Download presentation
Presentation is loading. Please wait.

2
Fluid and Electrolyte balance Dr Sanjay De Bakshi MS;FRCS

3
Distribution of body water

4
Distribution of Body Water (contd.) Neonates---75 to 80%. Infants and children------65%. Adults:- Males----60% Females---50%.

5
Distribution of Body Water (contd.) Body water is also inversely proportional to body fat.
 Body water is also inversely proportional to body fat.")
6
Measurement of Body water and its Components

7
WATER EXCHANGE

8
WATER EXCHANGE (60 to 80kg man.) GAIN
 GAIN")
9
WATER EXCHANGE LOSS

10
MRI OF THE BRAIN SAGGITAL SECTION

13
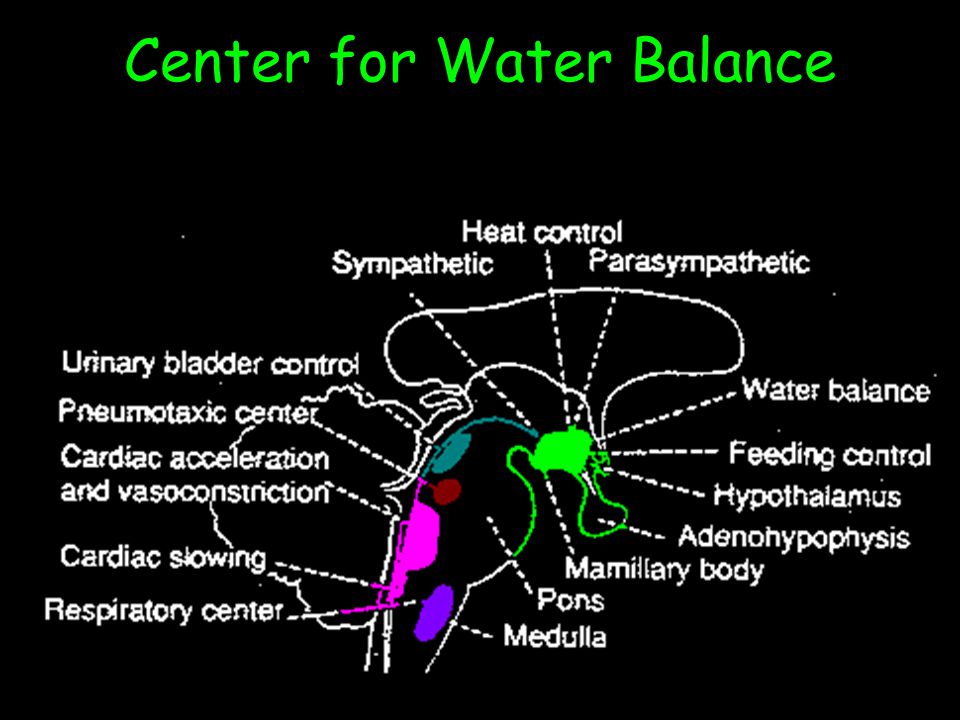
Center for Water Balance

15
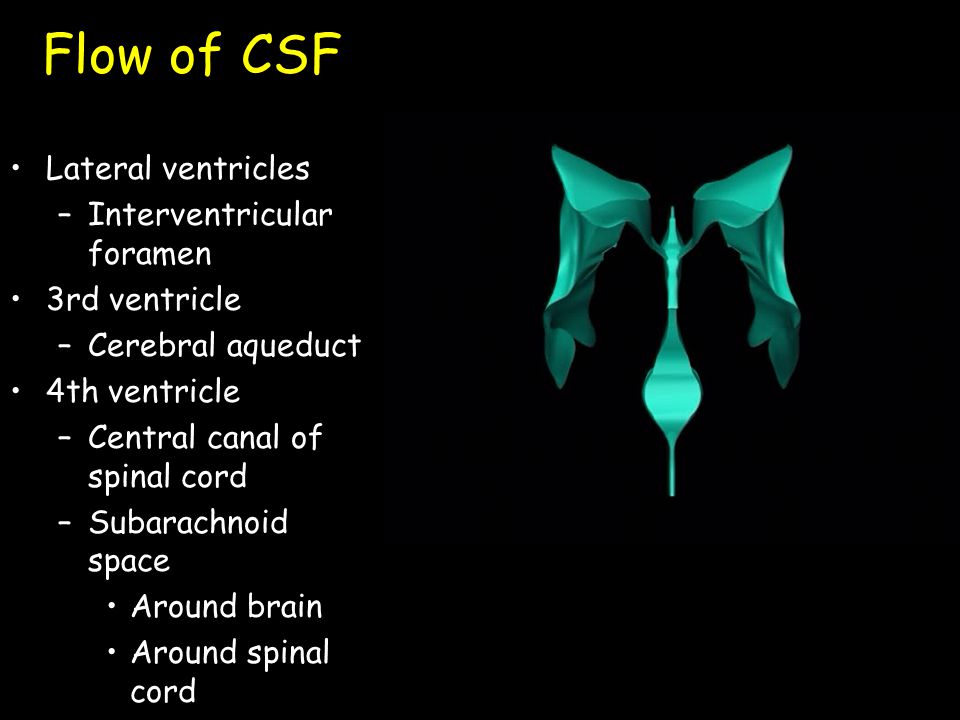
Flow of CSF Lateral ventricles –Interventricular foramen 3rd ventricle –Cerebral aqueduct 4th ventricle –Central canal of spinal cord –Subarachnoid space Around brain Around spinal cord

16
Flow of CSF Lateral ventricles –Interventricular foramen 3rd ventricle –Cerebral aqueduct 4th ventricle –Central canal of spinal cord –Subarachnoid space Around brain Around spinal cord

17
Flow of CSF Lateral ventricles –Interventricular foramen (Monro) 3rd ventricle –Cerebral aqueduct (Sylvius) 4th ventricle –Central canal of spinal cord (Magendie and Luschka) –Subarachnoid space Around brain Around spinal cord
 3rd ventricle –Cerebral aqueduct (Sylvius) 4th ventricle –Central canal of spinal cord (Magendie and Luschka) –Subarachnoid space Around brain Around spinal cord")
18
Function of Cerebrospinal Fluid Cushions and supports brain Transports respiratory gases, nutrients, wastes –Ependymal cells Produced by the choroid plexus –Network of capillaries in each ventricle –Materials for CSF taken from blood –Replaced every 8 hours Via projections from the subarachnoid space into the dural sinuses Removed during a spinal tap for diagnosis of meninges or brain infections

19
Control of Water Intake In humans, the thirst center is located in the anterior hypothalamus. The primary stimuli for thirst are hypertonicity and hypovolemia. Osmoreceptors in the anterior wall of the third ventricle mediate the osmotic regulation of thirst. Hypovolemia and hypotension stimulate thirst through the activation of low-pressure (venous) and high-pressure (arterial) vascular stretch receptors. Impulses from these receptors are transmitted by the vagus and the glossopharyngeal nerves to the medulla and from there to the hypothalamus. In addition, the hypothalamus is stimulated directly by angiotensin II.
 and high-pressure (arterial) vascular stretch receptors. Impulses from these receptors are transmitted by the vagus and the glossopharyngeal nerves to the medulla and from there to the hypothalamus. In addition, the hypothalamus is stimulated directly by angiotensin II..")
20
The hypothalamus and thirst response THIRST CENTER STIMULATED BY:- 1)Increased Plasma Osmolarity Increased thirst Increased ADH 2)Decreased ECF Volume a) Decreased stimulation of Atrial Type B receptors Increased sympathetic stimulation b) Decreased pressure at Renal Afferent Arteriole Stimulation of Angiotensin mechanism c) Low Sodium causes stimulation of the Renin-angiotensin System Increased Angiotensin II Vasoconstriction ADH Aldosterone Thirst
Increased Plasma Osmolarity Increased thirst Increased ADH 2)Decreased ECF Volume a) Decreased stimulation of Atrial Type B receptors Increased sympathetic stimulation b) Decreased pressure at Renal Afferent Arteriole Stimulation of Angiotensin mechanism c) Low Sodium causes stimulation of the Renin-angiotensin System Increased Angiotensin II Vasoconstriction ADH Aldosterone Thirst")
21
Renin angiotensin mechanism Low pressure at the afferent arteriole. Low sodium at the macula densa Increased Renin sectretion from the JG apparatus JG cells, Macula densa & Lacis (Polkissen)cells AngiotensinAngiotensinI Angiotensin II ACE
cells AngiotensinAngiotensinI Angiotensin II ACE.")
22
Fluid exchange

23
Fluid dynamics at the capillary CHP = Capillary Hydrostatic Pressure COP = Capillary Osmotic Pressure IFHP = Interstitial Fluid Hydrostatic Pressure IFOP =Interstitial Fluid Osmotic Pressure

24
Osmotic pressure DEFINITION:- Is the pressure that drives water across the semipermeable cell membrane and is dependant on those substances which fail to pass through the membrane. The total number of osmotically active particles is approximately 290 to 310 mO in each component.

