Download presentation
Presentation is loading. Please wait.

1
APPROACH TO CYANOSIS

2
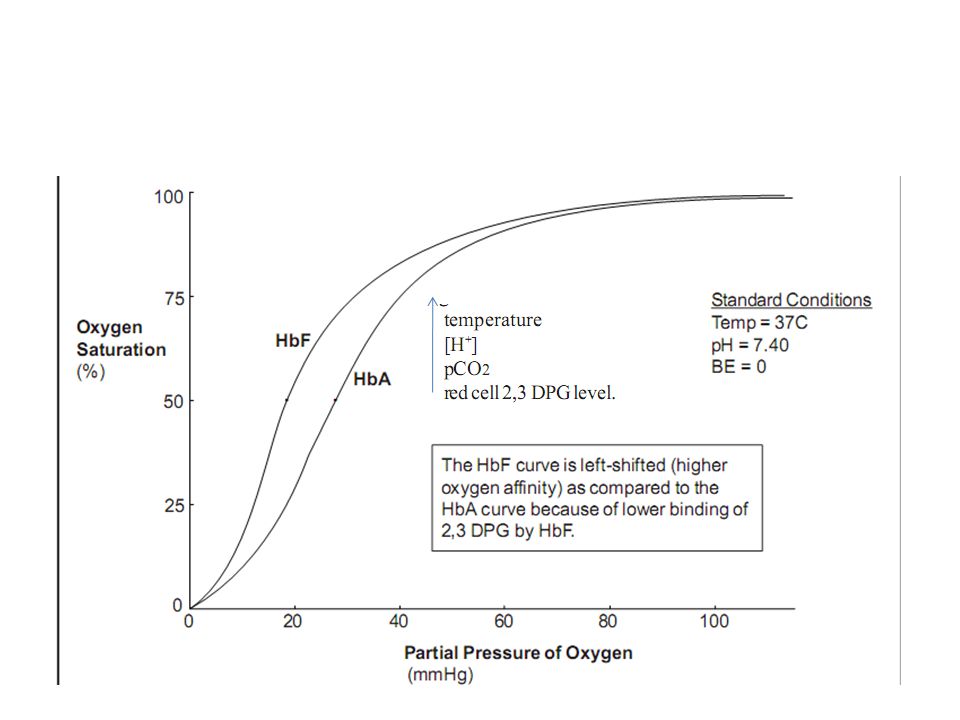
Definition Bluish discolouration of skin or mucous membrane caused by excess amounts of reduced hemoglobin or abnormal hemoglobin 4gm of reduced Hb in capillaries required for cyanosis to be apparent

3
Mechanism caused by absolute increase in reduced Hb,higher the Hb – greater tendancy towards cyanosis

4
In severe anemia , greater systemic arterial desaturation required for cyanosis to be evident
In polycythemia even lesser systemic arterial oxygen saturation may result in clinical cyanosis If fetal Hb is high, tissue hypoxia may occur even if cyanosis is mild( arterial PaO2 low)
")
6
central peripheral CAUSE ARTERIAL BLOOD DESATURATION OR ABNORMAL Hb CUTANEOUS VASOCONSTRICTION DUE TO LOWCO CONDITIONS Seen in R-L shunt, impaired pulmonary function, abnormal Hb exposure to cold air or water and abnormally greater extraction ofO2 from normally saturated blood SITES conjunctiva,palate,tongue,inner side of lips& cheeks limited to ears,nose,cheeks outer side of lips hands feet&digits certainly central if associated with clubbing and polycythemia, clubbing is absent probably central if it deepens on effort

