Download presentation
Presentation is loading. Please wait.

2
Perioperative Management of Heart Failure Gamal Fouad S Zaki, MD Professor of Anesthesiology Ain Shams University gamalzaki@gmail.com

3
Chronic Heart Failure Outline: Scope of the problem Classification Current understanding of pathophysiology Changing trends in drug therapy Anesthetic implications

5
Epidemiologic study Olmstead County, Minnesota, USA The prevalence of validated CHF was 2.2% With 44% having an EF higher than 50%.

6
European Journal of Heart Failure 2001

7
██ over 80 ██ 77.5-80 ██ 75-77.5 ██ 72.5-75 ██ 70-72.5 ██ 67.5-70 ██ 65-67.5 ██ 60-65 ██ 55-60 ██ 50-55 ██ 45-50 ██ 40-45 ██ under 40 ██ not available Life Expectancy at birth (years) Life Expectancy at birth (yrs) CIA World Factbook 2007 Estimates
 Life Expectancy at birth (yrs) CIA World Factbook 2007 Estimates")
8
Projected Increase in U.S. Population > 65 Years

9
Life Expectancy at birth in Egypt (years)
")
10
Population aged 65 and above in Egypt (%)
")
11
Chronic Heart Failure Epidemiology (USA) – Incidence: 400,000 new cases/year – Prevalence: About 5 million patients – Huge Costs 0.4 to 2% of the world’s adult population Progressive clinical syndrome: impaired ventricular function, exercise intolerance, ventricular arrhythmias & reduced life expectancy
 – Incidence: 400,000 new cases/year – Prevalence: About 5 million patients – Huge Costs 0.4 to 2% of the world’s adult population Progressive clinical syndrome: impaired ventricular function, exercise intolerance, ventricular arrhythmias & reduced life expectancy")
12
Chronic Heart Failure Multiple etiologies: CAD, Hypertension, Cardiomyopathy, Valvular Heart D,... High morbidity and mortality: – NYHA class I-II1-year mortality 5% – NYHA class IV1-year mortality 30-50% Normal About 50% have a Normal EF – Systolic dysfunction: failure to eject – Diastolic Dysfunction: failure to relax, fill, N. EF

13
Contrast ventriculogram (diastolic frame) in systolic and diastolic HF
 in systolic and diastolic HF")
14
LV Pressure–Volume Loops in Systolic and Diastolic Dysfunction

15
Mitral inflow patterns by Doppler Echocardiography Aurigemma, Gaasch. N Engl J Med 2004;351:1097

16
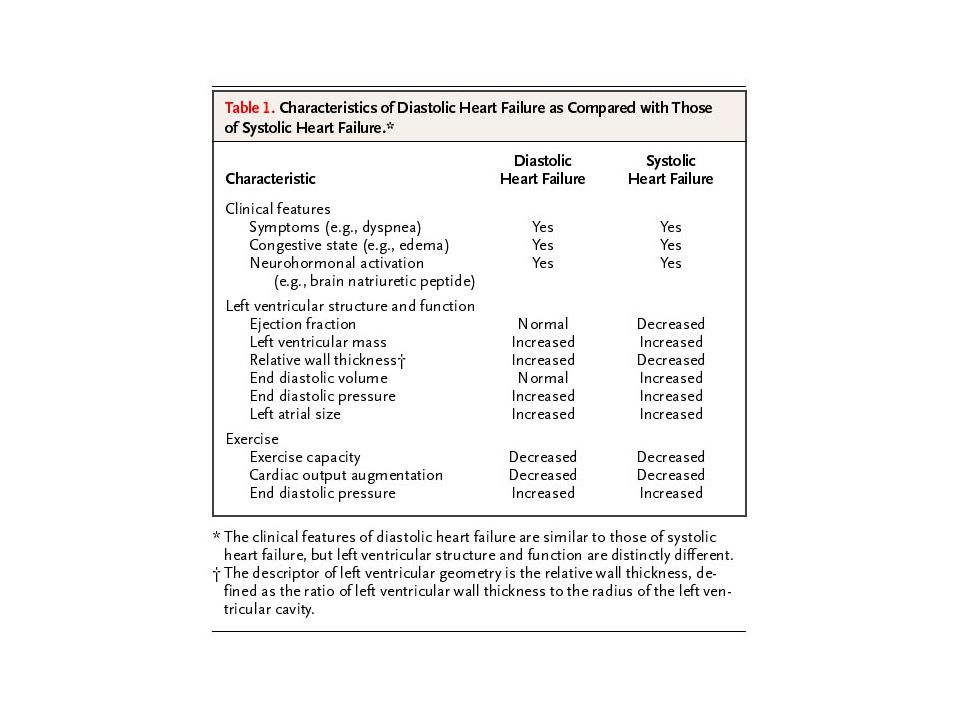
Diastolic vs Systolic HF Diastolic HF (HF w PSV) – Dyspnea – Congestion (edema) – ↑BNP – Normal LVEF – Normal LVEDV – Abnormal mitral inflow Systolic HF – Dyspnea – Congestion (edema) – ↑BNP – ↓LVEF – ↑LVEDV – Usually have diastolic abnormalities Aurigemma, Gassch. NEJM 2004;351:1097 Brucks. Am J Cardiol 2005;95:603-6

