Download presentation
Presentation is loading. Please wait.

1
توانبخشی: Rehabilitation
یک فرایند پویا و سلامت نگر است که به بیمار یا فرد ناتوان( دچار محدودیت جسمی، روحی، معنوی، اجتماعی و اقتصادی) کمک می کند جزء جدایی ناپذیر پرستاری است هدف از توانبخشی: بازگرداندن استقلال بیمار با گرداندن او به سطح عملکردی قبل از صدمه یا بیماری در کوتاهترین زمان ممکن است و اگر این امکانپذیر نباشد هدف رساندند بیمار به حداکثر استقلال و کیفیت زندگی قابل قبول است.
 کمک می کند. جزء جدایی ناپذیر پرستاری است. هدف از توانبخشی: بازگرداندن استقلال بیمار با گرداندن او به سطح عملکردی قبل از صدمه یا بیماری در کوتاهترین زمان ممکن است و اگر این امکانپذیر نباشد هدف رساندند بیمار به حداکثر استقلال و کیفیت زندگی قابل قبول است.")
2
تیم توانبخشی بیمار خانواده بیمار پرستار توانبخشی پزشک
پزشک متخصص توانبخشی فیزیوتراپیست کاردرمانگر گفتاردرمان روانشناس مددکار متخصص اورتوز و پروتز

3
حیطه های تخصصی در خدمات توانبخشی
توانبخشی بیماران دارای ضایعات مغزی و نخاعی توانبخشی ارتوپدی توانبخشی قلبی توانبخشی تنفسی توانبخشی سوختگی توانبخشی اعتیاد

4
بررسی تواناییهای عملکردی
مشاهده بیمار ADL(activity of daily living) – IADL(instrumental activity of daily living) شامل فعالیتهای روزمره زندگی: غذاخوردن، لباس پوشیدن، دفع و فعالیتهای سودمند شامل: توانایی خرید، انجام امور مالی و مقیاس عملکردی مستقل(FIM) مقیاس PULSES Bartel index سیستم مشاوره و ارزشیابی بیمار
 – IADL(instrumental activity of daily living) شامل فعالیتهای روزمره زندگی: غذاخوردن، لباس پوشیدن، دفع و فعالیتهای سودمند شامل: توانایی خرید، انجام امور مالی و مقیاس عملکردی مستقل(FIM) مقیاس PULSES. Bartel index. سیستم مشاوره و ارزشیابی بیمار.")
5
فرایند پرستاری بیمار دچار ناتوانی در مراقبت از خود-ADl
بررسی تشخیص برنامه ریزی و اهداف مداخلات: پرورش تواناییهای مراقبت از خود توصیه برای وسایل کمکی کمک به بیمار برای پذیرش محدودیتها ارزشیابی: تا حد امکان مستقلا امور روزمره زندگی را انجام دهد استفاده از وسایل کمکی به طور درست عدم ابتلا به عوارض

6
فرایند پرستاری بیمار دچار اختلال حرکتی
بررسی تشخیص برنامه ریزی و اهداف مداخلات: قرار دادن بیمار در وضعیتی مناسب برای پیشگیری از عوارض اسکلتی-عضلانی: انواع پوزیشن ها: طاقباز یا خوابیده به پشت supine - dorsal خوابیده به پهلو یا Lateral – side lying دمر یا روی شکم Prone در هر کدام از این حالتها بیمار در راستای صحیح بدن قرار داده شود و از فشار آمدن به عضلات و مفاصل جلو گیری شود. به وسیله بالش یا آتل

