Download presentation
Presentation is loading. Please wait.

1
Head, Facial, & Neck Trauma

2
Sections Introduction to Head, Facial, & Neck Injuries
Anatomy and Physiology of the Head, Face, & Neck Pathophysiology of Head, Facial, & Neck Injury Assessment and Management of Head, Facial, & Neck Injuries Head, Facial, & Neck Injury Management

3
Introduction to Head, Facial, & Neck Injuries
Common major trauma 4 million people experience head trauma annually Severe head injury is most frequent cause of trauma death GSW to cranium: % mortality At Risk population Males 15-24 Infants Young Children Elderly

4
Introduction to Head, Facial, & Neck Injuries
Injury Prevention Programs Motorcycle Safety Bicycle Safety Helmet & Head Injury Awareness Programs Other Sports Football Rollerblading Contact Sports

5
Introduction to Head, Facial, & Neck Injuries
TIME IS CRITICAL Intracranial Hemorrhage Progressing Edema Increased ICP Cerebral Hypoxia Permanent Damage Severity is difficult to recognize Subtle signs Improve differential diagnosis Improves survivability

6
Anatomy & Physiology Head, Face & Neck
Anatomy & Physiology of the Head Scalp Cranium Meninges Cerebrospinal Fluid Brain CNS Circulation Blood-Brain Barrier Cerebral Perfusion Pressure Cranial Nerves Ascending Reticular Activating System

7
Anatomy & Physiology of the Head
Scalp Strong Flexible mass of Skin Fascia Muscular Tissue Highly Vascular Hair provides Insulation Structures Beneath Galea Aponeurotica Between scalp and skull Fibrous connective sheath Subaponeurotica (Areolar) Tissue Permits venous blood flow from the dural sinuses to the venous vessels of scalp Emissary Veins: Potential route for Infection
 Tissue. Permits venous blood flow from the dural sinuses to the venous vessels of scalp. Emissary Veins: Potential route for Infection.")
8
Anatomy & Physiology of the Head
Recalling Structures of the Scalp S - skin C - connective tissue A - aponeurotica L - layer of areolar tissue P - periosteum of skull

9
Anatomy & Physiology of the Head
Skull comprised of Facial bones Cranium Vault for the brain Strong, light, rigid, spherical bone Unyielding to increased intracranial pressure (ICP) Bones Frontal Parietal Occipital Temporal Ethmoid Sphenoid
 Bones. Frontal. Parietal. Occipital. Temporal. Ethmoid. Sphenoid.")
10
Cranium Parietal Sphenoid Suture Line Frontal Temporal Orbits Maxillae
Mandible Temporal Mandibular Joint Nasal Bones Foramen Magnum (Hole in Base) Occiptal Zygomatic Arch
 Occiptal. Zygomatic Arch.")
12
Anatomy & Physiology of the Head
Skull Other Structures Foramen Magnum Largest opening of the skull Spinal cord exits Cribriform Plate Inferior aspect (Base) Rough surface Brain can be easily injured Abrade Contusion Laceration
 Rough surface. Brain can be easily injured. Abrade. Contusion. Laceration.")
13
Anatomy & Physiology of the Head
Meninges Protective mechanism for the CNS Dura Mater Layers Outer: Cranium’s inner periosteum Inner: Dural Layer Between: Dural Sinuses: Venous drains for brain Provides continuous connective tissue Forms partial structural divisions Falx cerebri Tentorium cerebelli Large arteries above Provide blood flow to the surface of the brain

14
Anatomy & Physiology of the Head
Meninges Pia Mater Closest to brain and spinal cord Delicate tissue Covers all areas of brain and spinal cord Very Vascular Supply superficial areas of brain Arachnoid Membrane “Spider-like” Covers inner dura Suspends brain in cranial cavity Collagen & Elastin fibers Subarachnoid Space beneath CSF Cushions brain

16
Anatomy & Physiology of the Head
Cerebrospinal Fluid Clear, colorless fluid Comprised of Water Protein Salts Cushions CNS Made in largest two ventricles of brain Medium for nutrients and waste products to diffuse into and out of brain

17
Anatomy & Physiology of the Head
Brain Occupies 80% of cranium Comprised of 3 Major Structures Cerebrum Cerebellum Brainstem High metabolic rate Receives 15% of cardiac output Consumes 20% of body’s oxygen Requires constant circulation IF Blood supply stops Unconscious within 10 seconds Death in 4-6 minutes

18
Anatomy & Physiology of the Head
Cerebrum Function Center of conscious thought, personality, speech, and motor control Visual, auditory, and tactile perception Lobes Frontal Personality Parietal Motor & Sensory Activity Memory & Emotion (continued)
")
19
Anatomy & Physiology of the Head
Occipital Sight Temporal Long-term memory Hearing, Speech, Taste & Smell

