Download presentation
Presentation is loading. Please wait.

1
Mechanical Injuries Of Brain and Meniges

2
1๐ Traumatic Lesions 2๐ Alterations

3
1๐ Traumatic Lesions Extracerebral lesions Intracerebral lesions

4
1๐ Traumatic Lesions Close injury Open injury

5
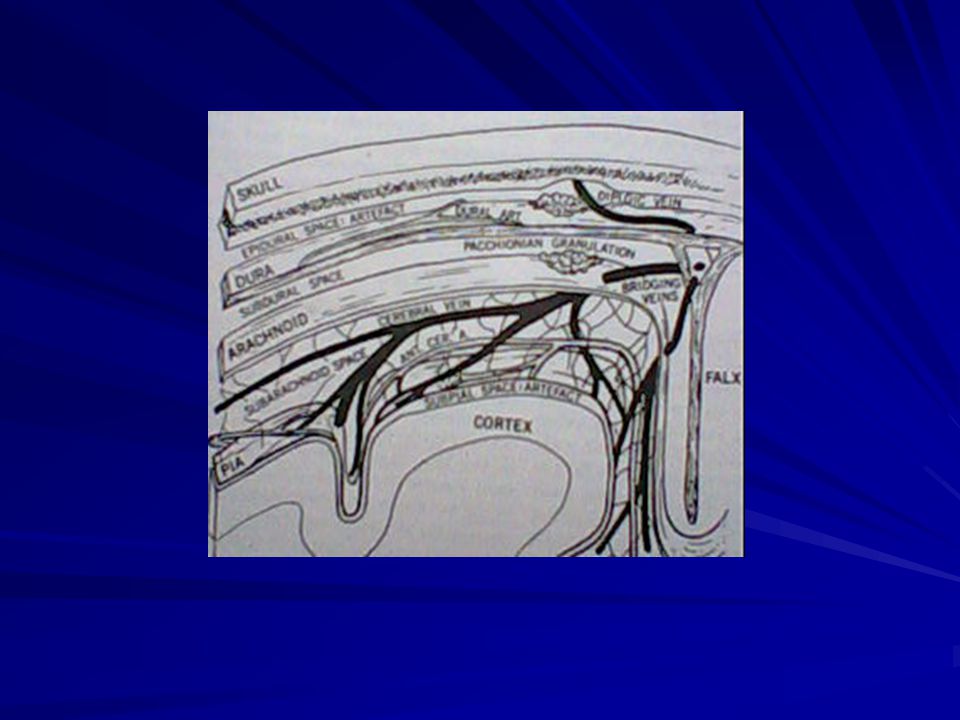
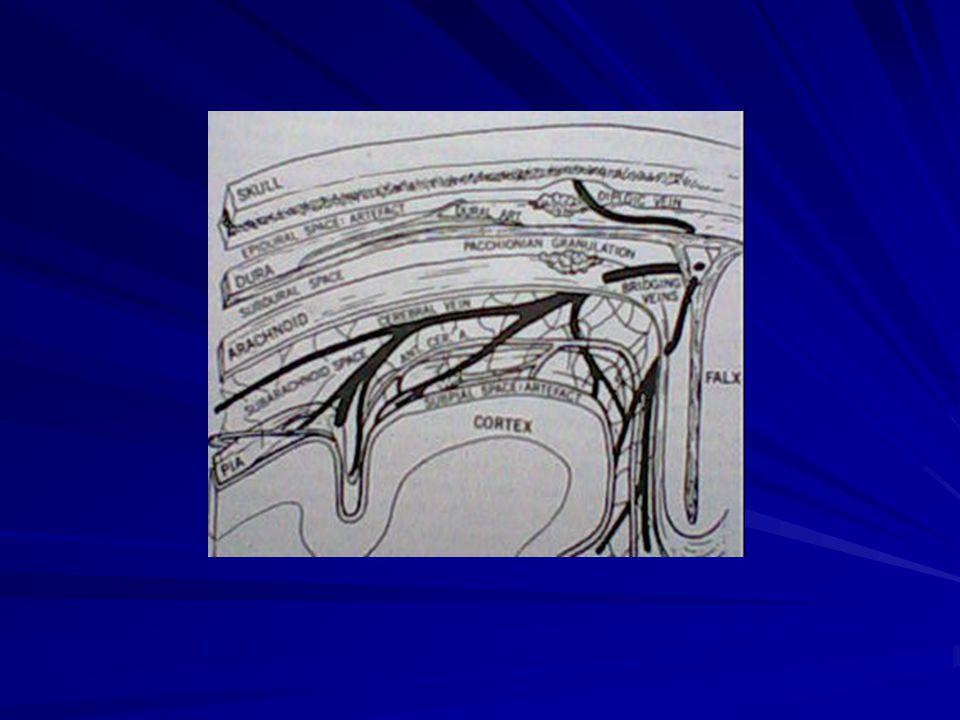
Extracerebral Lesions
Epidural bleeding Subdural bleeding Subaracnoid bleeding Intraventricular bleeding

