Download presentation
Presentation is loading. Please wait.

1
Diagnosis and Early Management of the Infant with Suspected Congenital Heart Disease

2
Introduction Congenital heart disease occurs in 1% of live- born infants Almost 1/2 of all cases of congenital heart disease are diagnosed during the 1st week of life The most frequently occuring anomalies seen during the 1st week are: PDA, D-transposition of the great arteries, hypoplastic left heart syndrome, TOF, and pulmonary atresia

3
Indications for Fetal Echocardiography

4
Maternal Risk Factors Associated With Congenital Heart Disease Congenital heart disease Cardiac teratogen exposure –Lithium –Amphetamines –Alcohol –Anticonvulsants: phenytoin, valproic acid, carbamazepine, and trimethadione –Isotretinoin

5
Maternal Metabolic Disorders or Infection Diabetes mellitus PKU Hyperthyroidism Lupus, collagen vascular disease Rubella, CMV, Coxsackie, Parvovirus

6
Fetal Risk Factors Associated With Congenital Heart Disease Trisomies, Turner’s syndrome, abnormal karyotype Congenital malformations: duodenal atresia, TEF, omphalocele, diaphragmatic hernia, renal dysgenesis, and hydrocephalus Fetal arrhythmias IUGR Nonimmune hydrops ?2 vessel cord

7
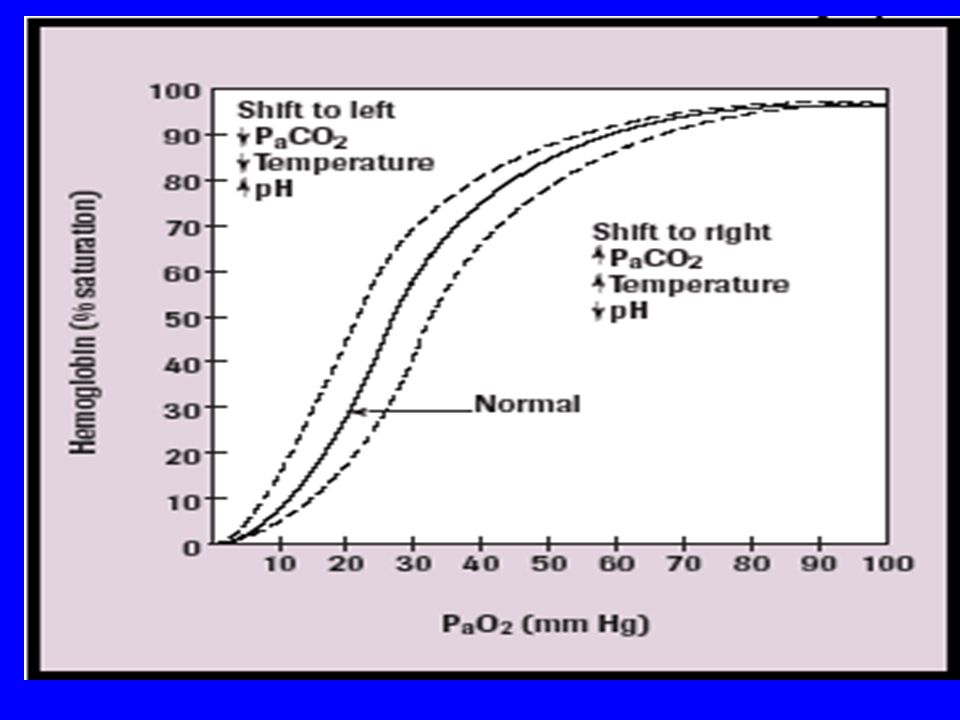
Cyanosis Etiology: CV, pulmonary, airway obstruction, neurological, neuromuscular, or hematological (methemoglobinemia or polycythemia) Infants can appear cyanotic when the deoxygenated Hgb concentration is at least 3g/dL; it is not related to the percent saturated 2 babies with sats of 80%: one with a hgb of 20g/dL and 4g/dL of desaturated hgb will be cyanotic, but an anemic infant with 10g/dL with 2g/dL deoxygenated hgb will not be cyanotic
 Infants can appear cyanotic when the deoxygenated Hgb concentration is at least 3g/dL; it is not related to the percent saturated 2 babies with sats of 80%: one with a hgb of 20g/dL and 4g/dL of desaturated hgb will be cyanotic, but an anemic infant with 10g/dL with 2g/dL deoxygenated hgb will not be cyanotic")
8
Evaluation ABC’s PE: murmur, pulses, precordium, respiratory status, HSM, color, capillary refill 4 ext BPs: if SBP >10mmHg in right hand compared to lower ext, concerning for arch anomaly (though if normal may not rule it out) Pre/post ductal saturations: if see a difference >5%, concerning for PPHN or left heart abnormalities
 Pre/post ductal saturations: if see a difference >5%, concerning for PPHN or left heart abnormalities")
9
Evaluation (Continued) Hyperoxia test: baseline pre-ductal ABG when infant in room air, then repeat on 100% FiO2 Reason for ABG and not just sats: with a saturation of 100%, you can have a PaO2 of 80 or 300; very different CXR: cardiomegaly; normal, increased, or decreased pulmonary vascularity EKG Echo
 Hyperoxia test: baseline pre-ductal ABG when infant in room air, then repeat on 100% FiO2 Reason for ABG and not just sats: with a saturation of 100%, you can have a PaO2 of 80 or 300; very different CXR: cardiomegaly; normal, increased, or decreased pulmonary vascularity EKG Echo")
12
Specific Heart Disease Abnormalities