20
Anatomy & Physiology of the Head
Cerebrum Falx Cerebri Divides cerebrum into right and left hemispheres Central Sulcus Fissure splits cerebrum into right and left hemispheres Each hemisphere controls the opposite side of the body Tentorium Fibrous sheet within occipital region Brainstem perforates thru incisura tentorri cerebelli Occulomotor Nerve (CN-III) travels along Controls pupil size Compression results in pupillary disturbances
 travels along. Controls pupil size. Compression results in pupillary disturbances.")
22
Anatomy & Physiology of the Head
Cerebrum Hemisphere Functions Left: DOMINANT Mathematical computations: Occipital Writing: Parietal Language interpretation: Occipital Speech: Frontal Right: NON-DOMINANT Non-verbal imagery

23
Anatomy & Physiology of the Head
Cerebellum Located under tentorium Function “Fine tunes” motor control Allows smooth movement Balance Maintenance of muscle tone

24
Anatomy & Physiology of the Head
Brainstem Central processing center Communication junction among Cerebrum Spinal cord Cranial nerves Cerebellum Structures Midbrain Pons Medulla Oblongata

25
Anatomy & Physiology of the Head
Midbrain Upper portion of brainstem Structures Hypothalamus Endocrine function, vomiting reflex, hunger, thirst Kidney function, body temperature, emotion Thalamus Switching center between pons & cerebrum Critical Element in Ascending Reticular Activating System (A-RAS) ESTABLISHES CONSCIOUSNESS Major pathways for optic & olfactory nerves Associated Structures
 ESTABLISHES CONSCIOUSNESS. Major pathways for optic & olfactory nerves. Associated Structures.")
26
Anatomy & Physiology of the Head
Pons Communication interchange between cerebellum, cerebrum, midbrain, and spinal cord Bulb shaped structure above medulla Sleeping phase of the RAS

27
Anatomy & Physiology of the Head
Medulla Oblongata Bulge in the top of the spinal cord Centers Respiratory Center Controls depth, rate and rhythm Cardiac Center Regulates rate and strength of cardiac contractions Vasomotor Center Distribution of blood Maintains blood pressure

28
Anatomy & Physiology of the Head
CNS Circulation Arterial Four Major Arteries 2 Internal Carotid Arteries From the common carotid 2 Vertebral Arteries Circle of Willis Internal Carotids and Vertebral Arteries Encircle the base of the brain Venous Venous drainage occurs through bridging veins Bridge Dural Sinuses Drain into internal jugular veins

29
Anatomy & Physiology of the Head
Blood-Brain Barrier Less permeable than elsewhere in body DO NOT allow flow of interstitial proteins Reduced lymphatic flow Very protected environment Blood acts as irritant resulting in cerebral edema

30
Anatomy & Physiology of the Head
Cerebral Perfusion Pressure Pressure within cranium (ICP) resists blood flow and good perfusion to the CNS Pressure usually less than 10 mmHg Mean Arterial Pressure (MAP) Must be at least 50 mmHg to ensure adequate perfusion MAP = DBP + 1/3 Pulse Pressure Cerebral Perfusion Pressure (CPP) Pressure moving blood through the cranium CPP = MAP - ICP
 resists blood flow and good perfusion to the CNS. Pressure usually less than 10 mmHg. Mean Arterial Pressure (MAP) Must be at least 50 mmHg to ensure adequate perfusion. MAP = DBP + 1/3 Pulse Pressure. Cerebral Perfusion Pressure (CPP) Pressure moving blood through the cranium. CPP = MAP - ICP.")
31
Anatomy & Physiology of the Head
Calculating MAP Calculating CPP

32
Anatomy & Physiology of the Head
Cerebral Perfusion Pressure Autoregulation Changes in ICP result in compensation Increased ICP = Increased BP This causes ICP to rise higher and BP to rise Brain injury and death become imminent Expanding mass inside cranial vault Displaces CSF If pressure increases, brain tissue is displaced

33
Anatomy & Physiology of the Head
Cranial Nerves 12 pair with distinct pathways Senses, facial innervation, & body function control Ascending Reticular Activation System Tract of neurons in upper brainstem, pons, and midbrain Responsible for sleep-wake cycle Monitors input stimulation Regulates body functions Respiration Heart Rate Peripheral Vascular Resistance Injury may result in prolonged waking state