25
Some more definitions What is a Mole and a Molar Solution? Molarity- A mole is a gram molecular weight of a substance. NaCl=58.5gm; C 6 H 12 O 6 =180gm. 1 molar solution = gram molecular weight of the substance in a litre of solution. 1 mol= 1000mmol.

26
Some calculations OSMOTIC PRESSURE depends on the actual number of particles in solution. Therefore, 1 gram mol weight of NaCl ie. 58.5gm of NaCl in 1 litre exerts how much of osmotic pressure? 58.5gm NaCl exerts--------------2000mosmol/L 9gm NaCl exerts--------------2000 x 9 58.5 = 307.69 mosmol/L 180gm C6H12O6 exerts------------1000mosmol/L 50gm C6H12O6 exerts-----------1000 x 50 180 = 277.77 mosmol/L

27
INTRACELLULARPLASMAECF IONIC COMPOSITION OF DIFFERENT BODY FLUIDS CATIONS ANIONSCATIONSANIONSCATIONSANIONS Na = 10HPO 4 = 150 Na = 142Cl = 103Na = 144Cl = 114 K = 150SO 4 = 150 K = 4HCO 3 = 27 K = 4HCO 3 = 30 Mg = 40HCO 3 = 10 Ca = 5SO 4 = 3Ca = 3SO 4 = 3 Prt = 40Mg = 3PO 4 = 3Mg = 2PO 4 = 3 Org Ac = 5 Prt = 16 Prt = 1 Urea = 24

28
OSMOLAR GAP CO = 2 X [Na]+[glucose (mg/dl)] / 20 + [urea (mg/dl) ] / 3 - 2 The osmolality gap is an indication of unmeasured solute in the blood.This is caused because complete dissociation of particles in vivo is only 93%. It is determined by the measured osmolality (MO) minus the calculated osmolality (CO). A large positive (>14) osmolality gap can help identify the presence in plasma of substances such as ethanol, methanol, isopropanol, ethylene glycol, propylene glycol, and acetone.
![OSMOLAR GAP CO = 2 X [Na]+[glucose (mg/dl)] / 20 + [urea (mg/dl) ] / The osmolality gap is an indication of unmeasured solute in the blood.This is caused because complete dissociation of particles in vivo is only 93%.](http://images.slideplayer.com/12/3451651/slides/slide_28.jpg "It is determined by the measured osmolality (MO) minus the calculated osmolality (CO). A large positive (>14) osmolality gap can help identify the presence in plasma of substances such as ethanol, methanol, isopropanol, ethylene glycol, propylene glycol, and acetone..")
29
ANION GAP Proper interpretation of the OG also requires knowledge of the anion gap (AG = Na - HCO3 - Cl), the blood pH, and qualitative testing of the plasma ketone bodies (KETO). Determinations of MO and for CO should be performed on the same plasma sample.

30
ANION GAP The formula (Anion Gap = Na + - HCO 3 - - Cl - ). Also important to define the TYPE of metabolic acidosis.

31
Importance of Osmolar and Anion Gap When the OG is combined with blood pH and AG, poisonings with toxic alcohols can be quickly recognized. The presence of low blood pH, elevated AG, and greatly elevated OG (>14) is a medical emergency that requires prompt treatment. SITUATIONpHAGKETOGLUOG (mOsm/kg H20)* Ethanol onlyNNNNHI 100 mg/dl = 21.7 Methanol (late)LOHINN or HIN or HI** 50 mg/dl = 15.6 IsopropanolNNPOSNHI 100 mg/dl = 16.7 (also acetone) Ethylene GlycolLOHINN 50 mg/dl = 8.1 Alcoholic KetoacidosisLOHI Weak POS 300HI (ethanol) Diabetic KetoacidosisLOHIPOS300 N or UP (usually < 20-25) 50 mg/dl = 8.6 (acetone)
 is a medical emergency that requires prompt treatment. SITUATIONpHAGKETOGLUOG (mOsm/kg H20)* Ethanol onlyNNNNHI 100 mg/dl = 21.7 Methanol (late)LOHINN or HIN or HI** 50 mg/dl = 15.6 IsopropanolNNPOSNHI 100 mg/dl = 16.7 (also acetone) Ethylene GlycolLOHINN 50 mg/dl = 8.1 Alcoholic KetoacidosisLOHI Weak POS 300HI (ethanol) Diabetic KetoacidosisLOHIPOS300 N or UP (usually < 20-25) 50 mg/dl = 8.6 (acetone).")
32
Case Study: A sixty-seven year old white male was found pulseless and resuscitated; then brought to the emergency room. He had been reported to be drinking in a bar all afternoon, and had then fallen from a ten foot balcony to snow covered ground. He arrived in the emergency room with a fractured occiput and was unresponsive.

33
Admission Data: Na=141 mEq/lUrea=8 mg/dlpH=7.30 Cl=105 mEq/lGLU=181 mg/dlMO=353 mOsm/kg HCO 3 =19 mEq/lKETO=Neg Anion Gap =Na - Cl- HCO 3 = 141 - 105- 19 = Calculated Osmolality = 2 x Na + GLU/20 + Urea/3 -2 = 282+ 181/20 + 8/3 -2 = 0smolar Gap =MO - CO= 353 - 292 = If we assume OG is due to ethanol, then ethanol concentration would be 61/21.7 x 100 mg/dl = 281 mg/dl The measured ethanol concentration on this sample was 270 mg/dl. 17 292 61
34
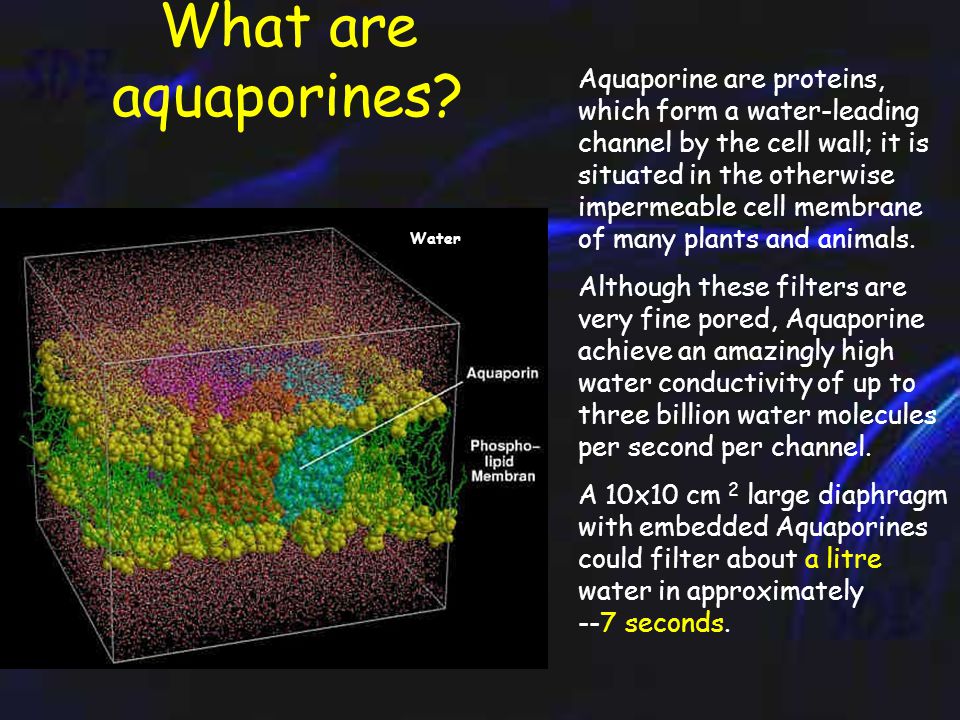
What are aquaporines? Water Aquaporine are proteins, which form a water-leading channel by the cell wall; it is situated in the otherwise impermeable cell membrane of many plants and animals. Although these filters are very fine pored, Aquaporine achieve an amazingly high water conductivity of up to three billion water molecules per second per channel. A 10x10 cm 2 large diaphragm with embedded Aquaporines could filter about a litre water in approximately --7 seconds.