7
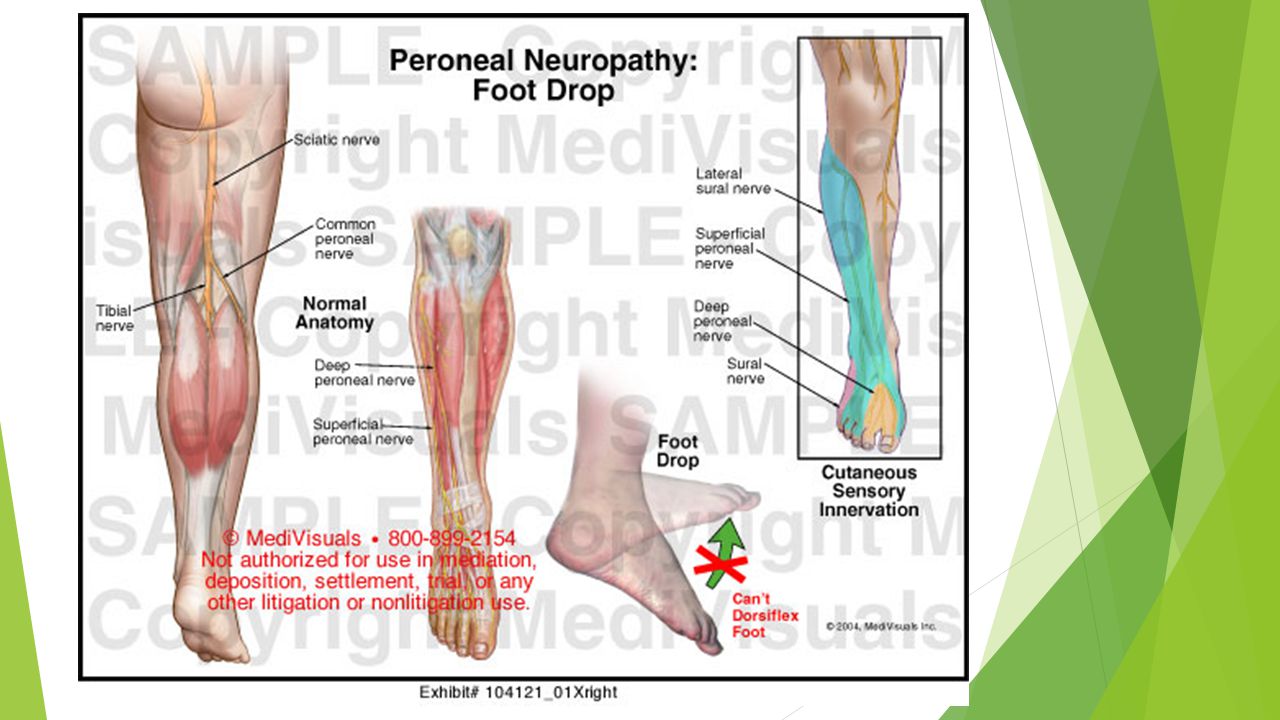
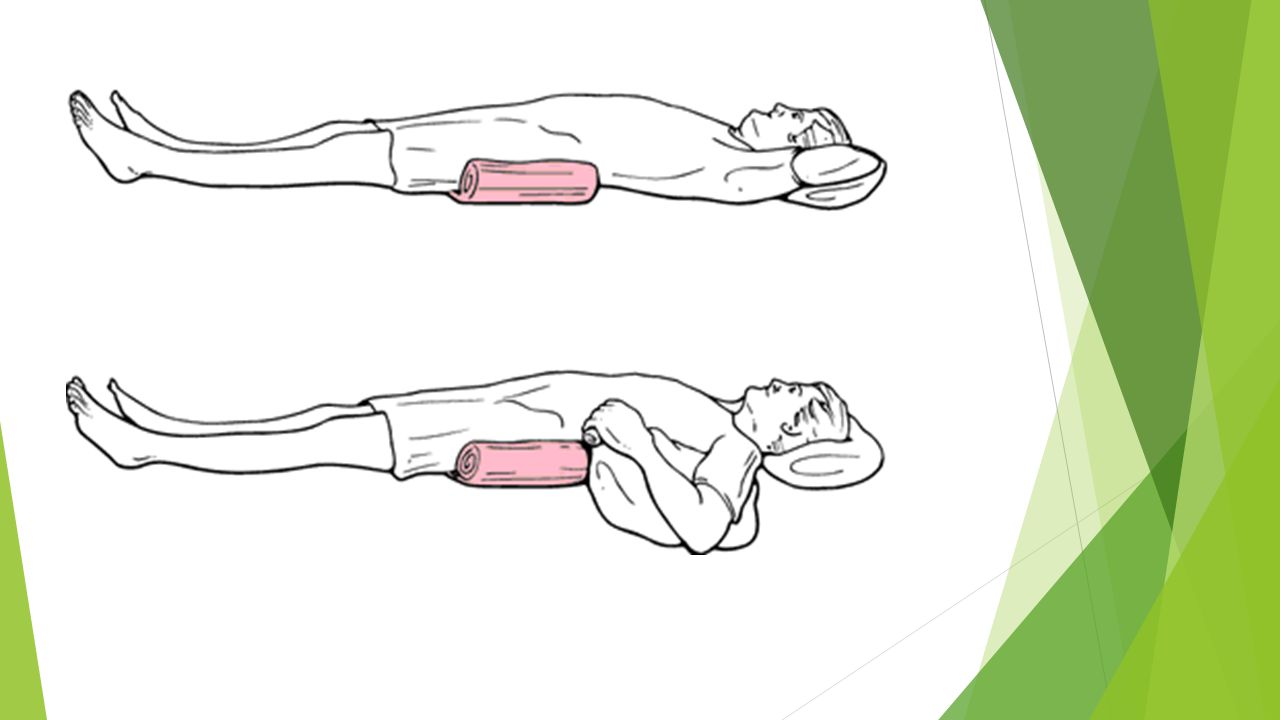
پیشگیری از چرخش مفصل ران به خارج
توسط یک تروکانتر رول با استفاده از یک ملافه لوله کرده از خار ایلیوم تا وسط استخوان ران پیشگیری از افتادگی پا(خم شدن به طرف کف پا) دلایل: صدمه عصب پرونئال جمع شدگی عضلات ساق پا( گاسترونیموس و سولئوس) فقدان حالت ارتجاعی تاندون آشیل با بالش یا آتل کف پا نسبت به ساق در یک حالت قائمه قرار گیرد. تمرینات ورزشی مچ پا
 دلایل: صدمه عصب پرونئال. جمع شدگی عضلات ساق پا( گاسترونیموس و سولئوس) فقدان حالت ارتجاعی تاندون آشیل. با بالش یا آتل کف پا نسبت به ساق در یک حالت قائمه قرار گیرد. تمرینات ورزشی مچ پا.")
11
حفظ کشش و قدرت عضله و تحرک مفصل
انجام ورزشهای دامنه حرکتی مفصل به صورت پاسیو یا اکتیو هر یک از مفاصل حداقل روزی 2 بار و هر بار 3 مرتبه باید در دامنه حرکتی آن مفصل ورزش داده شود انجام ورزشهای درمانی تشویق به تحریک مستقل کمک به انتقال و جابجایی بیمار آمادگی برای راه افتادن راه رفتن با چوب زیر بغل استفاد ه از واکر استفاده از عصا کمک به بیمار دارای ارتوز

