Download presentation
Presentation is loading. Please wait.

1
General principles of fractures III

2
Hold reduction The word 'immobilization' has been avoided because the objective is seldom complete immobility usually it is the prevention of displacement. Nevertheless, some restriction of movement is needed to promote soft tissue healing and to allow free movement of the unaffected parts.

3
The available methods of holding reduction are:
(1) Continuous traction. (2) Cast splintage. (3) Functional bracing. (4) Internal fixation. (5) External fixation. Note: the objective is to splint fracture, not entire limb.
 Continuous traction. (2) Cast splintage. (3) Functional bracing. (4) Internal fixation. (5) External fixation. Note: the objective is to splint fracture, not entire limb.")
4
CONTINUOUS TRACTION Traction is applied to the limb distal to the fracture, so as to exert a continuous pull in the long axis of the bone. This is particularly useful for shaft fractures which are oblique or spiral and easily displaced by muscle contraction. Maintain accurate reduction is by traction is difficult, but the patient can move his joints and exercise his muscles.

5
CONTINUOUS TRACTION So the by traction can Hold. Move. Safe
The weak point is the speed, healing take long time which keep patient in bed and hospital for long time. As soon as the fracture become sticky (deformable but not displaceable)'traction should be replaced by bracing.
 traction should be replaced by bracing.")
6
CONTINUOUS TRACTION Types of tractions:
Traction by gravity: this is applied to the upper limb fractures; with a wrist sling the weight of the arm provides continuous traction to the humerus injuries.

9
CONTINUOUS TRACTION 2. Skin traction: this traction will sustain a pull of no more than 5 Kg. it composed of adhesive plaster augmented by bandage. The malleoli are protected by sponge, and cords or tapes are used for traction.

13
CONTINUOUS TRACTION Indications
If the traction weight needed less than 5 kg. Children. If the traction used as a method of reduction only. Osteoporotic bone.

14
CONTINUOUS TRACTION Advantages Easy. Safe. Anybody can apply it.
Less complications

15
CONTINUOUS TRACTION Complications Compartmental syndrome.
Peroneal nerve injury and foot drop.

16
CONTINUOUS TRACTION 3.Skeletal traction: A Kirschner wire, Steinmann pin or Denham pin is inserted, usually in the distal femur or behind the tibial tubercle for hip, thigh and knee injuries, lower in the tibia or through the calcaneum for tibial fractures.

17
CONTINUOUS TRACTION Indications
When traction weight needed more than 5 kg. Traction weight calculated as 1/10 of the body weight. When traction used as mean of reduction and holding.

22
Advantages Can use weight more than 5 kg. Complications Neurovascular injury. Fracture. Osteomyelitis.

23
CAST SPLINTAGE P.O.P (Plaster Of Paris) is the widely used splint. It is partially hydrated calcium sulphate when put in water it will change to fully hydrated calcium sulphate and when it apply on the limb the water will evaporated and the end result is sold anhydrate calcium sulphate.
 is the widely used splint. It is partially hydrated calcium sulphate when put in water it will change to fully hydrated calcium sulphate and when it apply on the limb the water will evaporated and the end result is sold anhydrate calcium sulphate.")
24
CAST SPLINTAGE Types Partial or slab which is either anterior or posterior. Complete cast .

29
CAST SPLINTAGE Cast is Safe. Speed is good less hospital stay. Hold.
The weak point is the move because splintage should involve joint above and below, so movement is impossible and risk of joint stiffness is increased.

30
CAST SPLINTAGE Complications Tight cast
The cast may put too tight or it becomes tight when the limb swells. The patient complains of diffuse pain and later sign of vascular compression appear. The limb should be elevated, but if the pain persists the only safe course is to split the cast and ease it open. For that reason partial cast should be applied to fresh fractures.

