Download presentation
Presentation is loading. Please wait.

1
Cerebral Vascular Accident
STROKE

3
RISK FACTORS FOR STROKES
Nonmodifiable Age- incidence ↑ with age until age 75. Race- higher in African Americans Gender- higher in men Heredity- family history increases risk Potentially Modifiable Lifestyle- excessive alcohol, cigarette smoking, obesity, high fat diet, drug abuse. Pathologic conditions- cardiac disease, DM, HTN, migraine headaches, hypercoagulability states.

5
ETIOLOGY AND PATHO Extra-cranial factors- related to the circulatory system. Systemic blood pressure- <70 and >160 cardiac output- when reduced by 30% cerebral blood flow is reduced. Blood viscosity- anemia increases cerebral blood flow and polycythemia reduces it.

6
INTRACRANIAL FACTORS A. Metabolic factors
Increased CO2 and low O2 results in vasodilation to restore blood flow to normal. CO2 is the most potent regulator of cerebral blood flow. Increased Hydrogen ion concentration increases cerebral blood flow.

7
Intracranial factors, cont’d
B. Blood vessels The condition of the blood vessels supplying the brain is important!!! Potential problems- congenital anomalies (tortuosity, coiling, kinking, and AV malformations). The malformations interfere with cerebral blood flow and contribute to atherosclerotic disease Collateral circulation develops Circle of Willis
. The malformations interfere with cerebral blood flow and contribute to atherosclerotic disease. Collateral circulation develops. Circle of Willis.")
8
Intracranial factors, cont’d
C. Intracranial pressure ICP increases with an assault to brain. Causes of ICP: stroke, neoplasms, inflammation, trauma, and hydrocephalus. ICP compresses the brain and reduces cerebral blood flow, which may lead to infarct. Both extracranial and intracranial factors may lead to stroke

