Download presentation
Presentation is loading. Please wait.

1
Interesting Case Rounds Nadim J Lalani 20.07.2006

2
Patient C.B : 53 y.o. Transferred to FMC CCU from Red Deer with Acute MI PMHx: HTN Depression Etoh Abuse COPD on home O2 VP shunt 1996 [Obtructive Hydrocephalus due to benign mass] shunt revision 98

3
Pt C.B. Meds: Avalide Wellbutrin Imipramine Effexor Tryptophan Smoker has many cats

4
HPI: March 17 experiencing chest pain and HA Agitated, was pacing & collapsed EMS to Innisfail Hospital In ED: Vitals: 36 9, hr 119, 35, 106/80, Some respiratory distress. Neuro: Confused but following commands R pupil 5mm > L 4mm plantar response: Agitated

5
Innisfail ED [contd]: Given: Asthma cocktail Ativan for agitation Transferred to Red Deer: Confusion / agitation / sob
![Innisfail ED [contd]: Given: Asthma cocktail Ativan for agitation Transferred to Red Deer: Confusion / agitation / sob](http://images.slideplayer.com/1/257054/slides/slide_5.jpg "Innisfail ED [contd]: Given: Asthma cocktail Ativan for agitation Transferred to Red Deer: Confusion / agitation / sob")
6
Red Deer Hospital: Confused,agitated,restless, intermittent fevers Vitals: Afeb 120, 24, 100/75,93% Altered LOC, GCS 6,pupils variable ? tone, rambling speech

7
Red Deer Hospital [contd] Initial Labs: ABG: 7.37/41/116/24 Hb 137, WBC 15.2, Plt 264 CK 559 (< 140 u/L) Acetominophen/ ETOH/ ASA: all NEG
![Red Deer Hospital [contd] Initial Labs: ABG: 7.37/41/116/24 Hb 137, WBC 15.2, Plt 264 CK 559 (< 140 u/L) Acetominophen/ ETOH/ ASA: all NEG](http://images.slideplayer.com/1/257054/slides/slide_7.jpg "Red Deer Hospital [contd] Initial Labs: ABG: 7.37/41/116/24 Hb 137, WBC 15.2, Plt 264 CK 559 (< 140 u/L) Acetominophen/ ETOH/ ASA: all NEG")
8
CXR: Hyperinflation EKG: N Admitted with the following issues: COPD ? Seratonin Syndrome ? Etoh Withdrawal

9
Red Deer Hospital [Contd] Next 24 - 48H: Improved on IV fluids, multi-vits Solu-medrol & withholding psyc meds. March 20: breathlessness, LOC CXR: mild oedema ABG: 7.35/72/135/40 Intubated had following EKG:
![Red Deer Hospital [Contd] Next H: Improved on IV fluids, multi-vits Solu-medrol & withholding psyc meds.](http://images.slideplayer.com/1/257054/slides/slide_9.jpg "March 20: breathlessness, LOC CXR: mild oedema ABG: 7.35/72/135/40 Intubated had following EKG:.")
13
Red Deer Hospital [contd] Next 24H: extubated, more alert & lucid EKG: T-wave changes Echo: akinetic apex TNi 7.11 (0-0.10ug/L) (>1.5 ug/L= MI) CK 1751 CT head: Reported as Normal Pt transferred to FMC Cardiology Dx: MI on Nitro drip and Heparin
![Red Deer Hospital [contd] Next 24H: extubated, more alert & lucid EKG: T-wave changes Echo: akinetic apex TNi 7.11 (0-0.10ug/L) (>1.5 ug/L= MI) CK 1751 CT head: Reported as Normal Pt transferred to FMC Cardiology Dx: MI on Nitro drip and Heparin](http://images.slideplayer.com/1/257054/slides/slide_13.jpg "Red Deer Hospital [contd] Next 24H: extubated, more alert & lucid EKG: T-wave changes Echo: akinetic apex TNi 7.11 (0-0.10ug/L) (>1.5 ug/L= MI) CK 1751 CT head: Reported as Normal Pt transferred to FMC Cardiology Dx: MI on Nitro drip and Heparin")
14
En route to Foothills Hospital: Patient: became lethargic, gasping GCS decreased to 8 pupils unequal intubated (again)
")
15
Foothills Hospital CCU [Mar 22]: Exam: VSS Intubated, withdrawing, opens eyes to pain reflexes 4+ LEs ? tone, 4 beat clonus shunt depresses and fills completely
![Foothills Hospital CCU [Mar 22]: Exam: VSS Intubated, withdrawing, opens eyes to pain reflexes 4+ LEs .](http://images.slideplayer.com/1/257054/slides/slide_15.jpg "tone, 4 beat clonus shunt depresses and fills completely.")
16
Whats going on?