35
The overall structure of AQP1 is that of a tetramer, the four parts (monomers) of which each define a single pore. These monomers are arranged side by side in a tight cluster, with the pores running parallel. Each monomer in turn comprises six membrane-spanning helices that partially surround two shorter helices. The short non-membrane- spanning helices make up the major portion of the pore. Each pore has a dumbbell-like shape. One broad end is the cytoplasmic vestibule; the other is the extracellular vestibule. The bar of the dumbbell is the selectivity filter, which narrows to a constriction region on the extracellular end. Figure: The AQP1 tetramer viewed looking down the pores from the cytoplasmic side, normal to the membrane. One monomer of the four is represented as a solid space-filling model.

36
Computer simulation of the action of Aquaporines Left: Water molecules (red/white) diffuse over Aquaporin (blue) by the cell membrane (yellow/green). The cutout right shows the ' dance ' of an individual water molecule on its way by the channel." “Diagram: Max-Planck-Institut for Biophysical Chemistry "

37
Case Study : A healthy young lady of 32yrs. Undergoes an appendicectomy. She is fine till the third post- operative day, when she has three grand mal seizures. She recieves 20mgm of diazepam and 250mgm of Phenytoin IV and undergoes laryngeal intubation with mechanical ventilation. CAUSE:- Infused 5% Dextrose only on Day 1. Plenty of plain water orally on Day 2.

38
Case Study : Her body weight is 46kgs. Sodium concentration- 112mmol/litre Potassium concentration- 4.1 mmol/litre Serum osmolality- 228mOsm/kg of water. Urine osmolality- 510mOsm/kg of water. Withhold water. Infusion of 3 per cent Sodium Chloride. Intravenous administration of 20mgm of Furosemide.

39
TYPES OF HYPONATRAEMIA Total body water (TBW) decreases; total body sodium (Na + ) decreases to a greater extent. The extracellular fluid (ECF) volume is decreased. TBW increases while total sodium remains normal. The ECF volume is increased minimally to moderately, but edema is not present Total body sodium increases, and TBW increases to a greater extent. The ECF is increased markedly, and edema is present. Water shifts from the intracellular to the extracellular compartment, with a resultant dilution of sodium. The TBW and total body sodium are unchanged. This condition occurs with hyperglycemia The aqueous phase is diluted by excessive proteins or lipids. The TBW and total body sodium are unchanged. This condition is seen with hypertriglyceride mia and multiple myeloma.
 volume is decreased. TBW increases while total sodium remains normal. The ECF volume is increased minimally to moderately, but edema is not present Total body sodium increases, and TBW increases to a greater extent. The ECF is increased markedly, and edema is present. Water shifts from the intracellular to the extracellular compartment, with a resultant dilution of sodium. The TBW and total body sodium are unchanged. This condition occurs with hyperglycemia The aqueous phase is diluted by excessive proteins or lipids. The TBW and total body sodium are unchanged. This condition is seen with hypertriglyceride mia and multiple myeloma..")
40
Pathophysiology: Serum sodium is regulated by thirst, ADH, the renin-angiotensin-aldosterone system, and variations in renal handling of filtered sodium. Increases in serum osmolarity above the normal range (280-300 mOsm/kg) stimulate hypothalamic osmoreceptors, which, in turn, cause an increase in thirst and in circulating levels of ADH. ADH Free water absorption from the Kidneys Aldosterone Absorption of sodium at the distal renal tubule. K+K+ Vol
 stimulate hypothalamic osmoreceptors, which, in turn, cause an increase in thirst and in circulating levels of ADH. ADH Free water absorption from the Kidneys Aldosterone Absorption of sodium at the distal renal tubule. K+K+ Vol.")
41
NORMAL SODIUM BALANCE GI TRACT DCT 4-5% CD 2-3% INTAKE 80 –100 mmols/day (5-6gms) Secretions 1000mmols/day Plasma Sodium (136-144mmols) Kidney Loss in Urine (70-90mmols/day) Faeces 5mmols/day PCT 75% LH 22%
 Secretions 1000mmols/day Plasma Sodium ( mmols) Kidney Loss in Urine (70-90mmols/day) Faeces 5mmols/day PCT 75% LH 22%")
42
Clinical features of hyponatraemia Anorexia Nausea and vomiting Difficulty concentrating Confusion Lethargy Agitation Headache Seizures

43
Hypovolemic hyponatremia - sodium and free water are lost and replaced by inappropriately hypotonic fluids, such as tap water, half-normal saline, or dextrose in water oExcess fluid losses (eg, vomiting, diarrhea, excessive sweating, GI fistulas or drainage tubes, pancreatitis, burns) that have been replaced primarily by hypotonic fluids oAcute or chronic renal insufficiency oSalt-wasting nephropathy oCerebral salt-wasting syndrome H2OH2ONa H2OH2O
 that have been replaced primarily by hypotonic fluids oAcute or chronic renal insufficiency oSalt-wasting nephropathy oCerebral salt-wasting syndrome H2OH2ONa H2OH2O")
44
Euvolemic hyponatremia implies normal sodium stores and a total body excess of free water. This occurs in patients who take in excess fluids. oPsychogenic polydipsia, often in psychiatric patients oAdministration of hypotonic intravenous (IV) or irrigation fluids in the immediate postoperative period oInfants who may have been given inappropriate amounts of free water H2OH2O Na
 or irrigation fluids in the immediate postoperative period oInfants who may have been given inappropriate amounts of free water H2OH2O Na.")
45
Hypervolemic hyponatremia occurs when sodium stores increase inappropriately. oHistory of hepatic cirrhosis, congestive heart failure, or nephrotic syndrome, in which patients are subject to insidious increases in total body sodium and free water stores oUncorrected hypothyroidism or cortisol deficiency oSIADH oConsumption of large quantities of beer or use of the recreational drug MDMA (ecstasy) H2OH2O Na
 H2OH2O Na.")
46
HYPONATRAEMIA GI or Skin

47
Effect of hyponatraemia and its correction Normal Immediate effect of hypo state Water gain Rapid adapta- tion Loss of Na, K, Cl. Slow adapta- tion Loss of organic osmolytes Proper therapy Incorrect therapy Osmotic demyeli nation Water

48
Treatment of Hyponatraemia In asymptomatic patients: When symptoms are absent, the focus of therapy should be on identifying and correcting the underlying cause of hyponatraemia. If hypovolemic on the basis of clinical assessment and urine sodium concentration, normal saline solution should be administered initially to correct the extracellular fluid volume deficit. If hypervolemic, salt and water restriction is key. If euvolemic and hyponatremic, therapy consists primarily of water restriction. When the cause of the syndrome of inappropriate ADH is unknown or not treatable, other methods can be used, including increased dietary protein and salt and use of urea, loop diuretics and, rarely, demeclocycline hydrochloride (Declomycin).
..")
49
Treatment of Hyponatraemia In symptomatic patients: Patients with acute symptomatic hyponatremia are candidates for aggressive treatment Hyponatremia can be corrected with administration of hypertonic saline solution (3%) at a rate of about 1 mL/kg per hour. A loop diuretic may be added to enhance water excretion if urine osmolality is greater than 300 mOsm/kg. The serum sodium concentration should be raised no more than 25 mEq/L in the first 48 hours, at a rate of no more than 2 mEq/L per hour, and the target goal should be 120 to 125 mEq/L. With use of this combination therapy, sodium lost in the urine is replaced with an equal amount of sodium in a smaller volume. Treatment with hypertonic saline solution is advocated only for patients with severe hyponatremia who have profound neurologic symptoms.

50
Case Study : An elderly lady of 63yrs. Undergoes a difficult resection- anastomosis for a gangrenous segment of small intestine, which was incarcerated under a post-operative band. Her abdomen is distended, she is obtunded, and her bowel sounds are absent. The tongue is red and swollen, skin turgor is diminished and she is not totally coherent. She has mild orthostatic hypotension 1

51
Case Study : Serum sodium- 158mmol/liter Serum Potassium- 4.0mmol/liter Body weight is 60kg. Straight X-ray CT Scan

52
TYPES OF HYPERNATRAEMIA In general, hypernatremia is due to too little water, too much salt, or a combination thereof. H2OH2O Na H2OH2O H2OH2O

53
THUMB RULE:- Serum sodium levels of more than 190 mEq/L usually indicate long-term salt ingestion. Serum sodium levels of more than 170 mEq/L usually indicate DI. Serum sodium levels of more than 150-170 mEq/L usually indicate dehydration.