9
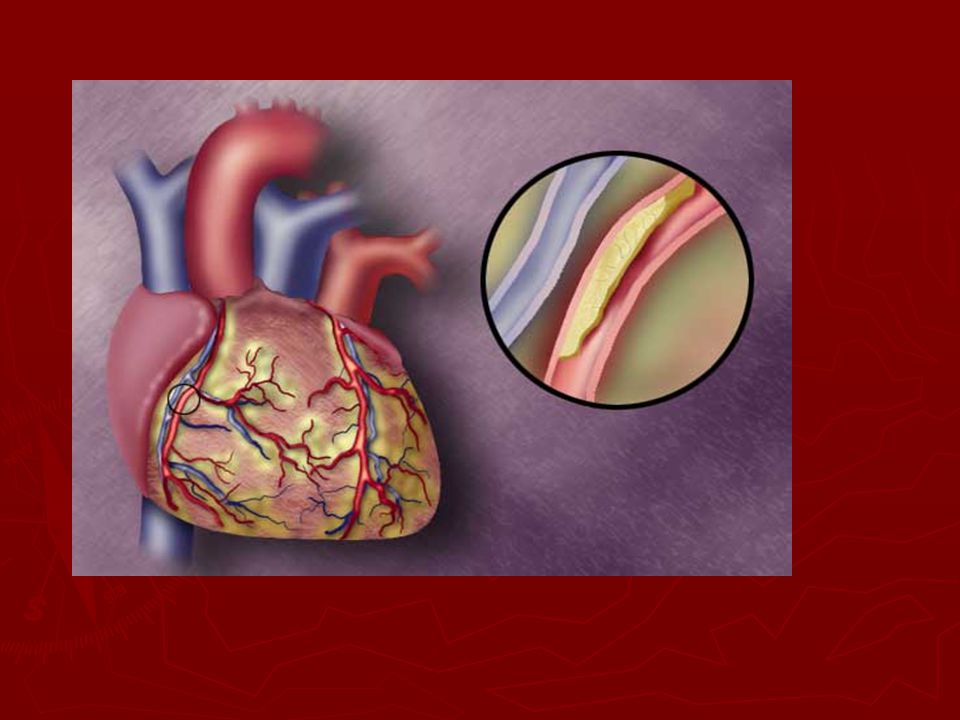
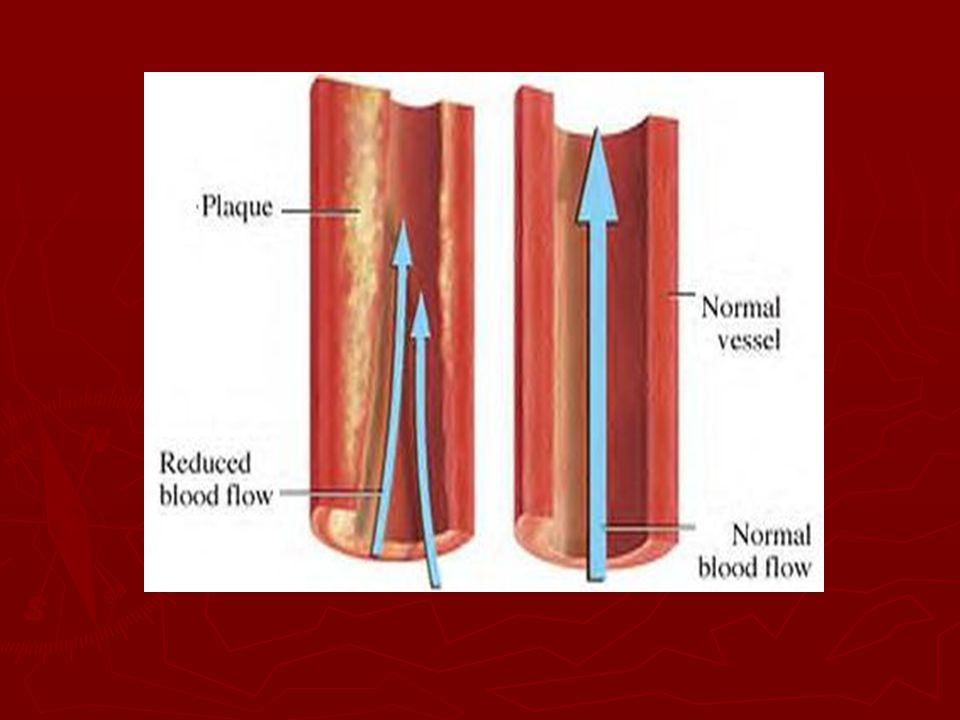
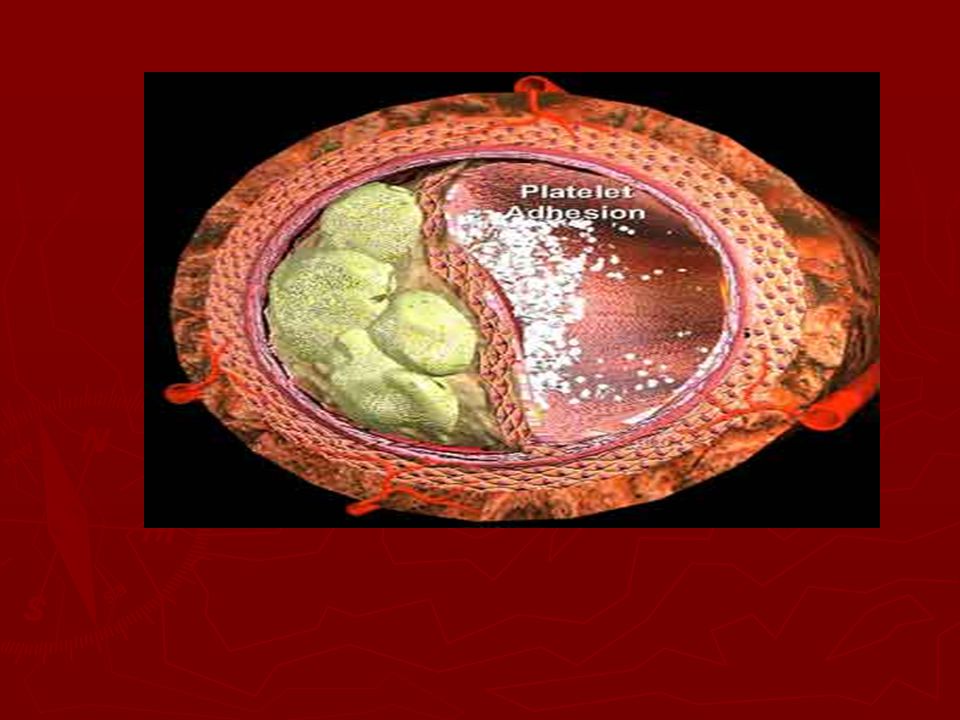
Atherosclerosis An abnormal accumulation and infiltration of in the intima of the arteries. Plaques develop in an area of high turbulence; which may later damage the plaque. Platelets and fibrin aggregate or collect on the surface of the plaque. Parts of the plaque breaks off and travel to a narrower distal artery Cerebral infarct occurs.