17
CCU: Gets Repeat CT

21
March 22 [contd] NeuroSurgery Consulted ? Shunt Malfxn Initial exam: Intub, withdrawing disconjugate gaze Drain off 20cc via shunt reservoir Pt immediately awakes, begins reaching for ETT Cannot palpate distal shunt got AXR:
![March 22 [contd] NeuroSurgery Consulted .](http://images.slideplayer.com/1/257054/slides/slide_21.jpg "Shunt Malfxn Initial exam: Intub, withdrawing disconjugate gaze Drain off 20cc via shunt reservoir Pt immediately awakes, begins reaching for ETT Cannot palpate distal shunt got AXR:.")
24
March 23-26: Further 20 cc drained off [02:00 am] In a.m Cardiac cath: Normal Coronaries Echo: Mild LV hypokinesis Pt had shunt studies went to OR third ventriculostomy Pt does well. Discharged home
![March 23-26: Further 20 cc drained off [02:00 am] In a.m Cardiac cath: Normal Coronaries Echo: Mild LV hypokinesis Pt had shunt studies went to OR third ventriculostomy Pt does well.](http://images.slideplayer.com/1/257054/slides/slide_24.jpg "Discharged home.")
26
HydroCephalus First described by Hippocrates Epidemiology: 1.2/1000 live births Disturbance of CSF flow

27
CSF physiology Secreted by Choroid Plexus [20ml/h] Passive absorption: SA space venous system Mostly obstruction [except choroid papilloma]
![CSF physiology Secreted by Choroid Plexus [20ml/h] Passive absorption: SA space venous system Mostly obstruction [except choroid papilloma]](http://images.slideplayer.com/1/257054/slides/slide_27.jpg "CSF physiology Secreted by Choroid Plexus [20ml/h] Passive absorption: SA space venous system Mostly obstruction [except choroid papilloma]")
28
Causes of Hydrocephalus Prematurity (posthemorrhagic) Myelomeningocoele Other congenital (Aqueductal stenosis &c.) Brain tumor Subarachnoid hemorrhage Meningitis
 Myelomeningocoele Other congenital (Aqueductal stenosis &c.) Brain tumor Subarachnoid hemorrhage Meningitis")
29
Shunts Three Parts: Ventricular catheter Valve Distal Catheter Diverted to: Peritoneum Pleural Cavity GB, RA, IJ Lumbar CSF Shunts

30
Shunts

31
Shunt Malfunction Two categories : Shunt Failure Infection Infection : Coag negative Staph Fevers/malaise meningitis Important to r/o in paeds presentation

32
Shunt Failure Shunt Failure: Debris Component failure Fracture/ separation/ migration 30-40% fail within 1 st year 15% failure in 2 nd year After 2 nd year 1-5% failure /year Mortality 1-4%

33
Assessment Hx: [ incr ICP] HA [morning], neck pain N/V Irritability, gait problems, recent VP shunt P/E: Papiloedema CN VI palsy,CN III palsy Sunsetting ALOC / Coma Dont forget to palpate the shunt
![Assessment Hx: [ incr ICP] HA [morning], neck pain N/V Irritability, gait problems, recent VP shunt P/E: Papiloedema CN VI palsy,CN III palsy Sunsetting ALOC / Coma Dont forget to palpate the shunt](http://images.slideplayer.com/1/257054/slides/slide_33.jpg "Assessment Hx: [ incr ICP] HA [morning], neck pain N/V Irritability, gait problems, recent VP shunt P/E: Papiloedema CN VI palsy,CN III palsy Sunsetting ALOC / Coma Dont forget to palpate the shunt")
35
Hx & P/E not very sensitive SensSpec Nausea /Vomit 3697 HA1597 ALOC10100 Papilloedema3100

36
Usefulness of balloting the shunt? Rationale: If it depresses patent distally If it refills patent proximally Reality: Sensitivity only 20% in the hands of Nsx! Even positive test not useful [25% false]

