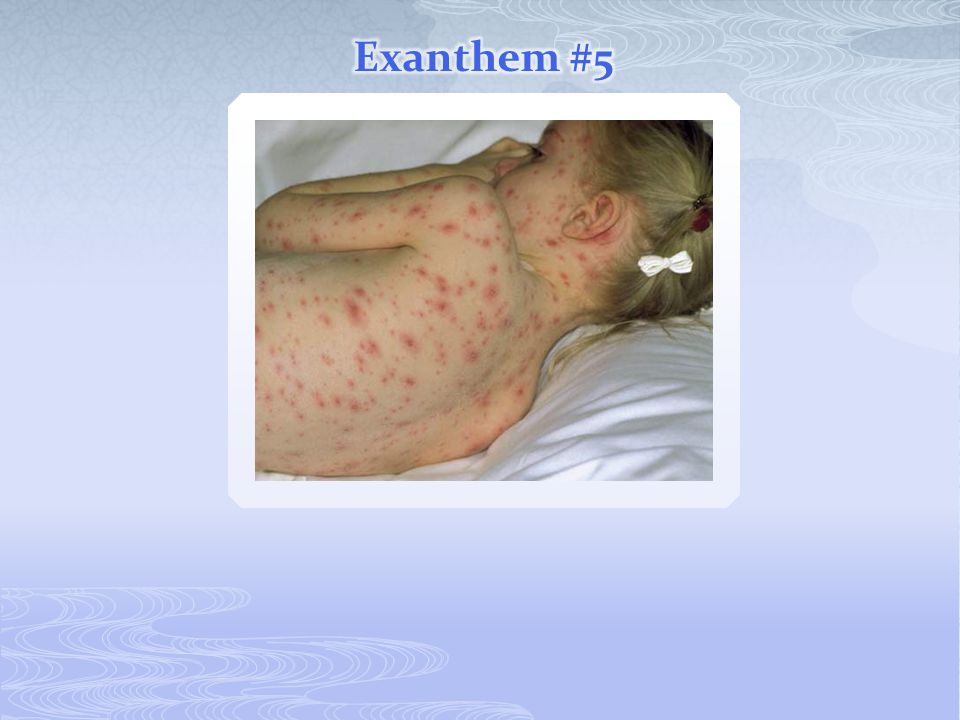
Clue: This patient had a h/o 3 days of fever (that has since defervesced) before the appearance of the rash
 before the appearance of the rash")
11
Clue: You might be more suspicious of this illness if this picture was a hypotensive woman

17
Koplik Spots

18
Exposure Fever, malaise Coryza, cough, conjunctivits Koplik spots Exanthum Exanthem: red/ purple papules appear at hairline, then spread downward (@ toes by day 3) Coalescence common on face and upper body Fades in same fashion (head toe) 24h8-12d 48h2-3d
 Coalescence common on face and upper body Fades in same fashion (head toe) 24h8-12d 48h2-3d")
19
Control Measures Isolation (airborne precautions) Immunization/ Immune globulin First determine who is susceptible <2 doses of MMR vaccine after the first birthday Low titers in response to vaccine administration No documentation of measles by a physician If susceptible: MMR vaccine within 72hours of exposure Immune globulin to household contacts or immunocompromised patients within 6 days of exposure if vaccine not given within 72h
 Immunization/ Immune globulin First determine who is susceptible <2 doses of MMR vaccine after the first birthday Low titers in response to vaccine administration No documentation of measles by a physician If susceptible: MMR vaccine within 72hours of exposure Immune globulin to household contacts or immunocompromised patients within 6 days of exposure if vaccine not given within 72h")
20
Hand, Foot, Mouth Disease

21
Echoviruses, Coxsackie A&B, Polio Primarily affect young children in the summer Accompanied by non-specific constitutional symptoms Exanthem displays impressive variability Urticarial, petechial, purpuric, vesicular, rubelliform, morbilliform, scarlatiniform Dx: Culture, nucleic acid amplification

22
Forchheimer Spots

23
In 2005, the CDC announced that rubella had been eliminated from the US But, it’s still on the Boards!! Epidemiology Spread by person-to-person transmission of infected droplets Patients are infectious a few days before the rash appears continuing through the first several days of the rash Peaks in late winter/ early spring

24
Exposure Tender adenopathy (post-auricular, posterior cervical, and occipital) Malaise, HA, low-grade fever, sore throat Exanthem (+/- Forchheimer spots) Exanthem: rose-pink maculopapules on face that spread quickly to involve trunk and then extremities Day 2: rash on face disappears, truncal rash coalesces Day 3: rash disappears 14-21 d 1-5 d
 Malaise, HA, low-grade fever, sore throat Exanthem (+/- Forchheimer spots) Exanthem: rose-pink maculopapules on face that spread quickly to involve trunk and then extremities Day 2: rash on face disappears, truncal rash coalesces Day 3: rash disappears d 1-5 d")
25
Highest rate of infection 1 st and 3 rd trimesters, morbidity associated with 1 st trimester infection Presentation: TTP Blueberry muffin lesions Radiolucencies in metaphyseal long bones PDA (or ASD/VSD) Sensorineural deafness Cataracts/ glaucoma HSM
 Sensorineural deafness Cataracts/ glaucoma HSM")
26
“Slapped cheek” appearance