35
M S II III V VI X XII XI VIII IV VII IX I
Face Muscles M Chewing muscles Posterior palate and pharynx Sight S Optic II Pupil Const, Rectus & Obliques Oculomotor III Opthalmic (FH), Maxillary (cheek) Mandible (chin) Trigeminal V Lateral rectus muscle Abducens VI Taste to posterior tongue Vagus X Tongue Hypoglossal XII Trapezius & Sternocleido. Muscles Accessory XI Hearing balance Acoustic VIII Superior Obliques Trochlear IV Facial VII Posterior pharynx, taste to anterior tongue Glossopharyn- geal IX Smell Olfactory I Innervation F Name CN
, Maxillary (cheek) Mandible (chin) Trigeminal. V. Lateral rectus muscle. Abducens. VI. Taste to posterior tongue. Vagus. X. Tongue. Hypoglossal. XII. Trapezius & Sternocleido. Muscles. Accessory. XI. Hearing balance. Acoustic. VIII. Superior Obliques. Trochlear. IV. Facial. VII. Posterior pharynx, taste to anterior tongue. Glossopharyn- geal. IX. Smell. Olfactory. I. Innervation. F. Name. CN.")
36
Anatomy & Physiology Head, Face & Neck
Anatomy & Physiology of the Face Structure Ear Eye

37
Anatomy & Physiology of the Face
Structure Facial Bones Zygoma Prominent bone of the cheek Protects eyes Attachment for muscles controlling eye & jaw movement Maxilla Upper jaw Supports the nasal bone Provides lower border of orbit Mandible Jaw bone Nasal Bones

39
Anatomy & Physiology of the Face
Structure Covered with skin Flexible and thin Highly vascular Minimal layer of subcutaneous tissue Circulation External carotid artery Supplies facial area Branches Facial, Temporal & Maxillary Arteries

40
Anatomy & Physiology of the Face
Nerves Trigeminal (CN-V) Facial Sensation Some eye motor control Enables chewing process Facial (CN-VII) Motor control for facial muscles Sensation of taste
 Facial Sensation. Some eye motor control. Enables chewing process. Facial (CN-VII) Motor control for facial muscles. Sensation of taste.")
41
Anatomy & Physiology of the Face
Nasal Cavity Upper Border Bones Junction of Ethmoid, Nasal, & Maxillary Bones Bony Septum Right & Left Chamber Turbinates Vascular mucosa support Warm, Humidify, and Filter incoming air Lower Border Bony Hard Palate Soft Palate Moves upward during swallowing Nasal Cartilage Forms Nares

42
Anatomy & Physiology of the Face
Oral Cavity Formed Structures Maxillary bone Palate Upper teeth meeting the mandible and lower teeth Floor Tongue Connects to hyoid bone Free-floating U-shaped bone inferior & posterior of the mandible Mandible Articulates with the TMJ joint

43
Anatomy & Physiology of the Face
Special Structures Salivary Glands First stage in digestion Location Anterior and inferior to the ear Under tongue Inside the inferior mandible Tonsils Posterior wall of the pharynx (continued)
")
44
Anatomy & Physiology of the Face
Sinuses Hollow spaces in cranium and facial bones Function Lighten head Protect eyes and nasal cavity Produce resonant tones of voice Strengthen area against trauma

45
Anatomy & Physiology of the Face
Cranial Nerves CN-XII (Hypoglossal) Swallowing & tongue movement CN-IX (Glossopharyngeal) Saliva production & taste CN-V (Trigeminal) Sensations from facial region & aids in chewing CN-VII (Facial) Muscles of facial expression & taste
 Swallowing & tongue movement. CN-IX (Glossopharyngeal) Saliva production & taste. CN-V (Trigeminal) Sensations from facial region & aids in chewing. CN-VII (Facial) Muscles of facial expression & taste.")
46
Anatomy & Physiology of the Face
Pharynx Posterior & Inferior to the oral cavity Aids in swallowing Bolus of food propelled back & down by tongue Epiglottis moves downward Larynx moves up Combined effect seals airway Peristaltic wave moves food down esophagus

47
Anatomy & Physiology of the Face
Ear Function Hearing Positional sense Structures Pinna Outer visible portion Formed of Cartilage & has Poor blood supply External Auditory Canal Glands that secrete cerumen (wax) Middle & Inner Ear Structures for hearing and positional sense
 Middle & Inner Ear. Structures for hearing and positional sense.")
49
Anatomy & Physiology of the Face
Ear Structures for Hearing Tympanic membrane Ossicle bones Cochlea Auditory Nerve Structures for Proprioception Semicircular canals Sense position & motion Present when eyes are closed Vertigo Continuous movement sensation