13
فرایند پرستاری در بیمار دچار اختلالات پوستی
بررسی: بی حرکتی اختلالات ادراکی حسی یا شناختی کاهش خونرسانی بافتی کاهش وضعیت تغذیه ایی اصطکاک و نیروی برشی افزایش رطوبت

14
Pressure Ulcers Definition
Pressure Ulcers are localized areas of tissue necrosis that tend to occur when soft tissue is compressed between a bony prominence and an external surface for a prolonged period. These lesions are also called bedsores, decubitus ulcers and pressure sores زخم فشاری بر اثر نکروز منطقه محدودی ازبافت نرم که در اثر وارد آمدن فشار بالاتر از فشار عادی برای باز ماندن مویرگ ها (32 میلی متر جیوه ).
.")
15
THE 4 FORCES 1. Pressure: Force applied to soft tissue between hard surface and bony prominence. When skin and the underlying tissues are trapped between bone and a surface such as a wheelchair or bed, blood flow is restricted. This deprives tissue of oxygen and other nutrients -> tissue death. 2. Friction: Resistance of one body sliding or rolling over another. Making skin more susceptible to pressure sores.

16
PRESSURE AND FRICTION

18
3. Shear: This occurs when skin moves in one direction, and the underlying bone moves in another. Sliding down in a bed or chair or raising the head of bed more than 30 degrees is especially likely to cause shearing, which stretches and tears cell walls and tiny blood vessels. Especially affected are areas such as tailbone where skin is already thin and fragile. 4. Strain: Tissue deformation in response to pressure

19
Risk Factors Spinal cord injuries Traumatic brain injury
Neuromuscular disorders Immobility Malnutrition Fecal and urinary incontinence Altered level of consciousness Chronic systemic illness Fractures Aging skin decreased epidermal turnover dermoepidermal junction flattens fewer blood vessels Decreased pain perception

20
Site Pressure ulcers commonly occur over the : Sacrum
Greater trochanter Ischial tuberosity Malleolus Heel Fibular head Scapula

22
Stages/ classification

23
Classification Stage I 1. most superficial,
2. non blanchable redness, does not subside after pressure is relieved. 3. The skin may be hotter or cooler than normal 4. have an odd texture, or 5. perhaps be painful to the patient.