27
Seen most often in children 4-15 in winter and spring Exposure HA, coryza, low-grade fever, malaise “slapped cheek appearance” erythematous, maculopapular rash on trunk and ext central clearing with lacy/ reticular appearance periodic increases in rash intensity (x1-3 wks) 4-15 d 7 d1-4 d end
 4-15 d 7 d1-4 d end")
28
Aplastic crisis in children with hemolytic anemias Chronic infection in immunocompromised patients Fetal infection Hydrops fetalis, fetal death, miscarriage Highest risk during second trimester

29
Vesicular lesions in different stages of healing

30
Exposure low-grade fever, malaise, HA vesicular exanthem crusting Exanthem: “dew drops on a rose petal,” occurs most commonly on trunk and extremities Contagious 1-2 days before rash appears and until all the lesions are crusted over 10-21d24-48h 3-5 d

31
Consider immune globulin (within 96h) for exposed susceptible children at risk for severe dz: Immunocompromised children Pregnant women Newborns whose mothers had varicella<5 days before delivery or <48h after Hospitalized premature infants >/= 28 weeks born to a varicella Ab-negative mother Hospitalized premature infants </= 28 weeksor <1000g
 for exposed susceptible children at risk for severe dz: Immunocompromised children Pregnant women Newborns whose mothers had varicella<5 days before delivery or <48h after Hospitalized premature infants >/= 28 weeks born to a varicella Ab-negative mother Hospitalized premature infants </= 28 weeksor <1000g")
32
Clue: This patient was recently treated with Ampicillin

33
Clue: This patient had a h/o 3 days of fever (that has since defervesced) before the appearance of the rash
 before the appearance of the rash")
34
Non-specific rubelliform eruption Central distribution (trunk, face, proximal extremities) Follows 3-5 days of spiking fevers in a young child Child looks well
 Follows 3-5 days of spiking fevers in a young child Child looks well")
35
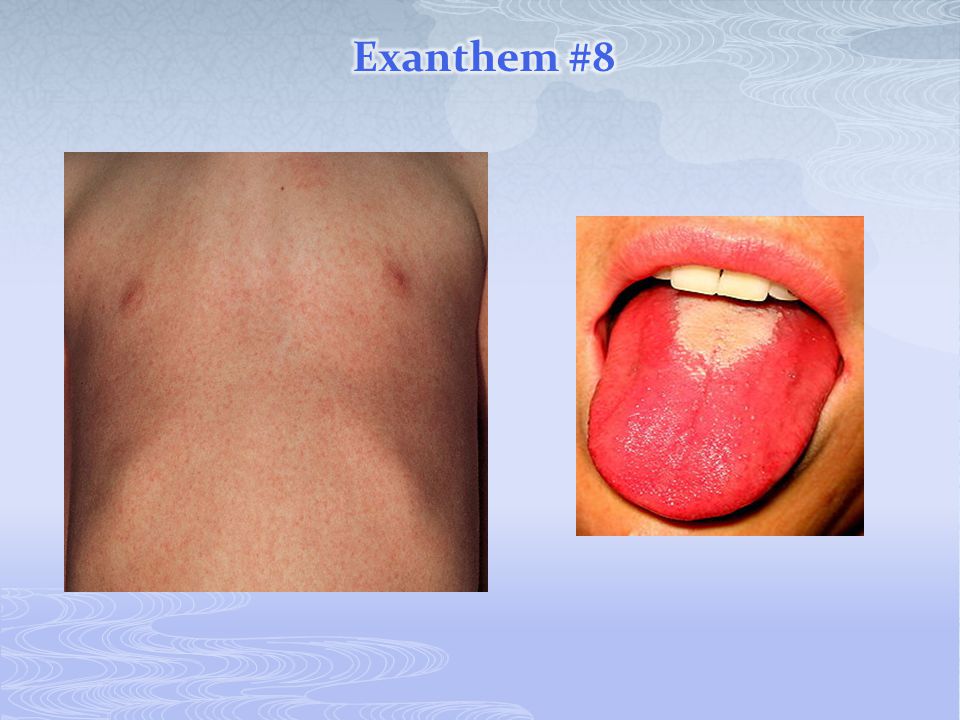
Sandpaper rash Strawberry Tongue

36
Acute streptococcal pharyngitis with fine, diffuse red rash “Sandpaper rash” Usually appears 24-48h after illness begins, but can be the presenting symptom Begins on neck and upper chest and spreads Lasts ~1wk, fades with subsequent desquamation of trunk, hands and feet