50
Anatomy & Physiology of the Face
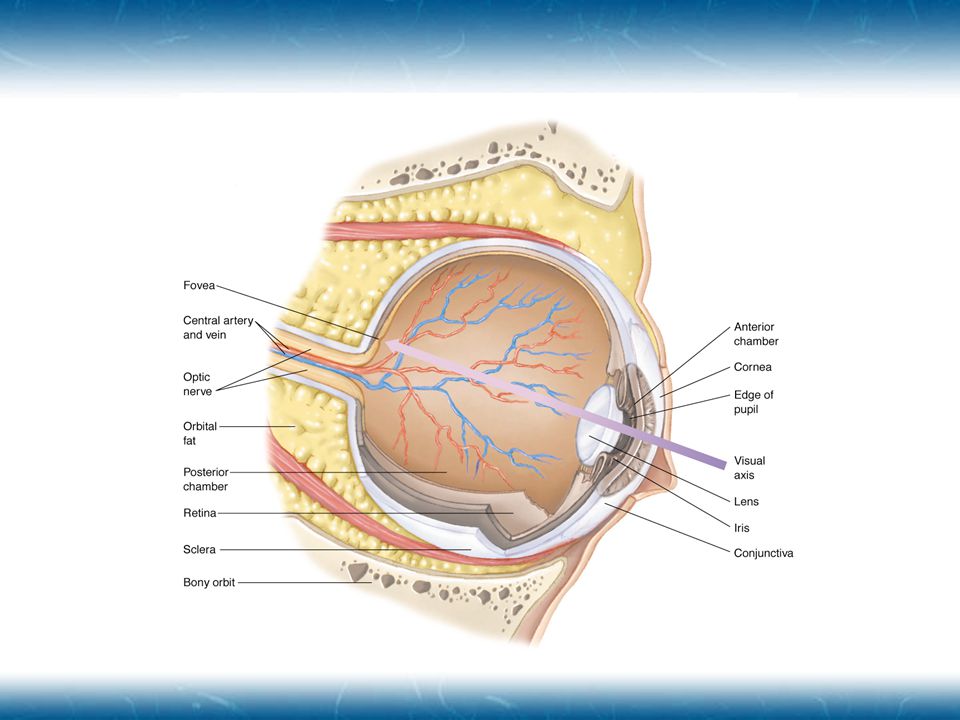
Eye Structures Sclera Cornea Conjunctiva Anterior Chamber Aqueous humor Iris Pupil Lens Posterior Chamber Vitreous humor Retina Lacrimal Fluid Bathes, protects, and nourishes cornea

52
Anatomy & Physiology of the Face
Eye Innervation CN-III (Oculomotor) Pupil dilation Conjugate movement Movement of eyes together Normal range of motion CN-IV (Trochlear) Downward & inward movement CN-VI (Abducens) Abduction (outward) gaze
 Pupil dilation. Conjugate movement. Movement of eyes together. Normal range of motion. CN-IV (Trochlear) Downward & inward movement. CN-VI (Abducens) Abduction (outward) gaze.")
53
Anatomy & Physiology of the Neck
Vasculature of the Neck Carotid Arteries Arise from RIGHT: Brachiocephalic Artery LEFT: Aorta Artery Split Internal & External Carotid Arteries Upper border of the Larynx Carotid Bodies & Sinuses located Bodies: Monitor CO2 and O2 levels Sinuses: Monitor Blood Pressure (continued)
")
54
Anatomy & Physiology of the Neck
Jugular Veins External Superficial, lateral to the trachea Internal Sheath with the carotid artery and vagus nerve

55
Anatomy & Physiology of the Neck
Airway Structures Larynx Epiglottis Thyroid & Cricoid Cartilage Trachea Posterior border is anterior border of esophagus

56
Anatomy & Physiology of the Neck
Other Structures Cervical Spine Musculoskeletal Function External Skeletal support of the head and neck Attachment point for spinal column ligaments Attachment point for tendons to move head and shoulders Nervous Function Spinal Cord contained within Peripheral Nerve Exit between vertebrae

57
Anatomy & Physiology of the Neck
Other Structures Esophagus Cranial Nerves CN-IX (Glossopharyngeal) Carotid Bodies & Carotid Sinuses CN-X Speech, swallowing, cardiac, respiratory & visceral function Thoracic Duct Delivers lymph to the venous system (continued)
 Carotid Bodies & Carotid Sinuses. CN-X. Speech, swallowing, cardiac, respiratory & visceral function. Thoracic Duct. Delivers lymph to the venous system. (continued)")
58
Anatomy & Physiology of the Neck
Glands Thyroid Rate of cellular metabolism Systemic levels of calcium Brachial Plexus Network of nerves in lower neck and should that control arm and hand function

59
Pathophysiology of Head, Facial, & Neck Injury
Mechanism of Injury Blunt Injury Motor vehicle collisions Assaults Falls Penetrating Injury Gunshot wounds Stabbing Explosions “Clothesline”

60
Scalp Injury Contusions Lacerations Avulsions Significant Hemorrhage
ALWAYS Reconsider MOI for severe underlying problems

61
Cranial Injury Trauma must be extreme to fracture Basal Skull Linear
Depressed Open Impaled Object Basal Skull Unprotected Spaces weaken structure Relatively easier to fracture