54
Hypovolemic hypernatremia (ie, water deficit >sodium deficit) Extrarenal losses - Diarrhea, vomiting, fistulas, significant burns Renal losses - Osmotic diuretics, diuretics, postobstructive diuresis, intrinsic renal disease Adipsic hypernatremia is secondary to decreased thirst. This can be behavioral or, rarely, secondary to damage to the hypothalamic thirst centers. H2OH2O Na

55
Hypervolemic hypernatremia (ie, sodium gains >water gains) Hypertonic saline Sodium bicarbonate administration Accidental salt ingestion Mineralocorticoid excess (Cushing syndrome) H2OH2O Na
 Hypertonic saline Sodium bicarbonate administration Accidental salt ingestion Mineralocorticoid excess (Cushing syndrome) H2OH2O Na")
56
Euvolemic hypernatremia Extrarenal losses - Increased insensible loss (eg, hyperventilation) Renal losses - Central DI, nephrogenic DI These patients appear euvolemic because most of the free water loss is from intracellular and interstitial spaces, with less than 10% occurring from intravascular space. Typically, symptoms result if serum sodium is more than 160-170 mEq/L. H2OH2O Na

57
Adipsic hypernatremia differential diagnosis Vascular (15%) - Anterior communicating artery aneurysm or postligation syndrome, intrahypothalmic hemorrhage, internal carotid artery ligation Neoplastic (50%) - Primary or metastatic Granuloma (20%) - Histiocytosis X, sarcoidosis Miscellaneous (15%) - Hydrocephalus, ventricular cyst, trauma, idiopathic
 - Anterior communicating artery aneurysm or postligation syndrome, intrahypothalmic hemorrhage, internal carotid artery ligation Neoplastic (50%) - Primary or metastatic Granuloma (20%) - Histiocytosis X, sarcoidosis Miscellaneous (15%) - Hydrocephalus, ventricular cyst, trauma, idiopathic")
58
Central DI differential diagnosis Head trauma Posthypophysectomy Suprasellar or intrasellar tumors Granulomas (sarcoidosis, Wegener granulomatosis, tuberculosis, syphilis) Histocytosis (eosinophilic granuloma) Infectious (encephalitis, meningitis, Guillain-Barré syndrome) Vascular (cerebral aneurysm, thrombosis, hemorrhage, Sheehan syndrome) Congenital
 Histocytosis (eosinophilic granuloma) Infectious (encephalitis, meningitis, Guillain-Barré syndrome) Vascular (cerebral aneurysm, thrombosis, hemorrhage, Sheehan syndrome) Congenital")
59
Nephrogenic DI (deficient renal response to ADH) differential diagnosis Advanced renal disease (interstitial disease) Electrolyte disturbances - Hypokalemia, hypercalcemia Systemic diseases - Sickle cell disease, Sjögren syndrome, amyloidosis, Fanconi syndrome, sarcoidosis, renal tubular acidosis, light chain nephropathy Dietary disturbances - Excessive water intake, decreased salt intake, decreased protein intake Drugs - Lithium, demeclocycline, colchicine, vinblastine, amphotericin B, gentamicin, furosemide, angiographic dyes, osmotic diuretics Miscellaneous - Postobstructive diuresis, diuretic phase of acute renal failure, osmotic diuresis, paroxysmal hypertension
 differential diagnosis Advanced renal disease (interstitial disease) Electrolyte disturbances - Hypokalemia, hypercalcemia Systemic diseases - Sickle cell disease, Sjögren syndrome, amyloidosis, Fanconi syndrome, sarcoidosis, renal tubular acidosis, light chain nephropathy Dietary disturbances - Excessive water intake, decreased salt intake, decreased protein intake Drugs - Lithium, demeclocycline, colchicine, vinblastine, amphotericin B, gentamicin, furosemide, angiographic dyes, osmotic diuretics Miscellaneous - Postobstructive diuresis, diuretic phase of acute renal failure, osmotic diuresis, paroxysmal hypertension")
60
Effect of Hypernatraemia and its correction Normal brain Hypertonic state Waterloss Rapid adaptation Acc. of electro- lytes Slow adaptation Acc. Of organic osmolytes PROPER CORRECTION IMPROPER CORRECTION CEREBRAL OEDEMA Water

61
Treatment of Hypernatraemia Treatment Same general principles as that of hyponatremia. Rapid correction should be avoided because of the brain's adaptive response to hypernatremia and the potential risk of cerebral edema. The current recommendation is to lower the serum sodium concentration by about 0.5 mEq/L per hour and to replace no more than half the water deficit in the first 24 hours. The following formula can be used to calculate the water deficit (total body water, in kilograms, is 60% of lean body mass in men and 50% in women): Water deficit = total body water (serum sodium concentration ÷ 140 - 1)
: Water deficit = total body water (serum sodium concentration ÷ ).")
62
Treatment of Hypernatraemia In hypovolemic hypernatremia, normal saline solution is indicated initially to correct the intravascular volume deficit. When that is accomplished, more hypotonic fluids (eg, 50% normal saline) can be used. In hypervolemic hypernatremia, removing the source of salt excess, administering diuretics, and replacing water are important to successful therapy. In euvolemic hypernatremia usually require water replacement alone--either free water orally or an infusion of 5% dextrose in water.
 can be used. In hypervolemic hypernatremia, removing the source of salt excess, administering diuretics, and replacing water are important to successful therapy. In euvolemic hypernatremia usually require water replacement alone--either free water orally or an infusion of 5% dextrose in water..")
63
HYPERNATRAEMIA

64
Case Study : A 70 yr old poorly controlled diabetic lady presented with features of peritonitis. A straight X -ray showed the following. The 1st post-operative day found her delirious, oliguric, with a feeble thready pulse and low blood pressure.She started to retain CO2 and needed to be put on ventilation. 2

65
Case Study : BLOOD RESULTS Blood Sugar -768mgm%. Serum Potassium-4.5mmol/L Serum Sodium- 138mmol/L Serum Creatinine-1.8ugm/dl Serum Osmolality-360mmol/L Urine-no ketone bodies TREATMENT:- 1)Large amounts of fluids to rapidly establish circ. And urinary flow. 2)Insulin for rapid corretion of hyperglycaemia. 3)Potassium to replenish intracellular shifts.
Large amounts of fluids to rapidly establish circ. And urinary flow. 2)Insulin for rapid corretion of hyperglycaemia. 3)Potassium to replenish intracellular shifts..")
66
USEFUL FORMULAS

67
MICROSCOPIC ANATOMY OF THE NEPHRON

68
FUNCTION OF THE KIDNEY -and the action of diuretics. 1) Proximal tubule-osmotic diuresis. 2) Ascending limb of the loop of Henle-reduction of Na reabsorption(K loss at 4). 3) Cortical diluting segment- reduction of Na reabsorption(K loss at 4). 4) Distal tubule-inhibition of Na exchange with K,H- aldosterone antagonism/independent. CORTEX MEDULLA Na;Cl; NaHCO 3 H2OH2O H2OH2O Na;Cl Na K;H H2OH2O Na
 Proximal tubule-osmotic diuresis. 2) Ascending limb of the loop of Henle-reduction of Na reabsorption(K loss at 4). 3) Cortical diluting segment- reduction of Na reabsorption(K loss at 4). 4) Distal tubule-inhibition of Na exchange with K,H- aldosterone antagonism/independent. CORTEX MEDULLA Na;Cl; NaHCO 3 H2OH2O H2OH2O Na;Cl Na K;H H2OH2O Na.")
69
Site of Action of Diuretics 1) Proximal tubule and descending limb of the Loop of Henle-osmotic diuresis. 2) Proximal tubule – Carbonic anhydrase inhibitors 3) Thick ascending limb of the loop of Henle- loop diuretics 4) Distal tubule- thiazide diuretics and potassium-sparing diuretics.
 Proximal tubule – Carbonic anhydrase inhibitors 3) Thick ascending limb of the loop of Henle- loop diuretics 4) Distal tubule- thiazide diuretics and potassium-sparing diuretics..")
70
A 62 year old man, presents with painless,profuse projectile vomiting containing old food material No history of any previous surgery, he complains of a long standing, mild Epigastric pain. On Examination; the patient had a BP of 100/60;Pulse110/min.Eyes shrunken, Decreased skin turgor, slow to questions, decreased tendon reflexes, a scaphoid abdomen with a visible peristalsis moving from left to right, no free fluid or lump in the abdomen. Barium meal X-ray showed the following Case Study: 3

71
Upper GI Endoscopy Revealed the following finding. Pylorus

72
Case Study : Blood tests.

73
Composition of Different Intestinal Juices SecretionsNaKClHCO 3 Volume Saliva 2-1020-308-18300.5-2L Gastric 9-1160-308-1540-150.1-4L Duodenum 1405800.1-2L Ileum 80-1502-845-137300.1-0.9L Colon 603040 Pancreas 115-1853-755-951150.1-0.8L Bile 130-1603-1290-180350.05-0.8L Stool 357020 Diarrhoea 30-14030-707320-80 Mixed G A 12010100

74
Principle of Hypokalaemia Direct potassium losses contribute only minimally to actual loss. Loss of gastric acid leads to metabolic alkalosis which increases tubular cell potassium concentration. Elevated plasma bicarbonate leads to increased bicarb to distal nephron, leading to an augmentation of potassium loss. Secondary aldosteronism augments potassium excretion Hypokalaemia-induces the excretion of H+ ions in place of K+ ions- PARADOXIC ACIDURIA

75
Case Study : A 32yr. old man presented with a history of severe diarrhoea, occasionally blood stained, with a history of rapid weight loss and severe weakness. His father and uncle had apparently some “bowel problems” for which they were both operated. Examination showed signs of dehydration, with diminished muscle tone and reflexes. His abdomen was slightly distended with diminished peristaltic sounds.