17
A Patients at high risk of developing HF but no structural/functional changes Hypertension, Coronary Artery Disease, Diabetes Mellitus B Structural changes associated with HF but never had Signs / Symptoms of HF LV hypertrophy, dilatation, hypocontractility, previous MI asymptomatic valvular HD, C Current or prior symptoms of HF associated with structural heart disease Dyspnea or fatigue due to LV dysfunction, patients who received previous ttt for HF D Symptoms of HF at rest despite maximum med therapy with structural heart disease Patients frquently hospitalized for HF, Cannot be safely discharged from the hospital StageDescriptionExamples Four stages of HF: ACC/AHA Hunt et al. Circulation 2001 Risk of Anesthesia/sSurgery related to underlying condition Risk of Anesthesia/sSurgery related to underlying condition, Preop Theraputic Optimization High risk of decompensation and adverse cardiac outcome Extreme risk of anesthesia, Patient usually in ICU Implications

18
Pathophysiology of HF Decreased renal blood flow activates renin- angiotensin-aldosterone system Sympathetic activation: Increase LV afterload, 1 -receptor downregulation Increase: total body water, total body Na blood volume Increase TNFα, ANP and BNP BNP <15pmol/L excludes HF etiology of dyspnea TNFα (pg/mL) NYHA Class Torre-Amione JACC 1996 Feldman JACC 2000
 NYHA Class Torre-Amione JACC 1996 Feldman JACC 2000")
19
LV Remodeling Pathophysiology of HF: LV Remodeling Changes in LV size, shape and function LV less elliptical, more spherical leads to progressive impairment of function, and ultimately resulting in reduced contractility and ejection fraction Modified by ACE Inhibitors & β-Blockers Slowing or reversing remodeling may improve outcome in HF Cohn. JACC 2000

20
LV Remodeling Pathophysiology of HF: LV Remodeling Remodeling Stimuli (wall stress: pressure or volume overload, Myocyte injury MI) Neurohumoral activation, oxidative stress, cytokine activation Local: Myocyte loss (necrosis, apoptosis) extracellular matrix changes, intracellular calcium regulation, gene expression Systemic: LV dilat., Myocyte hypertrophy Neurohumoral changes: Maladaptive
 Neurohumoral activation, oxidative stress, cytokine activation Local: Myocyte loss (necrosis, apoptosis) extracellular matrix changes, intracellular calcium regulation, gene expression Systemic: LV dilat., Myocyte hypertrophy Neurohumoral changes: Maladaptive")
21
Groban et al. Anesth Analg 2006 Pathophysiology of HF: LV Remodeling

22
Management of HF Changing trends in drug therapy: 1980: All HF patients get Dig, β -Blockers are bad for failing hearts 2008: Digitalis moved to end of list, β -Blockers good for the failing heart, ACE inhibitors are 1 st line drugs Logic: neurohumoral antagonism

23
Management of HF Disease Modifying therapy: – ACE inhibitors, Angiotensin II receptor blockers – β-Blockers: Carvedilol, bisoprolol, metoprolol – Aldosterone antagonists Symptomatic therapy: – Digoxin – Diuretics Other: Anemia, Anticoagulation, Lifestyle

24
Management of HF Non-Transplant Surgical Options: Revascularization of hibernating myocardium LV reshaping: Dor Procedure

25
Modified Dor Procedure

26
Partial left ventriculectomy & MV repair

27
Management of HF Non-Transplant Surgical Options: Revascularization of hibernating myocardium LV reshaping: Dor Procedure Correction of Mitral Regurge Cardiac Support Devices: Acorn CorCap