62
Cranial Injury Basal Skull Fracture Signs Battle’s Signs Raccoon Eyes
Retroauricular Ecchymosis Associated with fracture of auditory canal and lower areas of skull Raccoon Eyes Bilateral Periorbital Ecchymosis Associated with orbital fractures

63
Cranial Injury Basilar Skull Fracture May tear dura
Permit CSF to drain through an external passageway May mediate rise of ICP Evaluate for “Target” or “Halo” sign

64
Brain Injury As defined by the National Head Injury Foundation
“a traumatic insult to the brain capable of producing physical, intellectual, emotional, social and vocational changes.” Classification Direct Primary injury caused by forces of trauma Indirect Secondary injury caused by factors resulting from the primary injury

65
Direct Brain Injury Types
Coup Injury at site of impact Contrecoup Injury on opposite side from impact

66
Direct Brain Injury Categories
Focal Occur at a specific location in brain Differentials Cerebral Contusion Intracranial Hemorrhage Epidural hematoma Subdural hematoma Intracerebral Hemorrhage Diffuse Concussion Moderate Diffuse Axonal Injury Severe Diffuse Axonal Injury

67
Focal Brain Injury Cerebral Contusion
Blunt trauma to local brain tissue Capillary bleeding into brain tissue Common with blunt head trauma Confusion Neurologic deficit Personality changes Vision changes Speech changes Results from Coup-contrecoup injury

68
Focal Brain Injury Intracranial Hemorrhage
Epidural Hematoma Bleeding between dura mater and skull Involves arteries Middle meningeal artery most common Rapid bleeding & reduction of oxygen to tissues Herniates brain toward foramen magnum

69
Focal Brain Injury Intracranial Hemorrhage
Subdural Hematoma Bleeding within meninges Beneath dura mater & within subarachnoid space Above pia mater Slow bleeding Superior sagital sinus Signs progress over several days Slow deterioration of mentation

70
Focal Brain Injury Intracranial Hemorrhage
Intracerebral Hemorrhage Rupture blood vessel within the brain Presentation similar to stroke symptoms Signs and symptoms worsen over time

71
Diffuse Brain Injury Due to stretching forces placed on axons
Pathology distributed throughout brain Types Concussion Moderate Diffuse Axonal Injury Severe Diffuse Axonal Injury

72
Diffuse Brain Injury Concussion
Mild to moderate form of Diffuse Axonal Injury (DAI) Nerve dysfunction without anatomic damage Transient episode of Confusion, Disorientation, Event amnesia Suspect if patient has a momentary loss of consciousness Management Frequent reassessment of mentation ABC’s
 Nerve dysfunction without anatomic damage. Transient episode of. Confusion, Disorientation, Event amnesia. Suspect if patient has a momentary loss of consciousness. Management. Frequent reassessment of mentation. ABC’s.")
73
Diffuse Brain Injury Moderate Diffuse Axonal Injury
“Classic Concussion” Same mechanism as concussion Additional: Minute bruising of brain tissue Unconsciousness If cerebral cortex and RAS involved May exist with a basilar skull fracture Signs & Symptoms Unconsciousness or Persistent confusion Loss of concentration, disorientation Retrograde & Antegrade amnesia Visual and sensory disturbances Mood or Personality changes

74
Diffuse Brain Injury Severe Diffuse Axonal Injury
Brainstem Injury Significant mechanical disruption of axons Cerebral hemispheres and brainstem High mortality rate Signs & Symptoms Prolonged unconsciousness Cushing’s reflex Decorticate or Decerebrate posturing

75
Intracranial Perfusion
Review Cranial volume fixed 80% = Cerebrum, cerebellum & brainstem 12% = Blood vessels & blood 8% = CSF Increase in size of one component diminishes size of another Inability to adjust = increased ICP

76
Intracranial Perfusion
Compensating for Pressure Compress venous blood vessels Reduction in free CSF Pushed into spinal cord Decompensating for Pressure Increase in ICP Rise in systemic BP to perfuse brain Further increase of ICP Dangerous cycle ICP BP

77
Intracranial Pressure
Role of Carbon Dioxide Increase of CO2 in CSF Cerebral Vasodilation Encourage blood flow Reduce hypercarbia Reduce hypoxia Contributes to ICP Causes classic Hyperventilation & Hypertension Reduced levels of CO2 in CSF Cerebral vasoconstriction Results in cerebral anoxia

78
Factors Affecting ICP Vasculature Constriction Cerebral Edema
Systolic Blood Pressure Low BP = Poor Cerebral Perfusion High BP = Increased ICP Carbon Dioxide Reduced respiratory efficiency