76
Case study -Blood results Haemoglobin- 8.2mgm% TLC- normal Urea- 57mgm/dl Creatinine-0.9ugm/dl Sodium- 130mmol/L Potassium-2.5mmol/L Bicarbonate-13mmol/L

77
Case study -investigations. FAP with diarrhea causing HYPOKALAEMIA

78
oRenal tubular acidosis oHyperaldosteronism oMagnesium depletion oLeukemia (mechanism uncertain ) oVomiting or nasogastric suctioning oDiarrhea oEnemas or laxative use oIleal loop oDiuretics (most common cause) oBeta-adrenergic agonists oSteroids oTheophylline oAminoglycosides oInsulin oAlkalosis Malnutrition or decreased dietary intake, parenteral nutrition
 oVomiting or nasogastric suctioning oDiarrhea oEnemas or laxative use oIleal loop oDiuretics (most common cause) oBeta-adrenergic agonists oSteroids oTheophylline oAminoglycosides oInsulin oAlkalosis Malnutrition or decreased dietary intake, parenteral nutrition")
79
HYPOKALAEMIA

80
10% 350mEq 90% 3150mEq LOSS URINE (90-95mEq/D) STOOL (5-10mEq/D) SWEAT (<5mEq/D) 3.5-5mEq/L140-150mEq/L Bone 300mEq (8.6%) Urine 90-95mEq/L(1%) Interstitial fluid 35mEq/L(0.4%) Muscle 2650 mEq/L(76%) Liver 250mEq/L(7%) RBC 250mEq/L(7%)
 STOOL (5-10mEq/D) SWEAT (<5mEq/D) 3.5-5mEq/L mEq/L Bone 300mEq (8.6%) Urine 90-95mEq/L(1%) Interstitial fluid 35mEq/L(0.4%) Muscle 2650 mEq/L(76%) Liver 250mEq/L(7%) RBC 250mEq/L(7%)")
81
ACIDOSIS ALKALOSIS INSULIN GLUCAGON Beta-ADRENERGIC Alpha-ADRENERGIC ALDOSTERONE EXERCISE

82
EXTRARENAL POTASSIUM HOMEOSTASIS

83
RENAL POTASSIUM HANDLING 100% 30% 50% 140% 30% 50% 10-15%

84
EFFECT OF HYPOKALAEMIA muscle weakness & muscle cramping, paralytic ileus hypoventilation paralysis and respiratory failure hypotension, tetany, and rhabdomyolysis cardiac effects of hypokalemia-- -- premature ventricular and atrial contractions, ventricular and atrial tachyarrhythmias, and second or third degree atrioventricular block. ECG CHANGES ARE:- The characteristic ECG changes of ST segment depression, increased U-wave amplitude, and T-wave amplitude less than U-wave amplitude (in the same lead)
.")
85
TREATMENT Prehospital Care: Be attentive to the ABCs. If the patient is severely bradycardic or manifesting cardiac arrhythmias, appropriate pharmacologic therapy or cardiac pacing should be considered. Emergency Department Care: Patients in whom severe hypokalemia is suspected should be placed on a cardiac monitor; establish intravenous (IV) access and assess respiratory status. Direct potassium replacement therapy by the symptomatology and the potassium level. Usually, patients who have mild or moderate hypokalemia (potassium of 2.5-3.5 mEq/L), are asymptomatic, or have only minor symptoms need only oral potassium replacement therapy unless cardiac arrhythmias or significant symptoms are present. This treatment is similar to the treatment for severe hypokalemia. If the potassium level is less than 2.5 mEq/L, IV potassium should be given. Admission or ED observation is indicated; replacement therapy takes more than a few hours. Serum potassium is difficult to replenish if serum magnesium is also low. Look to replace both.
 access and assess respiratory status. Direct potassium replacement therapy by the symptomatology and the potassium level. Usually, patients who have mild or moderate hypokalemia (potassium of mEq/L), are asymptomatic, or have only minor symptoms need only oral potassium replacement therapy unless cardiac arrhythmias or significant symptoms are present. This treatment is similar to the treatment for severe hypokalemia. If the potassium level is less than 2.5 mEq/L, IV potassium should be given. Admission or ED observation is indicated; replacement therapy takes more than a few hours. Serum potassium is difficult to replenish if serum magnesium is also low. Look to replace both..")
86
Treatment of Hypokalaemia If K + is between 2.5 - 3.5 mmol/L & no symptoms of hypokalaemia use oral K + supplements, at least 80mmol/24 hours normal maximum daily oral dose is 100mmol/l may cause nausea, vomiting and GI ulceration K + must be closely monitored and supplements stopped when K + > 4.0 mmol/l

87
Treatment of Hypokalaemia If K + is < 2.5 mmol/l and a clinical decision is made to treat with IV Potassium Use IV potassium either centrally or peripherally. Ready-made potassium containing infusion bags should be prescribed and administered, unless there is a specific indication to do otherwise A syringe pump may be used for central line administration. All patients treated with IV potassium should have at least once daily measurement of serum potassium until levels are shown to be satisfactory

88
Treatment of Hypokalaemia Peripheral Line IV Administration Rate of Administration 10mmol/hour Maximum 20mmol/hour with ECG monitoring Maximum Concentration 40mmol/l Phlebitis may occur at concentrations > 30mmol/l Central Line IV administration Rate of Administration 10mmol/hour Maximum 20mmol/hour with ECG monitoring Maximum Concentration Can give undiluted KCL 2mmol/ml at a rate of 10-20mmol/hr via a syringe driver with appropriate ECG monitoring

89
Caution!! Strong Potassium Chloride Solution: restricted to ICU,CICU,CCU 10ml (20mmol) must be diluted to at least 500ml for peripheral administration dilute with sodium chloride 0.9% MIX WELL (otherwise, potassium chloride being heavier than the usual diluents will sink to the bottom if not mixed sufficiently and be given in effect undiluted as a bolus; this can be fatal)
 must be diluted to at least 500ml for peripheral administration dilute with sodium chloride 0.9% MIX WELL (otherwise, potassium chloride being heavier than the usual diluents will sink to the bottom if not mixed sufficiently and be given in effect undiluted as a bolus; this can be fatal).")
90
Case Study : An 62 yrs old farmer, sustained a crush injury to both his legs due to a tractor injury He was admitted at a peripheral hospital for 3 days before being transferred to the referral center. On examination he was found to have a thready irregular pulse, hypotension, was oliguric. The crush injury to both his legs were severe, with absent peripheral pulses with a compound injury to the right leg and a compartment syndrome of the left leg. In the past, the only relevent history was that of long standing small joint arthritis for which the patient had been on NSAIDS. 4

91
Case Study: Urea-112mgm/ Creatinine-2.2ugm Na-138mmol/l K-7.4mmol/l Hb-7.6mgm/dl TLC-15600; N 86 X-Ray-bilateral comm.# tib/fib ECG CAUSE: HYPERKALAEMIA(muscle damage+NSAIDS)
")
92
CAUSES OF HYPERKALAEMIA Excessive potassium intake alone is an uncommon cause of hyperkalemia renal failure drugs that interfere with potassium excretion angiotensin- convening enzyme inhibitor NSAIDs type IV renal tubular acidosis rhabdomyolysis tumor lysis insulin deficiency acute acidosis.