37
Radiography? Shunt Survey [XR skull, Chest, KUB]: Sensitivity 20% LR –ve 0.82 CT: 83% sens LR –ve 0.21 Combined : 88 sens BUT! 1 in 8 pts with obstruction have normal studies

38
Diagnostics Shunt study: Test of choice Usually NSx has to order Tapping the shunt: Easy to do / therapeutic Can send CSF [Can measure ICP]
![Diagnostics Shunt study: Test of choice Usually NSx has to order Tapping the shunt: Easy to do / therapeutic Can send CSF [Can measure ICP]](http://images.slideplayer.com/1/257054/slides/slide_38.jpg "Diagnostics Shunt study: Test of choice Usually NSx has to order Tapping the shunt: Easy to do / therapeutic Can send CSF [Can measure ICP]")
39
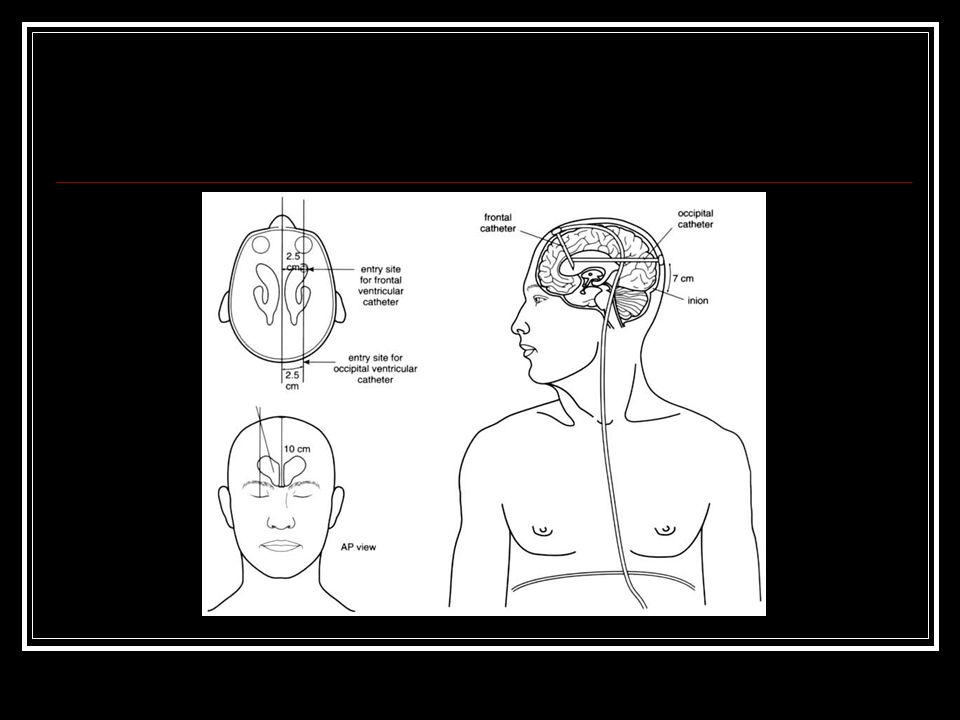
Tapping the Shunt Sterile Prep 25 gge Butterfly Tubing/syringe Take off 20 cc at a time

40
What about the MI ?:

41
Neuro-mediated Cardiac Stress: Electrocardiographic abnormalities well described for SAH TWi, ST Long QT &c. Originally thought to be benign SAH now known to cause: significant increases in ICP, Increased cardiac output Significant changes in creatine kinase and catecholamines

42
Furthermore, Pts with SAH and ST have been shown to have impaired contractilityneurogenic stunned myocardium One other Report of this related to hydrocephalus from choroid cyst But now recognise that both psychiatric physiologic stressors can cause an MI picture.