13
TYPES OF STROKE Ischemic: Most common type of stroke!
Occurs due to decreased blood flow to an area of the brain due to partial or complete occlusion of and artery due to thrombosis. This lack of blood, oxygen and nutrients to an area of the brain causes necrosis of cerebral tissue. Two types: thrombotic and embolic See Lewis, page 1648; table 55-1.

14
Thrombotic stroke Most common cause of cerebral infarct!
Cause: Due to formation of a blood clot or coagulation of blood that results in narrowing of blood vessel or occlusion. 2/3 of strokes due to HTN or DM. (accelerate the atherosclerotic process) May also be due to oral contraceptives, coagulation disorders, polycythemia, arteritis, chronic hypoxia and dehydration.
 May also be due to oral contraceptives, coagulation disorders, polycythemia, arteritis, chronic hypoxia and dehydration.")
16
Thrombotic Stroke Thrombotic strokes are usually proceeded by prodromal episodes (warnings) called TIA’s (transient ischemic attacks). TIA’s last from 5 to 30 minutes. Include- paresis or decreased strength and motion of an extremity. Aphasia or disturbance of language function, Paralysis, mental confusion, or visual disturbances.

17
Thrombotic stroke The extent of the stoke depends on rapidity of onset, size of lesion, and presence collateral circulation. There is a pattern to thrombotic stroke! 1. single attack; symptoms occur over several hours 2. intermittent progression toward a stroke over hours or days. 3. partial stroke with permanent neuro deficits 4. series of TIA’s followed by a stroke with permanent neuro deficits.

18
Thrombotic stroke Symptoms at 72 hours are usually due to resulting edema to tissues; symptoms improve after edema subsides 2 weeks). This type of stroke occurs during or after stroke.

21
EMBOLIC STROKE Cerebral embolism results from occlusion of cerebral artery by an embolus. Necrosis and cerebral edema results. Embolus is the second most common cause of stroke. Most emboli originate in the endocardium with plaques or tissue breaking off and entering circulation.

23
Embolic Stroke Emboli are associated with heart conditions such as;
A fib MI Infective endocarditis Rheumatic heart disease Valvular prostheses ASD

24
Embolic stroke Less common causes of emboli: Air
Fat from long bone fracture Amniotic fluid postpartum tumors

25
Embolic stroke Prodromal warning less likely; single events
sudden onset Most commonly related to head trauma High rate of re-occurrence if cause is not treated.

26
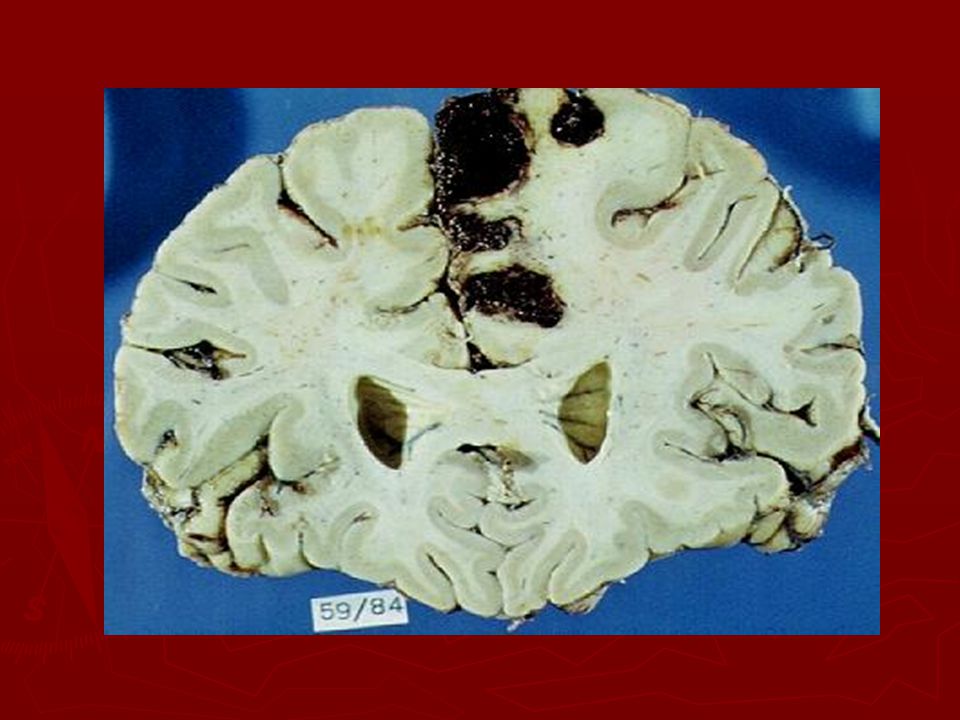
Hemorrhagic stroke Intracerebral hemorrhage is bleeding within the brain caused by rupture of a blood vessel that lasts from minutes to days. Most commonly caused by HTN May be caused by brain tumors, trauma, thrombolytic drugs, and ruptured aneurysms.