13
Cyanotic With Decreased Pulmonary Blood Flow Tetrology of Fallot Ebsteins Anomaly Tricuspid Atresia with PA or PS Pulmonary atresia with intact septum Critical pulmonic stenosis PPHN

14
Right Sided Obstructive Lesions Cyanosis No respiratory distress Normal pulses and perfusion Single second heart sound Murmur Moderate to marked hypoxemia CXR: normal to large sized heart, decreased pulmonary blood flow (PBF)
")
15
Tetralogy of Fallot

16
Tetrology of Fallot

17
Ebstein’s Anomaly

19
Tricuspid Atresia

21
EKG : QRS axis Tricuspid atresia with PS or PA with intact ventricular septum: superior (0— -90) Critical PS or PA : 0 to 90 degree quadrant TOF and TOF with PA: 90-180 degree quadrant
 Critical PS or PA : 0 to 90 degree quadrant TOF and TOF with PA: degree quadrant")
22
Cyanotic With Increased Pulmonary Blood Flow d-Transposition of the great vessels Truncus arteriosus Total anomalous pulmonary venous return, above diaphragm Single ventricle Endocardial cushion defect

23
Inadequate Mixing Lesions Cyanosis Mild tachypnea Normal pulses Single heart sound Murmur ABG: marked hypoxemia, + acidosis CXR: cardiomegaly, normal or increased PBF

24
Transposition of the Great Arteries

25
d - Transposition of the Great Vessels

26
Truncus Arteriosus

28
Lesions with Poor Gas Exchange Cyanosis Marked tachypnea Fair perfusion, normal pulses May or may not have a single heart sound May or may not have a murmur CXR: normal heart size, pulmonary congestion

29
Total Anomalous Pulmonary Venous Return

31
Left Sided Obstructive Lesions Coarctation of aorta, interrupted aortic arch Hypoplastic left heart syndrome Aortic stenosis Mitral stenosis Total anomalous pulmonary venous return, below diaphragm

32
Left Sided Obstructive Lesions Grey or ashen color Tachypnea Poor perfusion Decreased pulses/differential pulses Single second heart sound Murmur + gallop Hepatomegaly ABG: metabolic acidosis CXR: cardiomegaly with increased PBF

33
Coarctation of the Aorta

34
Hypoplastic Left Heart Syndrome

36
Aortic Stenosis

37
Acyanotic With Increased Pulmonary Blood Flow VSD ASD PDA Endocardial cushion defect

38
Ventricular Septal Defect

40
Atrial Septal Defect

41
Atrioventricular Canal

42
Patent Ductus Arteriosus

43
Initial Stabilization ABC’s: Volume resuscitation, ionotorpic support, correction of metabolic acidosis, r/o sepsis Intubate if needed, titrate Fi02 to keep Sp02 80%- 85% to prevent pulmonary overcirculation Placement of umbilical lines Infants who present in shock within the first 3 weeks of life, consider ductal dependent lesions Use of PGE1 (0.025 to 0.1mcg/kg/min)
")
44
Stabilization for Transport Reliable vascular access Intubation if on PGE1, OG placement Oxygen delivery, Sp02 Monitor HR, tissue perfusion, blood pressure, and acid-base status Calcium and glucose status (increased risk for DiGeorge)
")
45
Prostaglandin E1 Failure to respond: diagnosis incorrect, older infant with unresponsive ductus, ductus absent, obstructed pulmonary venous return Clinical deterioration after PGE1: obstructed blood flow out of pulmonary veins or left atrium, HLHS with restrictive FO, TGA with intact ventricular septum and restrictive FO, obstructed TAPVR, mitral atresia with restrictive FO

46
PGE 1 - Side Effects Common: Apnea, fever, leukocytosis, cutaneous flushing, and bradycardia. Uncommon: seizures, hypoventilation, hypotension, tachycardia, cardiac arrest, sepsis, diarrhea, DIC, fever Rare: urticaria, bronchospasm, hemorrhage*, hypoglycemia, and hypocalcemia *inhibits platelet aggregation

Similar presentations















 with Suspected Heart Disease (A Pragmatist’s Guide) Nick Pigott Staff Specialist in Paediatric Intensive Care Children’s Hospital.>")