93
Treatment of Hyperkalaemia Emergency treatment of hyperkalemia is targeted towards one of three objectives: Antagonizing calcium, eg Calcium Chloride administration Causing potassium to shift into cells, eg with administration of sodium bicarbonate, insulin + glucose, or nebulized albuterol Removing potassium from the body, eg with diuresis with a non-potassium-sparing diuretic, administration of cation exchange resin, or dialysis

94
Treatment of Hyperkalaemia

95
HYPERKALAEMIA

96
A 8-year-old male child presented with swelling neck right side since last 2 months. There were no other significant complaints. USG neck showed a hypoechoic nodule of size 23x14mm in the inferior portion of right lobe of thyroid and was highly suspicious of neoplastic lesion. Corroborated by the CT Scan. Thyroid profile was within normal limits. FNAC of thyroid swelling revealed to be a case of papillary carcinoma. Case Study 5

97
Patient was taken up for total thyroidectomy. On exploration, it was observed that the area surrounding the thyroid was also infiltrated by the tumour and was unseparable from the thyroid mass. Hence, parathyroid glands were also removed alongwith the lymph nodes of jugular chain. Histopathological examination confirmed the diagnosis of PTC infiltrating the parathyroid with lymph node metastasis. WHAT ARE THE PRECAUTIONS YOU WOULD WARN THE NURSING STAFF ABOUT AND WHAT WOULD YOU EXPECT THEM TO LOOK FOR?

98
CAUSES OF HYPOCALCAEMIA Hypoparathyroidism Severe pancreatitis Renal failure Massive blood transfusion Sepsis Alkalosis.

100
Vit D Metabolism

101
Treatment of hypocalcaemia Airway must be secured. Oxygen by mask. ECG monitoring while treatment is progressing. 10-20 ml of 10% Calcium gluconate IV slowly. Then 40ml of 10% Calcium Gluconate in 500 ml Saline in the next 4-8hrs. Oral Calcium and Vitamin D or its metabolites

102
Treatment of Hypocalcaemia Acute Hypocalcemia The patient with acute hypocalcemia may have symptoms of tetany seizure, or laryngeal spasm requiring aggressive treatment with intravenous calcium administration. Calcium gluconate given IV 1 to 2 ampules (180 mg of elemental calcium) diluted in 50 to 100 mL of 5% dextrose is infused over 10 minutes. This can be repeated until the patient's symptoms have cleared. This can be repeated until the patient's symptoms have cleared. The goals should be to raise serum calcium by 2 to 3 mg/dL with the administration of 15 mg/kg of elemental calcium over 4 to 6 hours. Calcium should be maintained in the low-normal range. If possible, oral calcium supplementation should be initiated concurrently with 1 to 2 grams of elemental calcium and if warranted, 1,25-dihydroxyvitamin D. Chronic Hypocalcemia Patients who are asymptomatic or with mild symptomatic hypocalcemia can be treated with oral calcium and vitamin D. The overall goal of therapy is to maintain serum calcium in the low- normal range. Serum calcium should be tested very 3 to 6 months.
 diluted in 50 to 100 mL of 5% dextrose is infused over 10 minutes. This can be repeated until the patient s symptoms have cleared. This can be repeated until the patient s symptoms have cleared. The goals should be to raise serum calcium by 2 to 3 mg/dL with the administration of 15 mg/kg of elemental calcium over 4 to 6 hours. Calcium should be maintained in the low-normal range. If possible, oral calcium supplementation should be initiated concurrently with 1 to 2 grams of elemental calcium and if warranted, 1,25-dihydroxyvitamin D. Chronic Hypocalcemia Patients who are asymptomatic or with mild symptomatic hypocalcemia can be treated with oral calcium and vitamin D. The overall goal of therapy is to maintain serum calcium in the low- normal range. Serum calcium should be tested very 3 to 6 months..")
103
Case Study A 38year old female executive has the following complaints:- Loss of energy and feeling old. Can't concentrate and feels depressed, irritable and has insomnia. Bones hurt; particularly the bones in the legs and arms. Has heartburn. Has Recurrent Headaches and Palpitations. PMH oStone in the kidney –treated by ESWL two occasions 6

104
Case study The phalanges are seen to be asymmetrical with subcortical bone resorption on their radial side. A minute examination of the tufts will usually reveal that the continuous line of cortical bone which delinates the tuft is interrupted and the appearance resembles a lace border.

106
Sestamibi scanning Sestamibi is a small protein which is labeled with the radio-pharmaceutical technetium-99. This very mild and safe radioactive agent is injected into the veins of a patient with parathyroid disease and is absorbed by the overactive parathyroid gland. Minimally Invasive Radioguided Parathyroid (MIRP) Surgery
 Surgery.")
108
Treatment of hypercalcaemia Goals of treatment oStabilization and reduction of the calcium level oAdequate hydration oIncreased urinary calcium excretion oInhibition of osteoclast activity in the bone oTreatment of the underlying cause (when possible)
")
109
Calcium balance Calcium balance. On average, in a typical adult approximately 1g of elemental calcium (Ca +2 ) is ingested per day. Of this, about 200mg/day will be absorbed and 800mg/day excreted. Approximately 1kg of Ca +2 is stored in bone and about 500mg/day is released by resorption or deposited during bone formation. Of the 10g of Ca +2 filtered through the kidney per day only about 200mg appears in the urine, the remainder being reabsorbed.
 is ingested per day. Of this, about 200mg/day will be absorbed and 800mg/day excreted. Approximately 1kg of Ca +2 is stored in bone and about 500mg/day is released by resorption or deposited during bone formation. Of the 10g of Ca +2 filtered through the kidney per day only about 200mg appears in the urine, the remainder being reabsorbed..")
110
ECF Ca 2+ Ca 2+ 0.5gm/D Ca 2+ 1Kg Ca 2+ 9.8gm/D Ca 2+ 0.2gm/D Ca 2+ 10gm/D Ca 2+ 0.2gm/D Ca 2+ 1 gm/D Ca 2+ 0.8gm/D URINE CALCIUM METABOLISM

111
ECF CALCIUM ACIDOSIS ALKALOSIS

112
Three types of cell produce and maintain bone. Osteoblasts (bone-forming cells) work at bone surfaces where they secrete osteoid (unmineralised collagen), modulate the crystallisation of hydroxyapatite and influence the activity of osteoclasts. Osteoclasts (bone-resorbing cells) are responsible for the resorption (destruction) of old worn out bone, which is necessary for the repair of bone surfaces and the remodelling of bone. Osteocytes are osteoblasts which have become embedded within the mineralised regions of bone. They are involved in the sensing and translation of information about the internal bone environment.
 work at bone surfaces where they secrete osteoid (unmineralised collagen), modulate the crystallisation of hydroxyapatite and influence the activity of osteoclasts. Osteoclasts (bone-resorbing cells) are responsible for the resorption (destruction) of old worn out bone, which is necessary for the repair of bone surfaces and the remodelling of bone. Osteocytes are osteoblasts which have become embedded within the mineralised regions of bone. They are involved in the sensing and translation of information about the internal bone environment..")
113
Bone turnover cycle

114
Stages of bone fracture healing FRACTURE HEALING PRIMARY SECONDARY SURGICAL RESORATION OF ANATOMY bone-resorbing cells on one side of the fracture show a tunnelling resorptive response, whereby they re-establish new haversian systems by providing pathways for the penetration of blood vessels Impaction stage Remodelling stage Inflammation stage Primary soft callus formation stage Callus mineralisation stage Upto 7 days Two weeks 4 – 16 weeks 1 – 4 years

115
CALCIUM HOMEOSTASIS

116
A. Endocrine Disorders Associated with Hypercalcemia 1.Endocrine Disorders with Excess PTH Production Primary Sporadic hyperparathyroidism Primary Familial Hyperparathyroidism MEN I MEN IIA FHH and NSHPT Hyperparathyroidism - Jaw Tumor Syndrome Familial Isolated Hyperparathyroidism 2. Endocrine Disorders without Excess PTH Production Hyperthyroidism Hypoadrenalism Jansen's Syndrome CAUSES OF HYPERCALCAEMIA

117
B. Malignancy-Associated Hypercalcemia (MAH) 1.MAH with Elevated PTHrP Humoral Hypercalcemia of Malignancy Solid Tumors with Skeletal Metastases Hematologic Malignancies 2. MAH with Elevation of Other Systemic Factors MAH with Elevated 1,25(OH)2D3 MAH with Elevated Cytokines Ectopic Hyperparathyroidism Multiple Myeloma C. Inflammatory Disorders Causing Hypercalcemia 1.Granulomatous Disorders 2.AIDS D. Disorders of Unknown Etiology 1.Williams Syndrome 2.Idiopathic Infantile Hypercalcemia CAUSES OF HYPERCALCAEMIA
 1.MAH with Elevated PTHrP Humoral Hypercalcemia of Malignancy Solid Tumors with Skeletal Metastases Hematologic Malignancies 2. MAH with Elevation of Other Systemic Factors MAH with Elevated 1,25(OH)2D3 MAH with Elevated Cytokines Ectopic Hyperparathyroidism Multiple Myeloma C. Inflammatory Disorders Causing Hypercalcemia 1.Granulomatous Disorders 2.AIDS D. Disorders of Unknown Etiology 1.Williams Syndrome 2.Idiopathic Infantile Hypercalcemia CAUSES OF HYPERCALCAEMIA.")
118
E. Medication-Induced 1.Thiazides 2.Lithium 3.Vitamin D 4.Vitamin A 5.Estrogens and Antiestrogens 6.Aluminium Intoxication 7.Milk-Alkali Syndrome CAUSES OF HYPERCALCAEMIA

119
Drugs in hypercalcaemia Bisphosphonates -- Inhibit bone reabsorption eg. Pamidronate,etidronate. Antineoplastic drugs -- Reduce bone turnover eg gallium nitrate. Antihypercalcemic agents -- Inhibit bone resorption and increase renal calcium excretion eg calcitonin. Glucocorticoids -- Inhibit cytokine release and have a direct cytolytic effect on some tumor cells. Minerals -- Phosphate inhibits calcium absorption and promotes calcium deposition. Calcimimetic agent -- Binds to and modulates the parathyroid calcium-sensing receptor, increases sensitivity to extracellular calcium, and reduces parathyroid hormone secretion eg cinacalcet.