27
Hemorrhagic stroke Blood within the closed area of the brain imposes pressure on the brain tissue and displaces brain tissue and decreases blood flow to brain. Clinical manifestations depends on the site and amount of hemorrhage and resultant damage. Poor prognosis; 70% die

29
Subarachnoid stroke Caused by aneurysms, AV malformations, trauma, and HTN. May have prodromal symptoms if ballooning or dilation applies pressure to brain tissue. May suddenly rupture, causing neuro changes Majority of aneurysms are in the Circle of Willis

30
Subarachnoid hemorrhage, cont’d
If aneurysm leaks, pt may have a headache! Rupture of aneurysm causes pressure in subarachnoid space due to bleeding. Clinical manifestations: Headache, lethargy, confusion, nausea, vomiting, fever, neck pain, and backaches, paralysis, coma and death. Massive hemorrhage is defines as 30 to 50 ml of blood. Watch for re-bleeding when clot starts to dissolve. (usually within first 2 weeks post rupture). Reduce activity and prevent straining.
. Reduce activity and prevent straining.")
31
Temporal Development of CVA
Transient Ischemic Attacks (TIA’s)- Brief episodes of neuro manifestations (less than 24 hours). Leaves no residual effects Three categories: 1/3 never have another TIA 1/3 will have more than one TIA 1/3 will have a stroke WARNING SIGNS OF PROGRESSING CVA!
- Brief episodes of neuro manifestations (less than 24 hours). Leaves no residual effects. Three categories: 1/3 never have another TIA. 1/3 will have more than one TIA. 1/3 will have a stroke. WARNING SIGNS OF PROGRESSING CVA!")
32
TIA’s s/s vary depending on the part of brain affected. Treatment:
Medications such as aspirin, Persantine (dipyridamole), Ticlid, and anticoagulant medication. Long term therapy post TIA Surgical treatment- carotid endartarectomy, extra-cranial- intracranial bypass (EC-IC bypass), and transiluminal angioplasty.
, Ticlid, and anticoagulant medication. Long term therapy post TIA. Surgical treatment- carotid endartarectomy, extra-cranial- intracranial bypass (EC-IC bypass), and transiluminal angioplasty.")
33
Reversible ischemic Neurologic Deficit
A neuro deficit which remains 24 hours after onset; but leaves no residual signs or symptoms. Considered a completed stroke with minimal to no residual deficits

34
Stroke –In- Evolution A progressive stroke which develops over hours or days. Characteristic of an enlarging intra-arterial thrombus. A stepwise or intermittent progression of deterioration of neurological symptoms. Manifestations do not resolve and leave residual damage.

35
Completed Stroke Neuro defects unchanged over 2 to 3 days.
Usually embolic in nature Also called “stable stroke”. Signals readiness for aggressive rehab therapy. (unless an aneurysm is involved).
.")
36
Clinical Manifestations
All deficits are directly related to area of brain that is involved. See Lewis, page 1650, Table 55-2.

37
Neuromotor Function Destruction of motor neurons in the pyramidal pathway causes: Mobility Respiratory function Swallowing and speech Gag reflex Self-care abilities

38
Motor deficits Loss of skilled voluntary movement (akinesia).
Impairment of integration of movements Alterations in muscle tones Alteration in reflexes Initial hypo-reflexia which progresses to hyper-reflexia for most patients.