80
Pressure & Structural Displacement
Increased pressure Compresses brain tissue Against & around Falx Cerebri Tentorium Cerebelli Herniates brainstem Compromises blood supply Signs & Symptoms Upper Brainstem Vomiting Altered mental status Pupillary dilation Medulla Oblongata Respiratory Cardiovascular Blood Pressure disturbances

81
Signs & Symptoms of Brain Injury
Altered Mental Status Altered orientation Alteration in personality Amnesia Retrograde Antegrade Cushing’s Reflex Increased BP Bradycardia Erratic respirations Vomiting Without nausea Projectile Body temperature changes Changes in pupil reactivity Decorticate posturing

82
Signs & Symptoms of Brain Injury
Pathophysiology of Changes Frontal Lobe Injury Alterations in personality Occipital Lobe Injury Visual disturbances Cortical Disruption Reduce mental status or Amnesia Retrograde Unable to recall events before injury Antegrade Unable to recall events after trauma “Repetitive Questioning” Focal Deficits Hemiplegia, Weakness or Seizures

83
Signs & Symptoms of Brain Injury Physiological Changes
Upper Brainstem Compression Increasing blood pressure Reflex bradycardia Vagus nerve stimulation Cheyne-Stokes respirations Pupils become small and reactive Decorticate posturing Neural pathway disruption

84
Signs & Symptoms of Brain Injury Physiological Changes
Middle Brainstem Compression Widening pulse pressure Increasing bradycardia CNS Hyperventilation Deep and Rapid Bilateral pupil sluggishness or inactivity Decerebrate posturing

85
Signs & Symptoms of Brain Injury Physiological Changes
Lower Brainstem Injury Pupils dilated and unreactive Ataxic respirations Erratic with no pattern Irregular and erratic pulse rate ECG Changes Hypotension Loss of response to painful stimuli

86
Signs & Symptoms of Brain Injury Pediatric Head Trauma
Different pathology than older patients Skull can distort due to anterior and posterior fontanelles Bulging Slows progression of increasing ICP Intracranial hemorrhage contributes to hypovolemia Decreased blood volume in ped’s General Management Avoid hyperextension of head Tongue pushes soft pallet closed Ventilate through mouth and nose

87
Signs & Symptoms of Brain Injury Glasgow Coma Scale

88
Signs & Symptoms of Brain Injury Eye Signs
Physiological Issues Indicate pressure on CN-II, CN-III, CN-IV, & CN-VI CN-III (Oculomotor Nerve) Pressure on nerve causes eyes to be sluggish, then dilated, and finally fixed Reduced peripheral blood flow Pupil Size & Reactivity Reduced Pupillary Responsiveness Depressant drugs or Cerebral Hypoxia Fixed & Dilated Extreme Hypoxia
 Pressure on nerve causes eyes to be sluggish, then dilated, and finally fixed. Reduced peripheral blood flow. Pupil Size & Reactivity. Reduced Pupillary Responsiveness. Depressant drugs or Cerebral Hypoxia. Fixed & Dilated. Extreme Hypoxia.")
89
Facial Injury Facial Soft Tissue Injury Highly vascular tissue
Contribute to hypovolemia Superficial injuries rarely life threatening and rarely involve the airway Deep Injuries can result in blood being swallowed and endanger the airway Soft tissue swelling reduces airflow Consider likelihood of basilar skull fracture or spinal injury

90
Facial Injury Facial Dislocations & Fractures Common Fractures
Mandibular Deformity along jaw & loss of teeth Possible airway compromise if patient placed supine Evaluate for multiple fracture sites Maxillary & Nasal Le Fort I, II and III Criteria Orbit Involve Zygoma, Maxilla, and/or interior shelf Reduction of eye movement Possible Diplopia Limitation of jaw movement

92
Facial Injury Nasal Injury Rarely life threatening
Swelling & Hemorrhage interfere with breathing Epistaxis Most common problem AVOID NASOTRACHEAL INTUBATION Passage of ET tube into the cerebral cavity

93
Facial Injury Ear Injury External Ear Internal Ear
Pinna is frequently injured due to trauma Poor blood supply Poor healing Internal Ear Well protected from trauma My be injured due to rapid pressure changes Diving, Blast, or Explosions Temporary or permanent hearing loss Tinnitus may occur

94
Facial Injury Eye Injury Penetrating trauma
can result in long term damage Suspect small foreign body if patient complains of sudden eye pain and sensation of something on the eye DO NOT REMOVE ANY FOREIGN OBJECT Corneal Abrasions & Lacerations Common & usually superficial Hyphema Blunt trauma to the anterior chamber of the eye Blood in front of iris or pupil Sub-conjunctival Hemorrhage Less serious condition May occur after strong sneeze, severe vomiting or direct trauma