7
DUCT-INDEPENDENT MIXING LESIONS TGA, TAPVC,TA DUCT-DEPENDANT PBF
CARDIOVASCULAR DUCT-INDEPENDENT MIXING LESIONS TGA, TAPVC,TA DUCT-DEPENDANT PBF TOF,EBSTEINS,TricusidAtre DUCT-Dependant SBF HLHS,IAA,CoA,Critical AS L-RSHUNT &PUL EDEMA SV States PRIMARY LUNG DISEASE AIRWAY OBSTRUCTION EXTRINSIC LUNG COMPRESSION PULMONARY AV MALFORMATION PPHN CNS DYSFUNCTION HEMATOLOGIC MISCELLANEOUS HYPOGLYCEMIA, METABOLICACIDOSIS SEPSIS, HYPOTHERMIA, SHOCK

8
Diagnostic ladder Echo Simple lab investigation Clinical evaluation
History Physical examination Simple lab investigation PO, CXray & ECG Hb conc &peripheral blood filim Echo Invasive cardiac evaluation

9
DIABETES- TTN,RDS,HYPOGLYCEMIA ASTHMA -TTN POLYHYDRAMNIOS - TEF
MATERNAL HISTORY DIABETES- TTN,RDS,HYPOGLYCEMIA ASTHMA -TTN POLYHYDRAMNIOS - TEF PIH – IUGR,POLYCYTHEMIA,HYPOGLYCEMIA LABOUR& DELIVERY PROM –SEPSIS,PNEUMONIA CHORIOAMNIONITIS- SEPSIS C-SECTION- TTN,RDS,PPHN NEWBORN ONSET AT BIRTH- TTN,RDS,MAS,CDH, ONSET –HRS AFTER BIRTH- CCHD,aspiration,TEF

10
CLUES BASED ON ONSET 1st week > 1 week D TGA TOF TGA
Pulmonary Atresia Admixture lesions Tricuspid atresia TAPVC Ebstein SV Critical PS DORV Truncus

11
Examined in neutral thermal enviornment Away from blue phototherapy lights Asses capillary refill time- <2 sec Barrel shaped chest –post term-MAS Bell shaped thorax – neurologic abnormalities Scaphoid abdomen-CDH Look for nasal flaring,grunting & retractions

12
Palpate brachial & femoral pulses BP- all four extrimities SBP-gradient quite specific for arch abnormality Not sensitive S2- split in 80% by 48 hours Differential cyanosis

13
CCHD in Newborns: Clues based on presentation
Cyanosis No Resp Distress Cyanosis + Resp Distress Shock Differential cyanosis TGA DDPC TAPVC obstructed DDSC

14
CCHD in Newborns: Clues Based on S2 split
single normal fixed DDPC TGA DDSC Excludes Cardiac cause TAPVC

15
CCHD in newborns: Clues based on Murmurs
Murmurs have poor sensitivity( < 50%) No Murmur TAPVC with obstruction DDPC( closed PDA) ESM TGA, DDPC, DDSC Continuous murmurs (are) DDPC with collaterals Diastolic murmur (to & fro) TOF- absent pulmonary valve
 No Murmur. TAPVC with obstruction. DDPC( closed PDA) ESM. TGA, DDPC, DDSC. Continuous murmurs (are) DDPC with collaterals. Diastolic murmur. (to & fro) TOF- absent pulmonary. valve.")
16
cardiac respiratory HEART RATE FASTER FAST RESPIRATORY RATE GRUNT ABSENT PRESENT MURMUR PROMINENT CAN BE PRESENT CHF LESSLIKELY ABNORMAL PULSE YES NO RESPONSE TO O2 NOT MUCH GOOD

17
Pulse oximetry Standard of care for all infants with respiratory distress & cyanosis Accurate& reliable method of monitoring o2 saturation in infants noninvasively Pulse oximeter probes on R hand & lower extremity Aim for 02 saturation of 90-95% by pulse oximetry PPHN- suspected –aim for higher o2 saturation