28
Cardiac Support Devices Acorn CorCap Heart Net

29
Management of HF Non-Transplant Surgical Options: Revascularization of hibernating myocardium LV reshaping: Dor Procedure Correction of Mitral Regurge Cardiac Support Devices: Acorn CorCap Cardiac Resynchronization therapy / AICD LVAD

30
Anesthetic Implications Detailed cardiac evaluation: coronaries, valves, myocardium, PAP, thrombi to ensure hemodynamic stability during Anesthetic I/M Other comorbidities included in anesthetic plan: renal, hepatic, CNS, anemia Targets Preoperative Optimization of drug therapy: afterload reduction, β-blockers, diuretics, Targets: HR, Lung, Periph edema, Circulating volume

32
Anesthetic Implications Perioperative questions ACE inhibitors: withdraw or continue ?? Initiation of β-blockade: under-utilized Dangerous β-blocker withdrawal: Dangerous Diuretics titrated against intravscular volume, pulmonary and peripheral edema, trying to avoid hypokalemia, hypovolemia Digoxin: long t ½, narrow therapeutic margin Avoid: NSAIDs, Ca CBs, Steroids, tricyclic antidepressants, Class I antiarrhythmics

33
Anesthetic Implications Preoperative medication Anxiolytic/sedative meds given with caution for risk of reducing sympathetic tone and respiratory depression Patients will poorly tolerate respiratory acidosis &/or hypoxia (increase PVR) Supplemental oxygen Monitor vital signs
 Supplemental oxygen Monitor vital signs")
34
Anesthetic Implications Choice of technique Noncardiac surgery: Regional A: if patient can lie flat and coagulation mechanisms are adequate?? General A: Positive pressure ventilation needed to control pulmonary edema

35
Anesthetic Implications Choice of technique Cardiac surgery Choice of drugs less important than fluid and medical management, transfusion decisions, pacemaker, aortic balloon adjustments.., and prompt correction of hemodynamics (vasoactive bullets ready) Classic technique: High dose opioids: problems with awareness, bradycardia, chest rigidity Etomidate rather than thiopental or propofol Ketamine in pediatric pts
 Classic technique: High dose opioids: problems with awareness, bradycardia, chest rigidity Etomidate rather than thiopental or propofol Ketamine in pediatric pts")
36
Anesthetic Implications Choice of technique Cardiac surgery Inhaled agents (including N2O) are myocardial depressants esp Halothane, enflurane Inhaled agents: myocardial depression, vasodilation, decrease automaticity, conduction, refractoriness: dysrhythmia Opioids + inhalational agents (Sevo, Iso, Des) Sevoflurane (less myocardial depression, less SVR reduction), anesthetic preconditioning
 are myocardial depressants esp Halothane, enflurane Inhaled agents: myocardial depression, vasodilation, decrease automaticity, conduction, refractoriness: dysrhythmia Opioids + inhalational agents (Sevo, Iso, Des) Sevoflurane (less myocardial depression, less SVR reduction), anesthetic preconditioning")
37
Anesthetic Implications Intraoperative considerations Monitoring Invasive hemodynamic monitoring: a must TEE: especially useful for volume assessment compared to Rt Sided Catheters owing to abnormal and changing pressure/volume relationships Prebypass: avoid increases in SVR, HR, oxygen consumption Antifibrinolytics?