24
STAGE I

25
Stage II is damage to the epidermis extending into, but no deeper than, the dermis. In this stage, the ulcer may be referred to as a blister or abrasion. The ulcer is superficial and manifest clinically as an abrasion, blister or shallow crater

26
STAGE II

27
STAGE II

28
Stage III involves the full thickness of the skin and may extend into the subcutaneous tissue layer. This layer has a relatively poor blood supply and can be difficult to heal. The ulcer manifests clinically as a deep crater with or without undermining of adjacent tissue

29
STAGE III

30
STAGE III

31
Stage IV is the deepest, extending into the muscle, tendon or even bone.
“Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and/or tunneling” Depth varies according to anatomic location Exposed bone/tendon usually directly visible and/or palpable

32
STAGE IV

33
Stage 4 A B

34
STAGE IV

35
Complications Cellulitis. This causes pain, redness and swelling, all of which can be severe. Cellulitis can also lead to life-threatening complications, including sepsis and meningitis. Bone and joint infections. These develop when the infection from a bedsore burrows deep into joints and bones. Joint infections (septic or infectious arthritis) can damage cartilage and tissue, whereas bone infections (osteomyelitis) may reduce the function of joints and limbs.
 can damage cartilage and tissue, whereas bone infections (osteomyelitis) may reduce the function of joints and limbs.")
36
Sepsis. It occurs when bacteria enters bloodstream through the broken skin and spreads throughout the body — a rapidly progressing, life-threatening condition that can cause shock and organ failure. Cancer. This is usually an aggressive carcinoma affecting the skin's squamous cells.

37
Treatments and drugs Treating bedsores is challenging. Open wounds are slow to heal, and because skin and other tissues have already been damaged or destroyed, healing is never perfect. Requires a multidisciplinary approach – nurses, physician, social worker, physical therapist, urologist or gastroenterologist, a neurosurgeon, orthopedic surgeon and plastic surgeon.

38
TREATMENT OBJECTIVES Identification of problem
Debridement of necrotic tissue Moist wound care without maceration Control of infection/bioburden Management of pain Pressure redistribution/Offloading Choice of wound care products is individual preference as long as above objectives met.

39
1. Changing positions often
1. Changing positions often. Carefully follow the schedule for turning and repositioning — approximately every 15 minutes if in a wheelchair and at least once every two hours when in bed. If unable to change position on own, a family member or other caregiver must be able to help. 2. Using support surfaces. These are special cushions, pads, mattresses and beds that relieve pressure on an existing sore and help protect vulnerable areas from further breakdown.

40
PRESSURE REDISTRIBUTION

41
3. Cleaning. It's essential to keep wounds clean to prevent infection
3. Cleaning. It's essential to keep wounds clean to prevent infection. A stage I wound can be gently washed with water and mild soap, but open sores should be cleaned with a saltwater (saline) solution each time the dressing is changed. Avoid antiseptics such as hydrogen peroxide and iodine, which can damage sensitive tissue and delay healing. 4. Controlling incontinence as far as possible is crucial to helping sores
 solution each time the dressing is changed. Avoid antiseptics such as hydrogen peroxide and iodine, which can damage sensitive tissue and delay healing. 4. Controlling incontinence as far as possible is crucial to helping sores.")
42
5. Removal of damaged tissue (debridement)
5. Removal of damaged tissue (debridement). To heal properly, wounds need to be free of damaged, dead or infected tissue. This can be accomplished in several ways - a. Autolytic debridement is autolysis with the body's own enzymes. b. Biological debridement, or maggot debridement therapy, c. Chemical debridement, or enzymatic debridement d. Mechanical debridement e. Sharp debridement is the removal of necrotic tissue with a scalpel or similar instrument. f. Surgical debridement g. Ultrasound-assisted wound therapy
. To heal properly, wounds need to be free of damaged, dead or infected tissue. This can be accomplished in several ways - a. Autolytic debridement is autolysis with the body s own enzymes. b. Biological debridement, or maggot debridement therapy, c. Chemical debridement, or enzymatic debridement. d. Mechanical debridement. e. Sharp debridement is the removal of necrotic tissue with a scalpel or similar instrument. f. Surgical debridement. g. Ultrasound-assisted wound therapy.")
43
6. Dressings. 7. Oral antibiotics. 8. Healthy diet. 9. Muscle spasm relief 10. Educating the caregiver