7
Intracerebral Lesions
Contusions Lacerations (or Wounds)
")
8
2๐ Alterations Circulatory disorder Necroses and hemorrhages
Post-traumatic hydrocephalus Secondary infections Fat and air embolism

10
Epidural Bleeding

12
Epidural Bleeding Epidural / Extradural Hemorrhage / Hematoma

13
Causes Skull fracture Separation of dura and skull bone
Tear of a dural artery ,its branches and/or occasionally of a vein

14
Most common site: lateral convexity of a cerebral hemisphere
Location: it almost always at the site of a skull fracture

15
Uncommon occur in the elderly
Children: skull deformation with separation of the dura from the bone without skull fracture

16
Acute hematoma: artery bleeding
Delayed hematoma: venous bleeding, transient arterial spasm

17
Progression of the bleeding
Space occupying hematoma Increase intracranial pressure Confusion Alteration of consciousness Pupillary dilatation: on the hematoma side Central respiratory failure

18
If venous bleeding ,or transient arterial spasm: Lucid interval
Consciousness (may be) ,no signs of confusion: occipital poles and/or cerebellum
 ,no signs of confusion: occipital poles and/or cerebellum.")
19
Chronic Epidural Hematoma
The hematoma spontaneously shrinks and becomes encapsulated by fibrous connective tissue.

20
Subdural Bleeding

22
Subdural bleeding Trauma Rupture of aneurysm
Arteriovenous malformation

23
Vein: - Tearing of one or - Several bridging vein
- Insignificant trauma (sometime): abnormally located blood vessels
: abnormally located blood vessels.")
24
Artery: - particularly in branches of the middle cerebral artery
- severe cortical contusions and bleeding into subarachnoid space: (usually) tears of arachnoid membrane
 tears of arachnoid membrane.")
25
Artery: - More frequently on the side opposite the impact - (May) without brain contusions or significant subarachnoid hemorrhage
 without brain contusions. or significant subarachnoid hemorrhage.")
26
Time of onset Acute: within 12 to 24 hr. Subacute: from 24 hr. to 7 d.
Chronic: more than 7 d.

27
Most Location: over the convexities and the lateral aspects of the cerebral hemisphere
Often: extend over the base of frontal and temporal lobes Occasionally: between the hemisphere

28
In skull intact: occur as often as with skull fracture
Rare in the posterior cranial fossa , around the brain stem and cerebellum

29
Chronic Subdural Hematoma
Enlargement if untreat Isotonicity Local presence of fibrinolytic enzymes: bleeding tendency

30
Subaracnoid Bleeding

32
Subaracnoid bleeding Trauma / Nontrauma
Extension of intraventricular hemorrhage

33
Moderately severe blow to the face or forehead
Sudden ,usually severe hyperextension of the head , as from a fall onto the forehead

34
Subarachnoid over the brain stem and basal cisterns = hydrocephalus
Forgetfulness , confusion , psychotic state Spasticity of the lower extremities

35
Intraventricular bleeding

36
Intraventricular bleeding
Most often arterial in origin Trauma Non-trauma: such as rupture AVM or Aneurysms

37
Intracerebral Lesions

38
Contusions Lacerations (Wounds)
")
39
Contusions Contusion hemorrhage Contusion necrosis Contusion tear

40
Intracerebral Hematoma
In the deeper portions of contusions More frequent in the frontal and /or temporal lobes Location: white matter > grey matter

41
Intracerebral Hematoma
Secondary rupture into the ventricular system and/or the subarachnoid space usually does not occur.

42
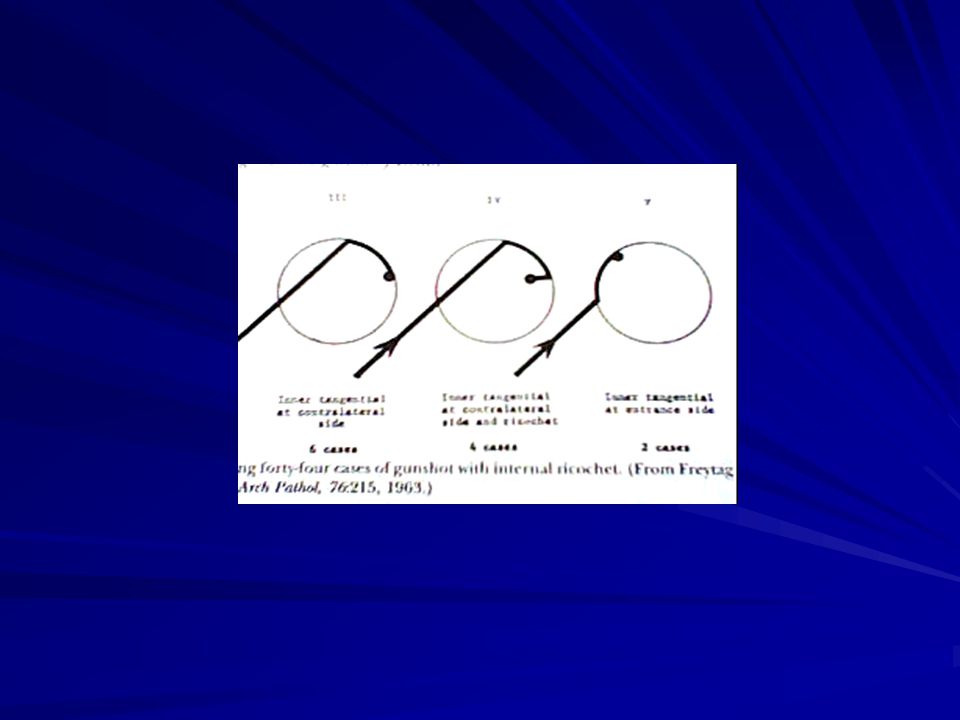
Lacerations Stab wounds Gunshot wounds