43
Transient LV dysfunction Clinically resembles acute myocardial infarction Characteristics of: transient/reversible LV dysfunction with chest pain EKG changes release of cardiac enzymes hypokinesis of LV on echo Normal coronary arteries

44
Clinically: elderly women over 60 years of age some physical or mental stress precedes the onset of the symptom Most common presenting symptom is chest pain or dyspnea Often CHF from decreased left ventricular systolic function

45
Diagnostics: EKG findings classically initial ST elevation ST depression Deep symetric T wave inversion Abnormal QT Small or moderate elevation of cardiac enzymes (large elevations unusual)
")
46
Etiology/Associated Events: Emotional stress (death of loved one, panic d/o) Pneumothorax, resp distress, subarachnoid haemorrhage Trauma Phaeochromocytoma Guillain-Barré syndrome
 Pneumothorax, resp distress, subarachnoid haemorrhage Trauma Phaeochromocytoma Guillain-Barré syndrome")
47
Pathophysiology: Animal/perfusion models support idea that it is likely the result of catecholamine surge involves microvascular perfusion AbN In some it involves coronary artery spasm

48
Pt C.B: Psych Hx Female, Over 50 Chest pain and dyspnea Echo that had apical hypokinesis ST that progressed to deep TWi and QT Normal Cath

49
Voila!

50
Questions?

51
References: 1. Physical examination of Patients With cerebrospinal Fluid Shunts: Is There Useful Information in Pumping the Shunt? Joseph H. Piatt Pediatrics 1992; 89(3):470-473. 2. Pitfalls in the diagnosis of ventricular shunt dysfunction: radiology reports and ventricular size. Iskandar BJ, McLaughlin C, Mapstone TB, Grabb PA Oakes WJ Pediatrics 1998; 101 (6): 1031-6 3. Evaluation of Hydrocephalus Shunts in the Emergency Room Robert C Dauser Emergency Medicine Clinics of North America 1987; 5 (4): 709-717
: Pitfalls in the diagnosis of ventricular shunt dysfunction: radiology reports and ventricular size. Iskandar BJ, McLaughlin C, Mapstone TB, Grabb PA Oakes WJ Pediatrics 1998; 101 (6): Evaluation of Hydrocephalus Shunts in the Emergency Room Robert C Dauser Emergency Medicine Clinics of North America 1987; 5 (4):")
52
References : 4.Radiographic evaluation for suspected cerebrospinal fluid shunt obstruction. Zorc JJ, Krugman SD, Ogborn J, Benson J. Pediatr Emerg Care. 2002 Oct;18(5):337-40 5.Ventriculoperitoneal shunt block: what are the best predictive clinical indicators? Barnes NP, Jones SJ, Hayward RD, Harkness WJ, Thompson D. Arch Dis Child. 2002 Sep;87(3):198-201. 6. Akashi et al. The clinical features of takotsubo cardiomyopathy. Q J Med. 2003: 96:563-573
: Ventriculoperitoneal shunt block: what are the best predictive clinical indicators. Barnes NP, Jones SJ, Hayward RD, Harkness WJ, Thompson D. Arch Dis Child Sep;87(3): Akashi et al. The clinical features of takotsubo cardiomyopathy. Q J Med. 2003: 96:")
53
7.Characterization of the cardiac effects of acute subarachnoid hemorrhage in dogs. Elrifai AM, Bailes JE, Shih SR, Dianzumba S, Brillman J. Stroke. 1996 Apr;27(4):737-41 8.Left ventricular wall motion abnormalities in patients with subarachnoid hemorrhage: neurogenic stunned myocardium. Kono T, Morita H, Kuroiwa T, Onaka H, Takatsuka H, Fujiwara A. J Am Coll Cardiol. 1994 Sep;24(3):636-40. 9.Myocardial injury and left ventricular performance after subarachnoid hemorrhage. Mayer SA, Lin J, Homma S, Solomon RA, Lennihan L, Sherman D, Fink ME, Beckford A, Klebanoff LM. Stroke. 1999 Apr;30(4):780-6.
: Left ventricular wall motion abnormalities in patients with subarachnoid hemorrhage: neurogenic stunned myocardium. Kono T, Morita H, Kuroiwa T, Onaka H, Takatsuka H, Fujiwara A. J Am Coll Cardiol Sep;24(3): Myocardial injury and left ventricular performance after subarachnoid hemorrhage. Mayer SA, Lin J, Homma S, Solomon RA, Lennihan L, Sherman D, Fink ME, Beckford A, Klebanoff LM. Stroke Apr;30(4):")
54
Roberts: Clinical Procedures in Emergency Medicine, 4th ed., Copyright © 2004 Garton HJL and Piatt JH Hydrocephalus. Pediatr Clin N Am 51 (2004) 305-325
")
Similar presentations
























>")