18
HYPEROXIA TEST ADMINISTER 100% O2 FOR 15 MINUTES
ASSES O2 OF UPPER LIMB LOWER LIMB ABG YES TCMO YES PO NO

19
HYPEROXIA TEST GIVE 100% O2 ASSES PO2 PO2>200 PO2<150 NO CCHD LIKELY CCHD PASS FAIL ?CCHD WITH PBF OR PPHN

20
CARDIOMEGALY NO CARDIOMEGALY PULMONARY VASCULARITY EBSTEINS
PAO2 <50MM C X RAY CARDIOMEGALY NO CARDIOMEGALY PULMONARY VASCULARITY EBSTEINS PBF PUL EDEMA PBF TGA + IVS TAPVR With OBSTRN TA with PA orPS PA WITH IVS CRITICAL PS TOF & TOF + PA

21
Those with decreased PBF &normal or slightly increased heart size differentiated by there QRS axis on ECG & MURMUR + or – TA with PS or PA – SUPERIOR QRS AXIS ( 0 to-90) Critical PS & PA with IVS- 0 to 90 degree Differentiated by loud pul ejection murmur TOF & TOF with PA - QRS 90 to 180 Pulmonary continuous murmur Stenosis murmur
 Critical PS & PA with IVS- 0 to 90 degree Differentiated by loud pul ejection murmur TOF & TOF with PA - QRS 90 to 180 Pulmonary continuous murmur Stenosis murmur")
22
Prostaglandin (PGE1) Infusion
Neonates –fail hyperoxia test High Signs& symptoms of CHD or likelihood Present in shock within 1st 3 wk of life of CHD PGE1 administration –open ductus arteriosus Depending on lesion - PBF or SBF or improves Intercirculatory mixing- improves hypoxemia &metabolic acidosis Neonate with shock or CHF in 1st few weeks of life - ductdependant SBF untilproven otherwise

23
mild/no cyanosis + abnormal pulses
PG sensitive lesions: Cyanosis + murmur or mild/no cyanosis + abnormal pulses Can be withheld in a relatively stable child ( SaO2 > 70%; no acidosis) Target SaO2 >80%; pO2 around 45-50, normal pH Once diagnosis is confirmed, it is ideal to start PGE1 before transport. WORSENING AFTER PGE1 – obstruction to blood flow out of pulmonary veins
 Target SaO2 >80%; pO2 around 45-50, normal pH. Once diagnosis is confirmed, it is ideal to start PGE1 before transport. WORSENING AFTER PGE1 – obstruction to blood flow out of pulmonary veins.")
24
Always given as continous IV infusion.
Start at μg/kg/min, can be reduced to µg/kg/min once duct is opened( ^ SaO2) Available as 500 μg vial Trade name: Alpostin/Prostin Cost: Rs 5000/- per ampoule One vial will last 2-3 days for a 3Kg baby
 Available as 500 μg vial. Trade name: Alpostin/Prostin. Cost: Rs 5000/- per ampoule. One vial will last 2-3 days for a 3Kg baby.")
25
Efficacy with age, less effective after 2 weeks of life, not effective after 4 weeks
Adverse reactions more common in premature& LBW infants Apnea –typically in 1st few hrs ,tachycardia, bradycardia, fever, NEC, seizures, thrombocytopenia, Continous cardiorespiratory monitoring

26
PGE1 – peripheral vasodilation – hypotension& cutaneous flushing
Separate IV line should be secured Hypotension treated by 10-20ml/kg bolus of NS,RL,5%albumin Remeasure ABG,reasses capillary refill& vitalsigns within 15 to 30 min of starting PGE1 infusion

27
Principles of managment
Intial stabilisation – airway management reliable venous access – umblical vein Arterial line to monitor BP,acid-base,o2 Volume resucitation,inotropic support & correction of metabolic acidosis Blood glucose & sepsis workup-cyanosis+circ collpse

28
Non invasive delineation of anatomic defect- ECHO Evaluation & treatment of additional organ system-pulmonary,renal,hepatic&CNS Evaluation of additional congenital defects Genetic evaluation – if indicated Cardiac Cathetrisation Surgical managment

29
CCHD is an important differential diagnosis in neonate presenting with cyanosis after birth.
Clinical evaluation with CXR and Hyperoxia test excludes CHD in most cases. Echocardiography recommended in all doubtful cases. Prior stabilization and a monitored transport to tertiary center ensures a optimal pre-operative state. Early intervention with very encouraging results is realistic for most forms of critical CHD in newborns