120
HYPERMAGNESAEMIA CAUSE:- Renal failure Medications containing magnesium FEATURES:- oMuscle weakness, Drowsiness oLoss of tendon reflex oECG - PR wide QRS T oDepression of respiratory centre. oMuscle oComa and Cardiac arrest Ca 2+ at synapse ACh at neuromuscular junction

121
HYPERMAGNESAEMIA TREATMENT:- Dialysis Calcium for cardiac arrhythmias. Inducing diuresis – Fluid load(4-5 litres of Saline) or Frusemide (20- 40mgm 8hrly) Adequate Calcium replacement.
 or Frusemide (20- 40mgm 8hrly) Adequate Calcium replacement..")
122
HYPOMAGNESAEMIA CAUSES:- Prolonged TPN GI losses – High output fistulae Alcoholism- Decreased tubular resorption Diuretics. FEATURES:- o NM Excitability( transmitter release) o Irregular tremors o Irritability o ECG- ST, T inversion, QT (Hypokalaemia) TREATMENT :- Magnesium Sulphate or Chloride ---- 30-50 mmols in 1 L of 5%Dextrose/24 hrs.
 o Irregular tremors o Irritability o ECG- ST, T inversion, QT (Hypokalaemia) TREATMENT :- Magnesium Sulphate or Chloride mmols in 1 L of 5%Dextrose/24 hrs..")
123
IMPORTANT FORMULA Trans tubular K+ concentration gradient (TTKG)Am. J. Kidney Dis. 24;597,1994. TTKG = ([K+]u x OSMp) ([K+]p x OSMu) The urine osmolality MUST exceed that of plasma in order to calculate an interpretable TTKG.
 ([K+]p x OSMu) The urine osmolality MUST exceed that of plasma in order to calculate an interpretable TTKG..")
124
INTERPRETATION OF BLOOD GASES ‘NORMAL’ BLOOD GASES pH7.35 – 7.45 PaO 2 13kPa PaCO 2 5.3kPa HCO 3 22 – 25mmol/l Base deficit or excess -2 to +2 mmol/l

125
INTERPRETING BLOOD GASES Look at the PaO 2. Is the patient hypoxaemic? What is the A-a gradient {Alveolar - Arterial oxygen difference (A-a)DO 2 } (A-a)DO 2 = FiO 2 x (atmospheric pressure – SVP of water) – PaCO 2 – PaO 2. (A-a)DO 2 =(FiO 2 x{101-6.2}-PaCO 2 -PaO 2 SCORE+4+3+2+10 RESULT>66.646.7- 66.5 26.7- 46.5 <26.7 APACHE
DO 2 } (A-a)DO 2 = FiO 2 x (atmospheric pressure – SVP of water) – PaCO 2 – PaO 2. (A-a)DO 2 =(FiO 2 x{ }-PaCO 2 -PaO 2 SCORE RESULT> <26.7 APACHE.")
126
INTERPRETING BLOOD GASES Look at the PaCO 2. Look at the pH. Alkalotic or Acidic?

127
INTERPRETING BLOOD GASES cPaCO 2 = pH SBE = pH cPaCO 2 = pH SBE = pH ‘NORMAL’ BLOOD GASES pH7.35 – 7.45 PaO 2 13kPa PaCO 2 5.3kPa HCO 3 22 – 25mmol/l Base deficit or excess -2 to +2 mmol/l

128
Respiratory acidosis Background: Respiratory acidosis is a clinical disturbance that is due to alveolar hypoventilation. Production of carbon dioxide occurs rapidly, and failure of ventilation promptly increases the partial arterial pressure of carbon dioxide (PaCO2). The reference range for PaCO2 is 36-44. Alveolar hypoventilation leads to an increased PaCO2 (ie, hypercapnia). The increase in PaCO2 in turn decreases the HCO3-/PaCO2 and decreases pH. What are the types of Respiratory Failure?
. The reference range for PaCO2 is Alveolar hypoventilation leads to an increased PaCO2 (ie, hypercapnia). The increase in PaCO2 in turn decreases the HCO3-/PaCO2 and decreases pH. What are the types of Respiratory Failure .")
129
RESPIRATORY FAILURE TYPE I FAILURE HYPOXIC PaO2 < 8kPa NORMAL OR LOW PaCO2 Impaired alveolar function; pneumonia,pulmonary oedema; ARDS TYPE II FAILURE HYPERCAPNIC PaO2 <8kPa PaCO2 > 8kPa Impaired alveolar ventilation; COPD, airway impairment,chest wall deformity, neuromuscular conditions

130
Compensation in Respiratory acidosis In acute respiratory acidosis, compensation occurs in 2 steps. The initial response is cellular buffering that occurs over minutes to hours. Cellular buffering elevates plasma bicarbonate (HCO3-) only slightly, approximately 1 mEq/L for each 10-mm Hg increase in PaCO2. In chronic respiratory acidosis, the second step is renal compensation that occurs over 3-5 days. With renal compensation, renal excretion of carbonic acid is increased and bicarbonate reabsorption is increased. In renal compensation, plasma bicarbonate rises 3.5 mEq/L for each increase of 10 mm Hg in PaCO2.
 only slightly, approximately 1 mEq/L for each 10-mm Hg increase in PaCO2. In chronic respiratory acidosis, the second step is renal compensation that occurs over 3-5 days. With renal compensation, renal excretion of carbonic acid is increased and bicarbonate reabsorption is increased. In renal compensation, plasma bicarbonate rises 3.5 mEq/L for each increase of 10 mm Hg in PaCO2..")
131
Respiratory acidosis The expected change in serum bicarbonate concentration in respiratory acidosis can be estimated as follows: Acute respiratory acidosis: HCO 3 - increases 1 mEq/L for each 10-mm Hg rise in PaCO 2. Chronic respiratory acidosis: HCO 3 - rises 3.5 mEq/L for each 10-mm Hg rise in PaCO 2.

132
Respiratory alkalosis Respiratory alkalosis is a clinical disturbance due to alveolar hyperventilation. Alveolar hyperventilation leads to a decreased PaCO2 level (hypocapnia). In turn, the decrease in PaCO 2 level increases the ratio of bicarbonate concentration (HCO 3 - ) to PaCO 2 and increases the pH level. Hypocapnia develops when the lungs remove more carbon dioxide than is produced in the tissues.
. In turn, the decrease in PaCO 2 level increases the ratio of bicarbonate concentration (HCO 3 - ) to PaCO 2 and increases the pH level. Hypocapnia develops when the lungs remove more carbon dioxide than is produced in the tissues..")
133
Respiratory alkalosis Respiratory alkalosis can be acute or chronic. In acute respiratory alkalosis, the PaCO2 level is below the lower limit of normal and the serum level is alkalemic. In chronic respiratory alkalosis, the PaCO2 level is below the lower limit of normal, but the pH level is normal or near normal because of renal compensation.

134
Respiratory alkalosis Acute hyperventilation with hypocapnia causes a small early reduction in serum bicarbonate due to cellular uptake of bicarbonate. Acutely, plasma pH and bicarbonate concentration vary proportionately with the PaCO2 along a range of 15-40 mm Hg. After a period of 2-6 hours, respiratory alkalosis is compensated by the kidneys by a decrease in bicarbonate reabsorption.