31
CAST SPLINTAGE 2. Pressure sores Even a well-fitting cast may press upon the skin over a bony prominence (the patella, the heel the elbow or the head of the ulna). The patient complains of localized pain over the pressure spot such localized pain demands immediate inspection through a window in the cast. 3. Skin abrasion and laceration
. The patient complains of localized pain over the pressure spot such localized pain demands immediate inspection through a window in the cast. 3. Skin abrasion and laceration.")
32
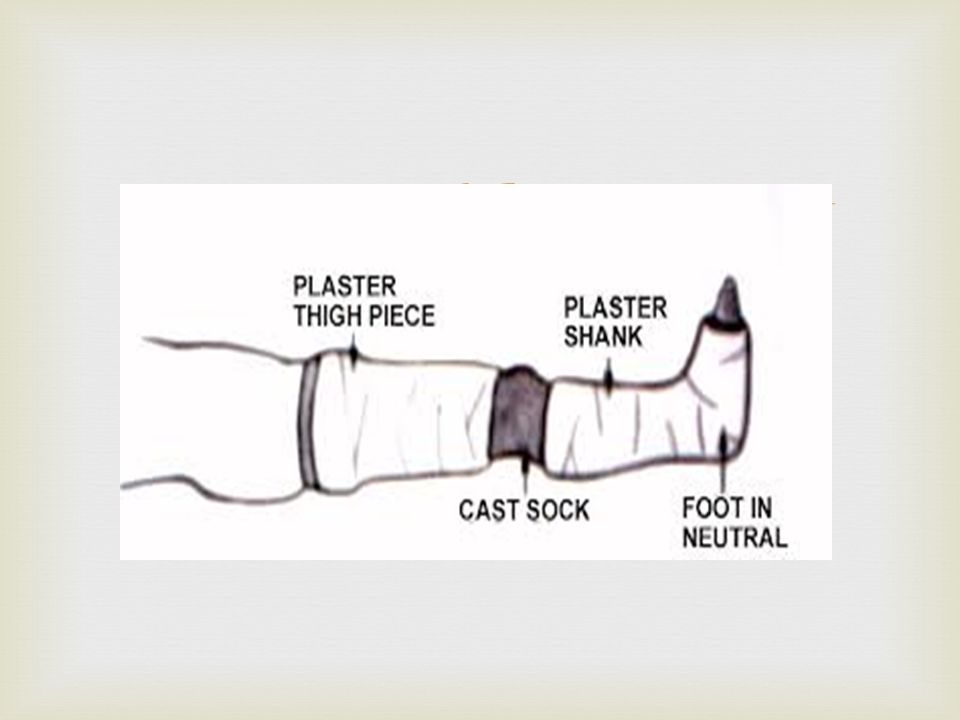
FUNCTIONAL BRACING Functional bracing, using either plaster of paris or one of the lighter materials, is one way of preventing joint stiffness while still permitting fracture splintage and loading. Segments of a cast are applied only over the shafts of the bones, leaving the joints free; the cast segments are connected by metal or plastic hinges which allow movements in one plane.

33
FUNCTIONAL BRACING The splints are 'functional' in that joint movements are much less restricted than with conventional casts. Functional bracing is used most widely for fractures of the femur or tibia. But since the brace is not very rigid, it is usually applied only when the fracture is beginning to unite, i.e. after 3-6 weeks of traction or conventional plaster.

34
FUNCTIONAL BRACING It provide Safety. Movement. Speed.
The weak point is not rigid so it cannot used as primary treatment

39
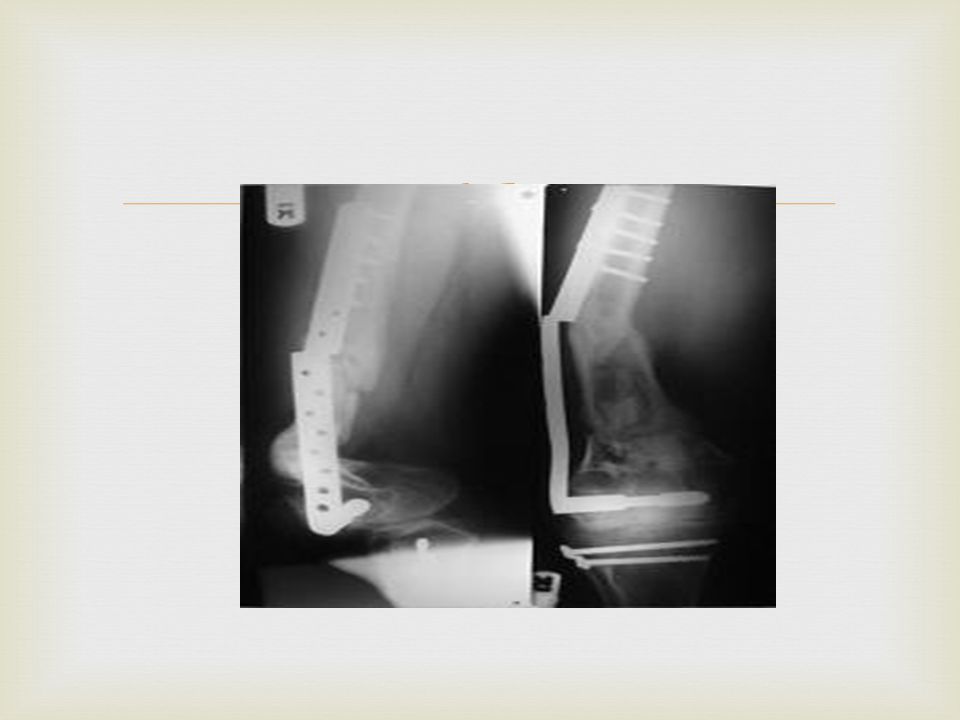
INTERNAL FIXATION Bone fragments may be fixed with Screws.
Transfixing pins or nails. Metal plate held by screws. Long intramedullary nail (with or without locking screws) Circumferential bands. Combination of these methods.
 Circumferential bands. Combination of these methods.")
47
INTERNAL FIXATION Internal fixation provides Rigid hold.
Free joint movement. Speed, patient early leaves the hospital. The weak point is risk of infection and neurovascular injury because it is invasive so it is not safe.