39
Patterns of deficits Contralateral deficits
A lesion on one side of the brain affects the motor function on the other side of the brain. The arms and legs on the affected side may be weak or paralyzed to different degrees depending the degree of cerebral circulation compromised. See Lewis, Page 1651; Table 55-5

40
The affected shoulder tends to rotate internally; the hip rotates externally.
The affected foot is plantar flexed and inverted. An initial period of flaccidity may lasts for several days to weeks. Spasticity of muscles follows the flaccid stage and is related to interruption of upper neuron influence.

41
Communication Aphasia- total loss of comprehension and use of language due to damage to the dominant hemisphere (left hemisphere). Dysphasia-dysfunction related to comprehension or use of language due to partial disruption or loss. Non-fluent (minimal speech activity with slow speech that requires obvious effort) Fluent- (speech is present, but contains little meaningful communication).
 Fluent- (speech is present, but contains little meaningful communication).")
42
Communication Conductive aphasia- mixture of both expressive and receptive aphasia Global aphasia- results from a massive lesion and there is virtual loss of all language ability.

43
Communication, cont’d Wernicke’s area damage Boca’s area damage
Receptive aphasia where neither the sound or speech or its meaning can be understood. Impaired comprehension of both spoken and written language. Boca’s area damage Expressive aphasia (difficulty speaking and writing) Dysarthria- disturbance in muscular control of speech. (pronunciation, articulation, phonation) DOES NOT EFFECT COMPREHENSION OF LANGUAGE.
 Dysarthria- disturbance in muscular control of speech. (pronunciation, articulation, phonation) DOES NOT EFFECT COMPREHENSION OF LANGUAGE.")
45
Affect May be unable to control emotions
May be depressed RT body image and loss of function May be frustrated RT immobility and communication issues

46
Intellectual Function
Memory and judgment may be impaired Left-sided stroke patients are more cautious in judgment and movement. Right-sided stroke patients more impulsive and move quicker.

47
Spatial-Perceptual Alterations
Right sided stroke patient has more spatial-perceptual orientation issues: Erroneous perception of self and illness (may deny illness or body parts). Erroneous perception of self in space (may ignore affected side; can’t judge distances) Agnosia or inability to recognize an object by sight, touch or hearing. Apraxia or the inability to carry out learned sequential movements on command.
. Erroneous perception of self in space (may ignore affected side; can’t judge distances) Agnosia or inability to recognize an object by sight, touch or hearing. Apraxia or the inability to carry out learned sequential movements on command.")
48
Elimination Most occur initially and are transient.
Frequent constipation DT immobility, weak abdominal muscles, dehydration, and diminished defecation reflexes. Urinary and bowel elimination may be DT functional inabilities to express needs and manage clothing.

49
Diagnostic Studies CT Scan- indicate size and location of lesion, differentiates between infarct and hemorrhage, effectiveness of treatment, and evaluate the course of healing. MRI- considered best method to differentiate between hemorrhage and infarct.

50
Diagnostics PET shows chemical activity and depicts extent if tissue damage. DSA- IV or arterial injection of contrast material to visualize blood vessels. TDA- transcranial doppler measures velocity of cerebral blood flow in the arteries, also detects micro-emboli. LP may be done to detect blood or WBC’s (not done if increased ICP is suspected)
")
52
Collaborative care PREVENTION Healthy diet Weight control
Regular exercise No SMOKING Limiting alcohol Routine health assessment

53
DRUG THERAPY Prophylactic low dose aspirin, daily.
Persantine 50 mg 3 X day decreases platelet aggregation which helps to decrease risk of thrombus and embolus formation. TICLID or PLAVIX- platelet aggregation inhibitors

54
Surgical Therapy Carotid endarterectomy (CEA)- the atheromatous lesion is removed from the carotid artery to improve blood flow Decreases stroke and death in patient with TIA’s. Done on patient with 70-99% occlusion

55
Transluminal Angioplasty
Insertion of balloon to open stenosed artery to permit blood flow. Patient with symptomatic stenosis of vertebrobasilar or carotid arteries Risk of dislodging emboli

56
EC-IC BYPASS Extracranial-intracranial bypass
Used when obstruction cannot be removed directly A branch of extracranial artery is anastomosed to a branch of intracranial artery just beyond the area of obstruction. Patients at high risk for stroke and require close-long term assessment and management.