95
Facial Injury Eye Injury Acute Retinal Artery Occlusion
Non-traumatic origin Painless loss of vision in one eye Occlusion of retinal artery Retinal Detachment Traumatic origin Complaint of dark curtain/obstruction in the field of view Possibly painful depending on type of trauma Soft Tissue Lacerations

96
Neck Injury Blood Vessel Trauma Airway Trauma Blunt trauma Laceration
Serious hematoma Laceration Serious exsanguination Entraining of air embolism Cover with occlusive dressing Airway Trauma Tracheal rupture or dissection from larynx Airway swelling & compromise

97
Neck Injury Cervical Spine Trauma Other Neck Trauma Vertebral fracture
Paresthesia, anaesthesia, paresis or paralysis beneath the level of the injury Neurogenic shock may occur Other Neck Trauma Subcutaneous emphysema Tension pneumothorax Traumatic asphyxia Penetrating Trauma Esophagus or Trachea Vagus nerve disruption Tachycardia & GI disturbances Thyroid & Parathyroid glands High vascular

98
Assessment of Head, Facial & Neck Injuries
Scene Size-up Initial Assessment Airway, Breathing, Circulation Rapid Trauma Assessment Head, Face, Neck Glasgow Coma Scale Score Vital Signs Focused History & Physical Exam Detailed Assessment Ongoing Assessment

100
Head, Facial, & Neck Injury Management
Airway Suctioning Patient Positioning OPA & NPA Use Endotracheal Intubation Orotracheal Digital Nasotracheal Retrograde Direct RSI Cricothyrotomy Breathing Oxygen 15 LPM/NRB Ventilations 12-20/min Hyperoxygenate Circulation Hemorrhage Control Blood Pressure Maintenance Fluid resuscitation Consider PASG

101
Needle Cricothyrostomy
Locate Site Cricothyroid Membrane Cleanse upper anterior neck Aseptic Technique Iodine & Alcohol Prepare Equipment 14 ga IV catheter Syringe Transtracheal jet insufflation device 6.0 ET Hub Insert Catheter into membrane Downward Angle Feel “pop” Advance Catheter Attach BVM or jet ventilator Evaluate breath sounds Secure Catheter Similar to impaled object Consider 2nd catheter for exhalation

102
Surgical Cricothyrotomy
Locate Site Cricothyroid Membrane Cleanse upper anterior neck Aseptic Technique Iodine & Alcohol Prepare Equipment Commercial device Scalpel 4” ET Tube Insert scalpel into membrane Downward Angle Feel “pop” Enlarge opening Place short ET tube Evaluate breath sounds Secure device

103
Head, Facial, & Neck Injury Management
Hypoxia Prevent/Reduce Hyperoxygenation with BVM Hypovolemia Reduces cerebral perfusion & hypoxia Consider early management with 2 large bore IV’s and isotonic fluids Prevents slower compensatory mechanism Maintain SBP mmHg Consider PASG

104
Medications: Oxygen Primary 1st line drug Administer high flow
Hyperventilation is contraindicated Reduces circulating CO2 levels NRB: 15 LPM BVM: times per minute Keep SaO2 > 95%