37
Clue: You might be more suspicious of this illness if this picture was a hypotensive woman

39
Impetigo Abscess Staph scalded skin Caused by exfoliating toxin Fever common, +/- bacteremia +Nikolsky sign Toxic Shock Syndrome Hypotension, fever, diarrhea, hypocalcemia Scarlatiniform erythroderma (within 24 h of fever), hyperemia of MM and conjuntivae Can also be caused by Group A Strep (pyogenes)- post- op and with chicken pox
, hyperemia of MM and conjuntivae Can also be caused by Group A Strep (pyogenes)- post- op and with chicken pox")
41
Major causes: Drugs: Abx (BACTRIM!!), anticonvulsants, NSAIDS Infectious: Herpes virus, Mycoplasma Prodrome of fever and malaise erythematous or purpuric macules or plaques sloughing Mucous membrane involvement: Erythema Multiforme (0) SJS ( 30%)
, anticonvulsants, NSAIDS Infectious: Herpes virus, Mycoplasma Prodrome of fever and malaise erythematous or purpuric macules or plaques sloughing Mucous membrane involvement: Erythema Multiforme (0) SJS ( 30%)")
42
Bright red diaper area with desquamation Red, cracked lips; conjuntivitis Red palms

43
Clinical criteria: Fever lasting >/= 5days plus 4 of the following: Bilateral bulbar conjunctival injection Oral mucous membrane changes Peripheral extremity changes Polymorphous rash (greatly variable) Cervial LAD (with at least 1 LN> 1.5cm in diameter)
 Cervial LAD (with at least 1 LN> 1.5cm in diameter)")
44
~Caused by Neisseria meningitidis ~Usually seen in patients < 2yo ~Penicillin G is treatment of choice (once Neisseria is confirmed) ~Hearing loss is a common complication of meningococcal meningitis
 ~Hearing loss is a common complication of meningococcal meningitis")
46
Caused by the Gm- coccobacillus Rickettsia rickettsii, which is transmitted by tick bite Usually seen in Southeastern US Clinical course Abrupt onset of fever, HA, myalgias After 2-5 days, exanthem appears Maculopapular Distribution involves flexural areas of wrists and ankles then spreads toward the center Becomes petechial within 1-3 days, then confluent and hemorrhagic with areas of necrosis

47
Have a low threshold to treat Doxycycline for all ages

48
A 6-day-old infant is brought to the emergency department in August with a 1-day history of decreased feeding, decreased activity, tactile fever, and rapid breathing. He was born at term by normal spontaneous vaginal delivery and weighed 3,742 g. His mother reports that she had a nonspecific febrile illness 1 week before delivery for which she received no treatment. Her group B Streptococcus screen was positive at 36 weeks' gestation, and she received two doses of ampicillin (>4 hours apart) during labor. The baby received no antibiotics and was discharged at 48 hours of age. Physical examination today reveals a toxic, lethargic infant who is grunting and has a temperature of 39.4°C, heart rate of 180 beats/min, and respiratory rate of 60 breaths/min. His lungs are clear, with subcostal retractions. He has a regular heart rhythm with gallop, his pulses are thready, his capillary refill is 4 seconds, and his extremities are cool. Of the following, the MOST likely cause of this baby's illness is: A. early-onset group B Streptococcus infection B. echovirus 11 infection C. herpes simplex virus infection D. hypoplastic left heart syndrome E. respiratory syncytial virus infection
 during labor. The baby received no antibiotics and was discharged at 48 hours of age. Physical examination today reveals a toxic, lethargic infant who is grunting and has a temperature of 39.4°C, heart rate of 180 beats/min, and respiratory rate of 60 breaths/min. His lungs are clear, with subcostal retractions. He has a regular heart rhythm with gallop, his pulses are thready, his capillary refill is 4 seconds, and his extremities are cool. Of the following, the MOST likely cause of this baby s illness is: A. early-onset group B Streptococcus infection B. echovirus 11 infection C. herpes simplex virus infection D. hypoplastic left heart syndrome E. respiratory syncytial virus infection.")
49
A 13-year-old girl presents with a 2-day history of fever, sore throat, and a rash that began on her arms and legs and spread to her chest and back. Physical examination reveals pharyngeal exudate; bilateral cervical adenopathy; and a "sandpapery" rash over her arms (Item Q157), legs, and trunk. A rapid diagnostic test for group A Streptococcus yields negative results. At 48 hours, a throat culture is growing small colonies with narrow bands of hemolysis on sheep blood agar. Of the following, the MOST appropriate antibiotic for treating this patient is(Item Q157) A. ceftazidime B. erythromycin C. penicillin D. tetracycline E. trimethoprim-sulfamethoxazole
, legs, and trunk. A rapid diagnostic test for group A Streptococcus yields negative results. At 48 hours, a throat culture is growing small colonies with narrow bands of hemolysis on sheep blood agar. Of the following, the MOST appropriate antibiotic for treating this patient is(Item Q157) A. ceftazidime B. erythromycin C. penicillin D. tetracycline E. trimethoprim-sulfamethoxazole.")
Similar presentations




























 Disease (strep throat, necrotizing fasciitis, impetigo) By: Dr. Awatif Alam.>")
 Primary infection results in varicella (chickenpox) Recurrent infection results in herpes zoster (shingles) Short.>")

>")