57
ACUTE CARE Table 55-5; Lewis page 1654. Initially
Ensure patent airway DT altered level of consciousness. Remove dentures Administer oxygen via nasal cannula or non-rebreather mask DT respiratory distress

58
Acute Care Establish IV access with normal saline to maintain BP
Remove clothing Obtain immediate CT Scan Monitor VS, LOC, O2 sats, cardiac rhythms, Glasgow Coma Scale, pupil size and reactivity.

59
Acute Care Maintain patient warmth Reassure patient and family

60
Ischemic Cascade Series of events in response to thrombotic and embolic strokes. Ischemic area becomes discolored and soft, initially. However, around the border there is an area of perfusion called the ischemic penumbra that maintains perfusion for 3 to 6 hours post stroke. If adequate blood flow is reinitiated during this period, less neuro damage results

61
Treatment Control fluid and electrolyte balance
Adequate hydration promotes perfusion to the brain; however over hydration may increase cerebral edema! Total intake (oral, tube feedings, IV etc., per day) Monitor urine output ( if ADH released urine output will decrease)
 Monitor urine output ( if ADH released urine output will decrease)")
62
Treatment IV solutions with glucose and water are avoided. (hypertonic solutions may increase cerebral edema) Increased ICP from cerebral edema peaks in 72 hours and may cause brain herniation.

63
How to manage ICP Enhance venous drainage by: Elevating HOB
Maintain head and neck in alignment Avoidance of hip flexion Limit cerebral tissue metabolism and vasodilation by: avoiding hyperthermia, avoiding hypervolemia, manage constipation

64
Medications Diuretics (decrease cerebral edema) Mannitol (Osmitrol)
Lasix, (Furosemide) Dexamethasone for patients with vasogenic edema
 Dexamethasone for patients with vasogenic edema.")
65
Drug Therapy Thrombolytic therapy
Recombinant tissue plasminogen activator (t-PA)- to re-establish blood flow and prevent cell death for patients with ischemic strokes. Patients who receive t-PA within 3 hours after a stroke more likely to have 32% less injury three months after stroke. T-PA works by lysis thrombus/clot by binding and digesting the fibrin and fibrinogen.
- to re-establish blood flow and prevent cell death for patients with ischemic strokes. Patients who receive t-PA within 3 hours after a stroke more likely to have 32% less injury three months after stroke. T-PA works by lysis thrombus/clot by binding and digesting the fibrin and fibrinogen.")
66
t-PA Clot specific Less likely to cause hemorrhage as compared to streptokinase or urokinase. Single most important factor is timing!!!

67
t-PA Patients are screened for coagulation disorders, GI bleeding, and hemorrhagic stroke before initiation of treatment. Major side effect is cerebral hemorrhage. Monitor VS during treatment/ control BP O anticoagulants or antiplatelet drug for 25 hours post treatment.

68
Platelet inhibition/anticoagulant therapy
Heparin, coumadin, aspirin, ticlipidine (Ticlid), clopidrogel (Plavix), dipyridamole (Persantine). Contraindicated for patients with hemorrhagic strokes Monitor PT/ PTT Monitor patient for bleeding
, clopidrogel (Plavix), dipyridamole (Persantine). Contraindicated for patients with hemorrhagic strokes. Monitor PT/ PTT. Monitor patient for bleeding.")
69
Drug therapy Calcium channel blockers are given for patients with hemorrhagic strokes. Excess intracellular calcium may be harmful to brain tissue. Nimodipine (Nimotop) decreases effects of vasospasm and minimizes tissue damage. Aspirin decreases platelet aggregation at site of plaque.
 decreases effects of vasospasm and minimizes tissue damage. Aspirin decreases platelet aggregation at site of plaque.")
70
Drug therapy Tylenol treats hyperthermia
Dilantin may be given for seizures

Similar presentations














>")

 Stroke - Overview Third leading cause of death in industrialized countries. Total cost of strokes in the U.S. is roughly.>")
 Most common in older adults – Heart.>")







 Megan McClintock, MS, RN Megan McClintock, MS, RN11/4/11.>")