44
B) Surgical repair by - tissue flap, free flap, Negative Pressure Wound Therapy
C) Other treatment options Researchers are searching for more effective bedsore treatments. Under investigation are hyperbaric oxygen, electrotherapy and the topical use of human growth factors.
 Other treatment options Researchers are searching for more effective bedsore treatments. Under investigation are hyperbaric oxygen, electrotherapy and the topical use of human growth factors.")
45
Prevention Bedsores are easier to prevent than to treat, but that doesn't mean the process is easy or uncomplicated. Although wounds can develop in spite of the most scrupulous care, it's possible to prevent them in many cases.

46
Position changes Changing position frequently and consistently is crucial to preventing bedsores. Experts advise shifting position about every 15 minutes that you're in a wheelchair and at least once every two hours, even during the night, if you spend most of your time in bed. Skin inspection Daily skin inspections for pressure sores are an integral part of prevention.

47
Nutrition A healthy diet is important in preventing skin breakdown and in aiding wound healing
Lifestyle changes – -Quitting smoking, - Exercise - Daily exercise improves circulation

48
Nursing Care of Bed Sores

49
Nursing Care of Bed Sores

50
Mobility & Immobility

51
Range of Motion Exercises

52
Flexion of the head and neck
Extension of the head and neck Rotation of neck. Lateral flexion of the head and neck

53
Extension of the shoulder
Flexion of the shoulder Abduction of the shoulder Adduction of the shoulder

54
Flexion and extension of the elbow
Internal and external rotation of the shoulder Extension of the finger Flexion of the finger

55
Adduction of the finger
Abduction of the finger Flexion and extension of the hip

56
Abduction of the hip Adduction of the hip External rotation of the hip Internal rotation of the hip

57
Flexion of the knee Extension of the knee Dorsiflexion of the ankle Plantar flexion of the ankle

58
Inversion of the ankle Eversion of the ankle Flexion of the toes Extension of the toes

59
Adduction of the toes Abduction of the toes

60
فرایند پرستاری در بیمار مبتلا به اختلال الگوی دفعی
بررسی تشخیص پرستاری اختلال دفع مدفوع اختلال دفع ادرار اهداف برنامه ریزی مداخلات

61
عوامل مختل کننده الگوی دفع
کاهش ظرفیت مثانه کاهش تون عضلانی افزایش حجم باقیمانده ادرار تاخیر در احساس علایم مربوط به دفع مصرف داروهای مختل کننده الگوی دفع مثل مدرها(افزایش حجم ادرار) آرابخشها (مختل کننده حساسیت مثانه به نشانه های دفع) و داروهای آنتی کولینرژیک یا آدرنرژیک (احتباس ادرار) بی حرکتی عملکردی عدم تحمل فعالیت
 آرابخشها (مختل کننده حساسیت مثانه به نشانه های دفع) و داروهای آنتی کولینرژیک یا آدرنرژیک (احتباس ادرار) بی حرکتی عملکردی. عدم تحمل فعالیت.")
62
برنامه تعین شده جهت مصرف مایعات (30 دقیقه قبل از دفع نوشیدن مایعات)
بیوفیدبک: آموزش آگاهانه انقباض اسفنکترها ورزش عضلات کف لگن(کگل):10 بار هر بار 4 ثانیه به صورت 4 تا 6 بار در روز ضربه زدن آهسته قسمت داخلی لگن و بالای عانه سوندگذاری متناوب
:10 بار هر بار 4 ثانیه به صورت 4 تا 6 بار در روز. ضربه زدن آهسته قسمت داخلی لگن و بالای عانه. سوندگذاری متناوب.")
63
افزایش کنترل مدفوع برنامه مشخص برای کنترل دفع
رفلکس های گاستروکولیک و دئودنوکولیک فعال کردن بازتاب آنورکتال با شیاف و به صورت مکانیکی (توشه رکتال) وضعیت چمپاته زدن
 وضعیت چمپاته زدن.")
Similar presentations









 Presented by: Nirvi Shah.>")










 A pressure ulcer is localized injury to the skin and/or underlying.>")