48
INTERNAL FIXATION The risk of infection depends upon:
(1) The patient - devitalized tissues, a dirty wound and an unfit patient are all dangerous. (2) The surgeon – experience how to deal with tissues. (3) The facilities - a guaranteed aseptic routine.
 The patient - devitalized tissues, a dirty wound and an unfit patient are all dangerous. (2) The surgeon – experience how to deal with tissues. (3) The facilities - a guaranteed aseptic routine.")
49
INTERNAL FIXATION Indications
Internal fixation is often the most desirable form of treatment. The chief indications are: Fractures that cannot be reduced except by operation. Unstable fractures and prone to redisplacement after reduction e.g. mid-shaft fractures of the forearm and displaced ankle fractures); also, those liable to be pulled apart by muscle action (e.g. transverse fracture of the patella or olecranon). Fractures that unite poorly and slowly, e.g. fractures of the femoral neck.
; also, those liable to be pulled apart by muscle action (e.g. transverse fracture of the patella or olecranon). Fractures that unite poorly and slowly, e.g. fractures of the femoral neck.")
50
INTERNAL FIXATION 4) Pathological fractures, in which bone disease may prevent healing. 5) Multiple fractures, where early fixation (by either internal or external fi-ration) reduces the risk of general complications and late multisystem organ failure. 6) Intraarticular fractures. 7) Fractures in patient who present nursing difficulties (paraplegics, those with multiple injuries and very elderly).
 Multiple fractures, where early fixation (by either internal or external fi-ration) reduces the risk of general complications and late multisystem organ failure. 6) Intraarticular fractures. 7) Fractures in patient who present nursing difficulties (paraplegics, those with multiple injuries and very elderly).")
51
INTERNAL FIXATION Complications Infection. Non-union. Implant failure.
Refracture.

57
EXTERNAL FIXATION A fracture may be held by transfixing screws or tensioned wires which pass through the bone above and below the fracture and are attached to an external frame.

63
EXTERNAL FIXATION Indications
1. Fractures associated with severe soft tissue damage where the wound can be left open for inspection, dressing or skin grafting (open fractures). 2. Fractures associated with nerve or vessel damage. 3. Severely comminuted and unstable fractures, which can be held out to length until healing. 4. Ununited fractures, which can be excised and compressed; sometimes this is combined with elongation.
. 2. Fractures associated with nerve or vessel damage. 3. Severely comminuted and unstable fractures, which can be held out to length until healing. 4. Ununited fractures, which can be excised and compressed; sometimes this is combined with elongation.")
64
EXTERNAL FIXATION 5. Fractures of the pelvis, which often cannot be controlled by any other method. 6. Infected fractures, for which internal fixation not suitable. 7. Severe multiple injuries, where early stabilization reduces the risk of serious complications.

65
EXTERNAL FIXATION The main complications of external fixation are:
(1) Over distraction of the fragments, which are then held rigidly apart. (2) Reduced load transmission through the bone, which delays fracture healing and causes osteoporosis. (For this reason, external fixators should be dynamized or removed after 6-8 weeks. and replaced by some alternative form of splintage which will allow bone loading). (3) Pin-track infection. (4) Neurovascular injuries.
 Over distraction of the fragments, which are then held rigidly apart. (2) Reduced load transmission through the bone, which delays fracture healing and causes osteoporosis. (For this reason, external fixators should be dynamized or removed after 6-8 weeks. and replaced by some alternative form of splintage which will allow bone loading). (3) Pin-track infection. (4) Neurovascular injuries.")
Similar presentations







































Extension of traumatized wound to allow identification of zone of injury 2)Detection & removal of foreign material, especially.>")


![Thigh and knee. CLASSIFICATION FRACTURES OF THE FEMUR [1 ]Fracture of the neck of the femur, and [2]Fracture of the trochanteric region [3] Fracture of.](/14/4311083/big_thumb.jpg "Thigh and knee. CLASSIFICATION FRACTURES OF THE FEMUR [1 ]Fracture of the neck of the femur, and [2]Fracture of the trochanteric region [3] Fracture of.>")









 guidelines with attention.>")