105
Medications: Diuretics
Mannitol (osmotrol) MOA Large glucose molecule Does not leave blood stream Osmotic Diuretic Effective in drawing fluid from brain Contraindication Hypovolemia & Hypotension CHF Dose 1gm/kg CAUTION Forms crystals at low temperatures Reconstitute with rewarming & gentle agitation USE IN-LINE filter & PREFLUSH line
 MOA. Large glucose molecule. Does not leave blood stream. Osmotic Diuretic. Effective in drawing fluid from brain. Contraindication. Hypovolemia & Hypotension. CHF. Dose. 1gm/kg. CAUTION. Forms crystals at low temperatures. Reconstitute with rewarming & gentle agitation. USE IN-LINE filter & PREFLUSH line.")
106
Medications: Diuretics
Furosemide (Lasix) MOA Loop Diuretic Inhibits reabsorption of Na+ in Kidneys Increased secretion of water and electrolytes Na+, Cl–, Mg++, Ca++. Venous dilation & Reduces cardiac preload May be given in combination with Mannitol Contraindication Pregnancy: fetal abnormalities Dose Slow IVP or IM over 1-2 minutes 0.5-1 mg/kg: Commonly 40 or 80 mg
 MOA. Loop Diuretic. Inhibits reabsorption of Na+ in Kidneys. Increased secretion of water and electrolytes. Na+, Cl–, Mg++, Ca++. Venous dilation & Reduces cardiac preload. May be given in combination with Mannitol. Contraindication. Pregnancy: fetal abnormalities. Dose. Slow IVP or IM over 1-2 minutes mg/kg: Commonly 40 or 80 mg.")
107
Medications: Paralytics
Succinylcholine (Anectine) MOA Depolarizing Medication Causes Fasciculations Onset & Duration Onset: seconds Duration: 2-3 minutes Precaution Paralyzes ALL muscles including those of respiration Increases intraoccular eye pressure Contraindication Penetrating eye injury & Digitalis Dose 1-1.5 mg/kg IV Consider administration of 0.5 mg of Atropine to reduce fasciculations
 MOA. Depolarizing Medication. Causes Fasciculations. Onset & Duration. Onset: seconds. Duration: 2-3 minutes. Precaution. Paralyzes ALL muscles including those of respiration. Increases intraoccular eye pressure. Contraindication. Penetrating eye injury & Digitalis. Dose mg/kg IV. Consider administration of 0.5 mg of Atropine to reduce fasciculations.")
108
Medications: Paralytics
Pancuronium (Pavulon) MOA Non-depolarizing agent Does not affect LOC Onset & Duration Onset: 3-5 min Duration: min Dose Must premed with sedative mg/kg Vecuronium (Norcuron) MOA Non-depolarizing agent Does not affect LOC Onset & Duration Onset: < 1 min Duration: min Dose Consider premed with sedative mg/kg
 MOA. Non-depolarizing agent. Does not affect LOC. Onset & Duration. Onset: 3-5 min. Duration: min. Dose. Must premed with sedative mg/kg. Vecuronium. (Norcuron) MOA. Non-depolarizing agent. Does not affect LOC. Onset & Duration. Onset: < 1 min. Duration: min. Dose. Consider premed with sedative mg/kg.")
109
Medications: Sedatives
Diazepam (Valium) MOA Benzodiazepine Anti-anxiety Muscle relaxant Onset & Duration Onset: min Duration: min Dose 5-10 mg Midazolam (Versed) MOA Benzodiazepine 3-4x potent than valium Dose SLOW IVP 1 mg/min 1-2.5 mg titrated
 MOA. Benzodiazepine. Anti-anxiety. Muscle relaxant. Onset & Duration. Onset: 1-15 min. Duration: min. Dose mg. Midazolam (Versed) MOA. Benzodiazepine. 3-4x potent than valium. Dose. SLOW IVP. 1 mg/min mg titrated.")
110
Medications: Sedative
Morphine MOA Opium alkaloid Analgesic Sedation Anti-anxiety Reduces vascular volume & cardiac preload Increases venous capacitance Side Effects Respiratory depression Hypovolemia Dose 5-10 mg IVP Consider using promethezine with to reduce nausea Naloxone (Narcan) is antagonist
 is antagonist.")
111
Medications: Atropine
MOA Anticholinergic Parasympathetic Reduces parasympatholyic stimulation Reduce oral and airway secretions Reduce fasciculations Pupillary dilation Dose 0.5-1 mg rapid IVP

112
Medications: Dextrose
Consider if patient is hypoglycemic Only if VERIFIED by GLUCOMETER Dose 25 gm IVP Consider Thiamine if known alcoholic 100 mg Thiamine

113
Medications: Thiamine
Vitamin B1 Essential for the processing of glucose through Kreb’s cycle Chronic alcoholics can have B1 depletion Dose 100 mg IV or IM

114
Medications: Topical Anesthetic Spray
Xylocaine or Benzocaine Anesthetize oral and pharyngeal mucosa Reduces gag reflex Reduces likelihood of ICP associated with vomiting Inhibits nerve sensation Onset & Duration Onset: 15 seconds Duration: 15 minutes PRECAUTION Patient has reduced ability to remove oral fluids ASPIRATION can occur

115
Transport Considerations
Limit external stimulation Can increase ICP Can induce seizures Cautious about Air Transport Seizures

116
Emotional Support Have friend or family provide constant reassurance
Provided constant reorientation to environment if required Keeps patient calm Reduces anxiety

117
Special Injury Care Scalp Avulsion Pinna Injury
Cover the open wound with bulky dressing Pad under the fold of the scalp Irrigate with NS to remove gross contamination Pinna Injury Place in close anatomic position as possible Dress and cover with sterile dressing

118
Special Injury Care Eye Injury General Injury Corneal Abrasion
Cover injured and uninjured eye Prevents sympathetic motion Consider sterile dressing soaked in NS Corneal Abrasion Invert eyelid and examine eye for foreign body Remove with NS moistened gauze or Morgan’s Lens Avulsed or Impaled Eye Cover and Protect from injury General Care Calm & reassure patient

119
Special Injury Care Dislodged Teeth Impaled Objects Rinse in NS
Wrap in NS soaked gauze Impaled Objects Secure with bulky dressing Stabilize object to prevent movement Indirect pressure around wound

Similar presentations


























 and passes through foramina of skull There are 12 pairs of cranial nerves They have both name.>")