31
r CCHD derived from heterogeneous group of conditions May have pulmonic stenosis ,PAHor NL pulm pressure with out PS PBF may be NL,INCREASED or DECREASED Decreased PBF may be due to Pulmonic stenosis or PAH Anomalies where free mixing of systemic and venous blood occurs severity of cyanosis determined by pulmonary blood flow Thymus regresses very fast in cyanotic patients

32
Without PS NO VSD With VSD PULM VENOUS OBSTRN PBF PA pressure
CCHD With PS NO VSD With VSD Without PS PA pressure NL PA pressure elevated PBF PULM VENOUS OBSTRN

33
This classification result in six sub group of cyanotic patients PS without VSD PS + large VSD Increased PBF with or without PAH(transposition physiology PAH withdecreased PBF(Eisenmengerphisiology) PAHdue to pul venous obstruction NL or MILD elevated pul pressure without PS
 PAHdue to pul venous obstruction NL or MILD elevated pul pressure without PS")
34
(cyanosis due to R toL shunt at atrial level& cardiomegaly)
PS without VSD (cyanosis due to R toL shunt at atrial level& cardiomegaly) Triad-cyanosis,cardiomegaly,ischemic lung fields on Cxray Dominant a in JVP Cardiomegaly Parasternalimpulse Widely split 2nd HS p2 late &soft 3rd &4th HS Pulm ejection systolic murmur,TR murmur Severe or critical pure PS with failing RV,Ebstein’s
 Triad-cyanosis,cardiomegaly,ischemic lung fields on Cxray. Dominant a in JVP. Cardiomegaly. Parasternalimpulse. Widely split 2nd HS p2 late &soft. 3rd &4th HS. Pulm ejection systolic murmur,TR murmur. Severe or critical pure PS with failing RV,Ebstein’s.")
35
Mild parasternal impulse Systolic thrill uncommon
PS with VSD (Fallot’s physiology) Prominent a wave in jvp NL heart size Mild parasternal impulse Systolic thrill uncommon Single 2nd sound(widely split with inaudible pulmonic sound) ESM Clear diastolic period Ischemic lungs in xray without cardiomegaly
 Prominent a wave in jvp. NL heart size. Mild parasternal impulse. Systolic thrill uncommon. Single 2nd sound(widely split with inaudible pulmonic sound) ESM. Clear diastolic period. Ischemic lungs in xray without cardiomegaly.")
36
D/D of fallots physiology Fallot’stetrology(commonest >2yrs ) TGA TRICUSPID ATRESIA SV DORV correctedTGA AVCD If no rvh on ecg;posssibilities-rv hypoplastic &small,rv absent,PA not connected to RV Tricuspid atresia,hypoplasticRV with or without straddling TV, & single ventricle
 TGA TRICUSPID ATRESIA SV DORV correctedTGA AVCD If no rvh on ecg;posssibilities-rv hypoplastic &small,rv absent,PA not connected to RV Tricuspid atresia,hypoplasticRV with or without straddling TV, & single ventricle")
37
Increased pulmonary blood flow with or without PAH(transposition physiology)
Symptomatic in Neonate Cyanosis-mild to severe Failure to thrive& gain weight CCF Cardiomegaly –in2-3 wks of life 2nd sound single,s3 gallop,insignificant systolic murmur Cardiomegaly with Incrs pulm vasculatureon xray& thymicshadow absent

38
Anomalies with cyanosis and increased PBF TGA DORV without PS TA with Incrs PBF (largeVSD+ NO PS) Persistent Truncus SV without PS TAPVC
 Persistent Truncus SV without PS TAPVC")
39
Cyanosis with PAH and Diminished PBF (eisenmenger- defnd as nonreactive PAH resulting in a R to L shunt at atrial,ventricular or great artery level) Characteristics H/O frequent chest infections in infancy Cyanosis present from birth and appear late Jvp-prominent a wave No cardiomegaly or thrill(except when shunt at atrial level) No PSH Constant EC of PAH
 No PSH. Constant EC of PAH.")
40
2nd sound is palpable,pulmonary component accentuated
Systolic murmur in pulmonary area is insignificant or absent Pulmonary and/or TR murmurs may be present