43
Gunshot wounds Shearing forces within brain tissue
Expansile cavitation Distant contusions (hemorrhages)
")
46
Contusions According to causative mechanism
Classification of Contusions According to causative mechanism

47
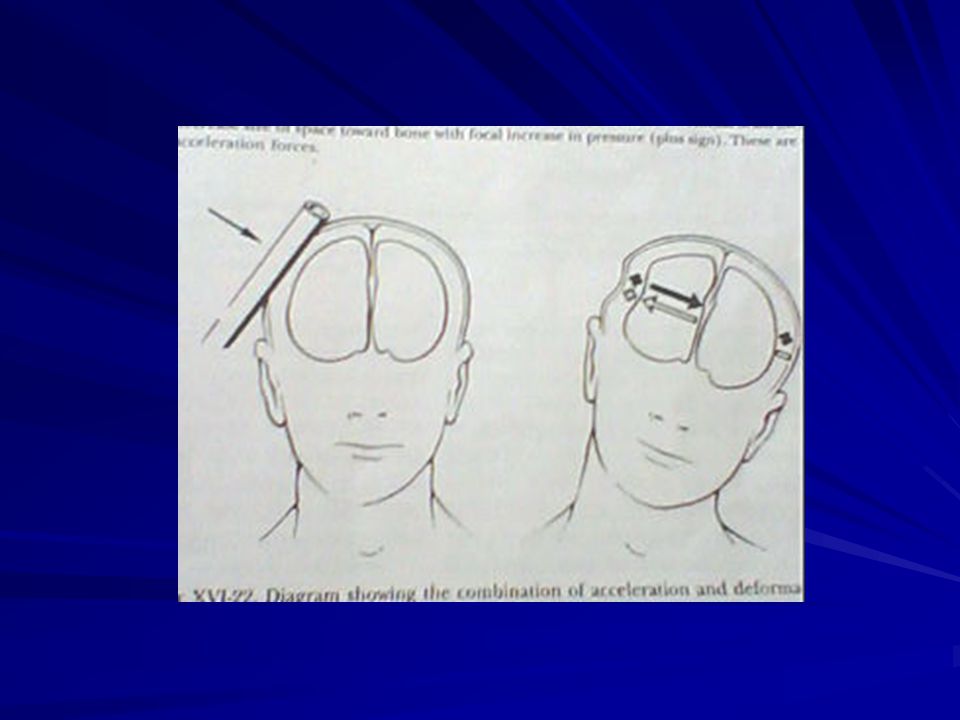
Depending on site and direction of impact
: Coup , Intermediary coup , Contrecoup Independent of site and direction of impact : Fracture contusion , Gliding contusion , Herniation contusion

52
Axonal injury Shearing forces due to blunt head injuries
Focal , diffuse Early ,the areas: little or no change on gross examination of the white matter Older lesions: slightly gray pallor

53
2๐ Alterations

54
2๐ Alterations Circulatory disorder Necroses and hemorrhages
Post-traumatic hydrocephalus Secondary infections Fat and air embolism

55
Circulatory disorder Swelling of the brain: edema and cell necrosis
Usually reversible Perifocal: surrounding a 1๐ brain lesion Generalize: a primary lesion , shock

56
Other rare causes Obstruction of the superior sagittal sinus
Traumatic thrombus or obstruction in internal carotid artery

57
Necroses/Hemorrhages
Vascular compression Shearing lesions

58
Necroses/Hemorrhages
Many lesion are large: such as midbrain and pons If rapidly progressing space occupying lesion: secondary lesion may appear within 30 mins. After injury Hemorrhage : sometimes small or absent

59
Hydrocephalus Traumatic or Non-traumatic cause
White matter loss following a shearing lesion and degeneration of myelinated axons Distension of ventricles by elevated pressure of the CSF

60
Secondary infections Meningitis Intracerebral abscesses

61
Meningitis An infected open injury caused by a foreign body
A fracture in the wall of one of the cranial sinuses associated with a tear in the dura and arachnoid

62
Intracerebral abscesses
In the vicinity of the primary lesion Complication: rupture into the underlying ventricle (Pyocephalus)
")
63
Fat and air embolism Primary or Secondary lesions
Fat embolism: fractures , stab wound at neck Air embolism: stab wound at neck , a skull fracture lacerating a paranasal dural sinus

Similar presentations










>")