135
Respiratory alkalosis The expected change in serum bicarbonate concentration ([HCO 3 - ]) can be estimated as follows: Acute - [HCO 3 - ] falls 2 mEq/L for each decrease of 10 mm Hg in the PaCO 2 (Limit of compensation: [HCO 3 - ] = 12-20 mEq/L) Chronic - [HCO 3 - ] falls 5 mEq/L for each decrease of 10 mm Hg in the PaCO 2 (Limit of compensation: [HCO 3 - ] = 12-20 mEq/L)
![Respiratory alkalosis The expected change in serum bicarbonate concentration ([HCO 3 - ]) can be estimated as follows: Acute - [HCO 3 - ] falls 2 mEq/L for each decrease of 10 mm Hg in the PaCO 2 (Limit of compensation: [HCO 3 - ] = mEq/L) Chronic - [HCO 3 - ] falls 5 mEq/L for each decrease of 10 mm Hg in the PaCO 2 (Limit of compensation: [HCO 3 - ] = mEq/L)](http://images.slideplayer.com/12/3451651/slides/slide_135.jpg "Respiratory alkalosis The expected change in serum bicarbonate concentration ([HCO 3 - ]) can be estimated as follows: Acute - [HCO 3 - ] falls 2 mEq/L for each decrease of 10 mm Hg in the PaCO 2 (Limit of compensation: [HCO 3 - ] = mEq/L) Chronic - [HCO 3 - ] falls 5 mEq/L for each decrease of 10 mm Hg in the PaCO 2 (Limit of compensation: [HCO 3 - ] = mEq/L)")
136
CONTROL OF VENTILATION CORTICO-SPINAL TRACT

137
REGULATION OF VENTILATION CHEMICAL CONTROL 1.CO2 - via CSF H + CONCENTRATION 2.O2 - via CAROTID AND AORTIC BODIES 3.H+ - via CAROTID AND AORTIC BODIES NON CHEMICAL CONTROL 1.Afferents from Pons, Hypothalamus & Limbic System. 2.Afferent from Proprioceptors. 3.Afferents from pharynx, trachea & bronchi. 4.Vagal efferents from inflation/ deflation receptors in lung. 5.Afferents from baroreceptors: arterial, atrial, ventricular & pulmonary.

138
INTERPRETING BLOOD GASES cPaCO 2 = pH SBE = pH cPaCO 2 = pH SBE = pH ‘NORMAL’ BLOOD GASES pH7.35 – 7.45 PaO 2 13kPa PaCO 2 5.3kPa HCO 3 22 – 25mmol/l Base deficit or excess -2 to +2 mmol/l

139
METABOLIC CHANGES ACIDOSIS EFFFECTS OF METABOLIC ACIDOSIS oIncreased respiratory drive (?){pH <7.1}. oDecreased response to inotropes. oH + ions into cells and K + out as buffering action. oHyperkalaemia.

140
ANION GAP The formula (Anion Gap = Na + - HCO3 - - Cl - ). Also important to define the TYPE of metabolic acidosis.

141
METABOLIC CHANGES CAUSES OF METABOLIC ACIDOSIS Accumulation of H+ Anion gap > 8 mmols/l Loss of bicarbonate Anion gap < 8mmols/l KetoacidosisVomiting /diarrhoea Lactic acidosisSmall bowel fistula ARFRenal tubular acidosis Salicylate poisoning Calculating NaHCO3 = ½ x base deficit(mmols/l x weight(kg) 3 Very rarely needed!!!!! Anion Gap = Na + - (HCO3 - + Cl - )
.")
142
COMPENSATORY MECHANISMS 1.BLOOD - Buffers. 2.RESPIRATORY – increased ventilation – CO 2 blown off. 3.KIDNEYS – HCO 3 secreted all reabsorbed.

143
BUFFERS IN BLOOD Plasma proteins. Imidazole groups of the histidine residues of haemoglobin. Carbonic acid bicarbonate system. Phosphate system (intracellular) Therefore use of bicarbonate only for the pH < 7.2 in an inotrope resistant hypotensive patient
 Therefore use of bicarbonate only for the pH < 7.2 in an inotrope resistant hypotensive patient.")
144
METABOLIC CHANGES ALKALOSIS EFFFECTS OF METABOLIC ALKALOSIS oReduced respiratory drive. oH+ ions out of cells and K+ in as buffering action. oHypokalaemia. oHypocalcaemia – tetany, paresthesia

145
COMPENSATORY MECHANISMS 1.RESPIRATORY – Reduced respiration = retention of CO 2 = increased H + 2.RENAL – Increased HCO 3 excretion

146
RELATION BETWEEN BASE EXCESS AND pCO2 Whenever the pH is normal, i.e., pH = 7.4. then the PCO2 and the SBE are equal and opposite. In such circumstances, if the PCO2 is described as a marked acidosis then logically the SBE must be the exact opposite, a marked alkalosis. Fortunately, the slope for BE/PCO2 when ph = 7.4 gives us this ratio: three units of change in the SBE is equivalent to a five mmHg change in the PCO2. Thus, (change in) pCO 2 : (change in) SBE = 5:3 chpCO 2 /chSBE=5/3
 pCO 2 : (change in) SBE = 5:3 chpCO 2 /chSBE=5/3.")
147
INTERPRETING BLOOD GASES cPaCO 2 = pH SBE = pH cPaCO 2 = pH SBE = pH ‘NORMAL’ BLOOD GASES pH7.35 – 7.45 PaO 2 13kPa PaCO 2 5.3kPa HCO 3 22 – 25mmol/l Base deficit or excess -2 to +2 mmol/l

148
INTERPRETATION OF BLOOD GASES ‘NORMAL’ BLOOD GASES pH7.35 – 7.45 PaO 2 13kPa PaCO 2 5.3kPa HCO 3 22 – 25mmol/l Base deficit or excess -2 to +2 mmol/l

149
EXAMPLES Example A: pH = 7.2, PCO2 = 60 mmHg, SBE = 0 mEq/L Overall change is acid. Respiratory change is also acid - therefore contributing to the acidosis. SBE is normal - no metabolic compensation. Therefore, pure respiratory acidosis. Typical of acute respiratory depression. Magnitude: marked respiratory acidosis

150
EXAMPLES Example B: pH = 7.35, PCO2 = 60 mmHg, SBE = 7 mEq/L Overall change is slightly acid. Respiratory change is also acid - therefore contributing to the acidosis. Metabolic change is alkaline - therefore compensatory. The respiratory acidosis is 20 mmHg on the acid side of normal (40). To completely balance plus 20 would require 20 X 3 / 5 = 12 mEq/L SBE The actual SBE is 7 eEq/L, which is roughly half way between 0 and 12, i.e., a typical metabolic compensation. The range is about 6mEq/L wide - in this example between about 3 and 9 mEq/L. Magnitude: marked respiratory acidosis with moderate metabolic compensation
. To completely balance plus 20 would require 20 X 3 / 5 = 12 mEq/L SBE The actual SBE is 7 eEq/L, which is roughly half way between 0 and 12, i.e., a typical metabolic compensation. The range is about 6mEq/L wide - in this example between about 3 and 9 mEq/L. Magnitude: marked respiratory acidosis with moderate metabolic compensation.")
151
EXAMPLES Example C: pH = 7.15, PCO2 = 60 mmHg, SBE = -6 mEq/L Overall change is acid. Respiratory change is acid - therefore contributing to the acidosis. Metabolic change is also acid - therefore combined acidosis. The components are pulling in same direction - neither can be compensating for the other Magnitude: marked respiratory acidosis and mild metabolic acidosis

152
EXAMPLES Example D: pH = 7.30, PCO2 = 30 mmHg, SBE = -10 mEq/L Overall change is acid. Respiratory change is alkaline - therefore NOT contributing to the acidosis. Metabolic change is acid - therefore responsible for the acidosis. The components are pulling in opposite directions. SBE is the acid component so it is primarily a metabolic problem with some respiratory compensation The metabolic acidosis is 10 mEq/L on the acid side of normal (0). To completely balance 10 would require 10 * 5 / 3 = 17 mmHg respiratory alkalosis (= 23 mmHg) The actual PCO2 is 30 eEq/L which is roughly half way between 23 and 40, i.e., a typical respiratory compensation. The range is about 10 mmHg wide - in this example between about 27 and 37 mmHg. Magnitude: marked metabolic acidosis with mild respiratory compensation.
. To completely balance 10 would require 10 * 5 / 3 = 17 mmHg respiratory alkalosis (= 23 mmHg) The actual PCO2 is 30 eEq/L which is roughly half way between 23 and 40, i.e., a typical respiratory compensation. The range is about 10 mmHg wide - in this example between about 27 and 37 mmHg. Magnitude: marked metabolic acidosis with mild respiratory compensation..")
153
“All’s well that ends well” To ensure that your per-op. Care,matches, nay, exceeds your operation.

154
GOOD SURGERY BUT BAD MANAGEMENT!!

Similar presentations





















 Newborn (77%) Adult male (60%) Adult female (54%) Elderly (45%) Adipose.>")