41
EISENMENGER SYNDROME-DIFFERENTIATION
ASD VSD PDA CYANOSIS UNIFORM DIFFERENTIAL CARDIOMEGALY PRESENT ABSENT PARASTERNAL IMPULSE HEAVING MILD 2nd SOUND WIDE FIXED SPLIT SINGLE NORMALLY SPLIT TR COMMON RARE ASC AORTA IN C Xray NORMAL LARGE

42
PAH-DIFFERENTIATION HYPERKINETIC OBSTRUCTIVE HEART SIZE LARGE
NORMAL(except ASD) PARASTERNAL IMPULSE FORCIBLE &HEAVING-ASD, MILD IN VSD&PDA CLICK OF PAH ABSENT PRESENT 2nd SOUND(P2accentuated in both) ASD-WIDE&FIXED,VSD-WIDE&VARIABLE,PDA-PARADOXICALLY SPLIT ASD-WIDEFIXED VSD-SINGLE PDA-NORMAL Shunt murmur LOUD SHORT OR ABSENT Flow murmur
 PARASTERNAL IMPULSE. FORCIBLE &HEAVING-ASD, MILD IN VSD&PDA. CLICK OF PAH. ABSENT. PRESENT. 2nd SOUND(P2accentuated in both) ASD-WIDE&FIXED,VSD-WIDE&VARIABLE,PDA-PARADOXICALLY SPLIT. ASD-WIDEFIXED. VSD-SINGLE. PDA-NORMAL. Shunt murmur. LOUD. SHORT OR ABSENT. Flow murmur.")
43
Patients with PAH due to Pulmonary Venous hypertension(HLHS&TAPVC with obstruction) Generally present in neonatal period Severe cyanosis,CHF,S3 gallop,no cardiomegaly,absence of significant murmurs, Cxray –NL sized heart with severe PVH- causing GROUND GLASS appearance 2d echo- mitralatresia,aortic atresia,pulmonary venous obstruction, hypoplastic LV
 Generally present in neonatal period Severe cyanosis,CHF,S3 gallop,no cardiomegaly,absence of significant murmurs, Cxray –NL sized heart with severe PVH- causing GROUND GLASS appearance 2d echo- mitralatresia,aortic atresia,pulmonary venous obstruction, hypoplastic LV")
44
Cyanosis without PS & PA pressure normal Heterogeneous group of anomalies TAPVC- features of 2 ASD but with cyanosis,figure of 8 Single atrium-mostly associated with polysplenia SVC entering LA Pulmonary AV fistula

45
Cyanosis+diagnostic approach Dextrocardia
Levocardia With visceral situsinversus complex Poor femoral pulse& Large brachio-poplipteal Systolic pressure gradient Booming p2 Cardiomegaly Prominent pulmonary conus Peripheral vascular pruning Large&relatively silent heart Huge RA oligemic lung fields Giant p wave Prescence of Howell-jolly bodies Syndrome of Levocardia with Visceral situs inversus Coarctation syndrome Eisenmeinger syndrome Ebstein’s anomaly Asplenia

46
Abnormal rhythm& CHD L- TGA Heart Block ; SVT Ebstein - SVT

47
TGA TAPVC DORV Cyanosis&RVH Plethora Oligemia TOF PA PS+ASD&/OR VSD
NL axis/RAD Plethora Oligemia TGA TAPVC DORV TOF PA PS+ASD&/OR VSD PS+TGA/DORV/DOLV

Similar presentations













 with Suspected Heart Disease (A Pragmatist’s Guide) Nick Pigott Staff Specialist in Paediatric Intensive Care Children’s Hospital.>")