38
Anesthetic Implications Postoperative management Cardiac function: pharmacologic manipulation, epicardial pacing, electrolytes, Hb Pain: risk of tachycardia, stress, diastolic filling: Systemic Opioids: bolus, pump, PCA Epidural LA+Opioids? (Hematoma) Intrathecal Morphine 10μg/kg+fentanyl 25μg 1 hr before induction & 2 hr before heparin Avoid NSAIDs
 Intrathecal Morphine 10μg/kg+fentanyl 25μg 1 hr before induction & 2 hr before heparin Avoid NSAIDs.")
39
Acute exacerbations of Chronic HF No change in therapy in last 2 decades Shift in paradigm to cardioprotection Loop diuretics, opiates, IV nitrates (tolerance), inotropes (hypotension): Dobutamine ?, milrinone, enoximone Nesiritide (human recombinant BNP), Levosimendan ( inodilator, calcium sensitizer Non-invasive Ventilation
, inotropes (hypotension): Dobutamine , milrinone, enoximone Nesiritide (human recombinant BNP), Levosimendan ( inodilator, calcium sensitizer Non-invasive Ventilation")
40
Levosimendam vs dobutamine for severe low-output HF (LIDO study) 203 patients Levo 24 mg/kg 10 min + 0.1 mg/kg/min vs dob 5 µg/kg/min 1 o outcome: CO to ↑ 30%; PCWP ↓25% 28% Levo patients, 15% dob patients achieved primary outcome Fewer deaths with levo (HR 0.57) Follath. Lancet 2002;360:196-202 Levo Dob Time (days) Percent surviving
 Percent surviving.")
41
Nesiritide (B-type natriuretic peptide) for acute exacerbations of HF Nesiritide better than nitroglycerine or placebo added to standard therapy for decompensated CHF (hemodynamics, symptoms) Nesiritide better than dobutamine for decompensated CHF (premature beats, tachycardia) Am Heart J 2002;144:1102-8 JAMA 2002;287:1531-40 J Cardiothorac Vasc Anesth 2004;18:780-7
 for acute exacerbations of HF Nesiritide better than nitroglycerine or placebo added to standard therapy for decompensated CHF (hemodynamics, symptoms) Nesiritide better than dobutamine for decompensated CHF (premature beats, tachycardia) Am Heart J 2002;144: JAMA 2002;287: J Cardiothorac Vasc Anesth 2004;18:780-7")
42
Aging population and better survival of patients with CV disease will increase the number of HF patients coming to surgery Prevention is the only treatment LV Remodeling related to progression of HF Diastolic HF is not rare and frequently misdiagnosed and mismanaged Perioperative management relies on evaluation, therapeutic optimization and attention to comorbid conditions Avoid myocardial depressants

43
Foxglove, William Withering 1785

46
McMurray Circulation 2004;110:3281-8

47
Is there a role for positive inotropes for any patients with CHF? 1 Cardiogenic shock Congestion, hypoperfusion no shock? Support until resolution of other conditions 2 Hospitalization for HF, no “need” 3 Intermittent outpatient therapy? Bridging until transplant? “Destination” end of life care? 1 Stevenson. Circulation 2003;108:367-72 2 Hayes. NEJM 1994;330:1717-22 3 Cuffe. JAMA 2002;287:1541-7

48
Hunt et al. ACC/AHA Guidelines for the evaluation and management of chronic heart failure in the adult: An executive summary. J Heart Lung Transplant 21:189-203, 2003

50
LV Remodeling Simplified

51
Copyright restrictions apply. Groban, L. et al. Anesth Analg 2006;103:557-575 Figure 3. Schematic of the renin-angiotensin-aldosterone system and site of action of angiotensin-converting enzyme (ACE) inhibitors (one slash), angiotensin receptor blockers (dotted slash), and aldosterone receptor blockers (double slash)
 inhibitors (one slash), angiotensin receptor blockers (dotted slash), and aldosterone receptor blockers (double slash).")
54
Copyright restrictions apply. Groban, L. et al. Anesth Analg 2006;103:557-575 Table 1. Selected Clinical Trials of Angiotensin-Converting Enzyme Inhibitors in Heart Failure (HF)
.")
55
Copyright restrictions apply. Groban, L. et al. Anesth Analg 2006;103:557-575 Table 2. Angiotensin Receptor Blocker Trial in Heart Failure (HF)
.")
56
Copyright restrictions apply. Groban, L. et al. Anesth Analg 2006;103:557-575 Figure 4. Effects of inotropic therapy on intracellular calcium handling in cardiac myocytes

59
A Hypertension, Coronary Artery Disease, Diabetes Mellitus B LV hypertrophy, dilatation, hypocontractility, previous MI asymptomatic valvular HD, C Dyspnea or fatigue due to LV dysfunction, patients who received previous ttt for HF D LV hypertrophy, dilatation, hypocontractility, previous MI asymptomatic valvular HD, Stage Risk of Anesthesia/sSurgery related to underlying condition Risk of Anesthesia/sSurgery related to underlying condition, Preop Theraputic Optimization High risk of decompensation and adverse cardiac outcome Extreme risk of anesthesia, Patient usually in ICU Implications Examples Four stages of HF: ACC/AHA Hunt et al. Circulation 2001

Similar presentations


























. “Heart (or cardiac) failure is the pathophysiological state in which the heart is unable to pump blood at a rate commensurate.>")
 failure is the state in which the heart is unable to pump blood.>")