Download presentation
Presentation is loading. Please wait.

1
ECG ROUNDS Navpreet Sahsi

2
“ED Doc to Bed 9”

4
Patient - Sent from Pre-admission clinic because of ECG findings
“I feel fine, I don’t know what the big deal is!” Asymptomatic, resting comfortably Obese, 50 years old, male. Meds: Spironolactone, lisinopril T- 36.7, HR 70, BP – 205/118, RR 12, 96 % RA Thoughts?

5
“Oh, and by the way I have these bilateral adrenal tumors.”
Chart shows a recent diagosis of bilateral adrenal tumors -> hypercortisolemia Does this change anything?

6
ECG Findings in Metabolic/Endocrine Disease

7
The Ultimate “Pimp” Question
What are the “classic” ECG manifestations of pheochromocytoma???

8
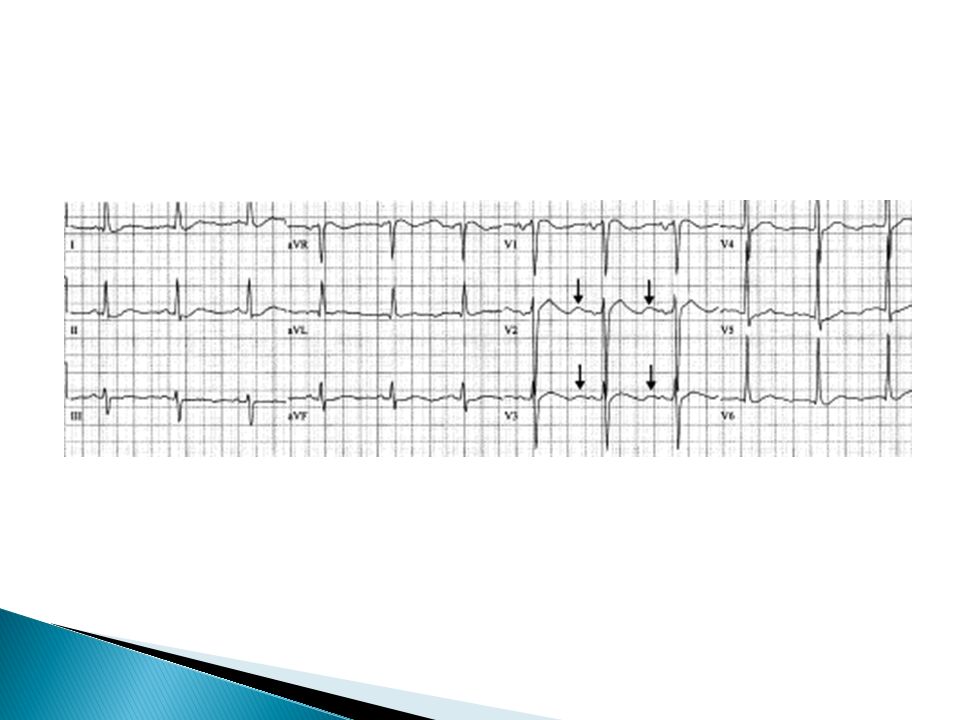
ECG in Pheo No “classic” ECG
Often present with ST elevation in a variety of patterns, mimicking acute infarction Can also present with other ST-T changes, most commonly T wave inversions QTc often prolonged – risk of arrythmias Case series – 25 patients with eventual diagnosis of pheo – 17 had abnormal ECG findings, 6 had initial diagnosis of acute STEMI - > urgent angiography - > all were normal Cardiovascular Manifestations of Pheocromocytoma.AM J Em Med, 18:5; : 2000. ECG manifestations of endocrine disease. Heart 2001, 86; 679.

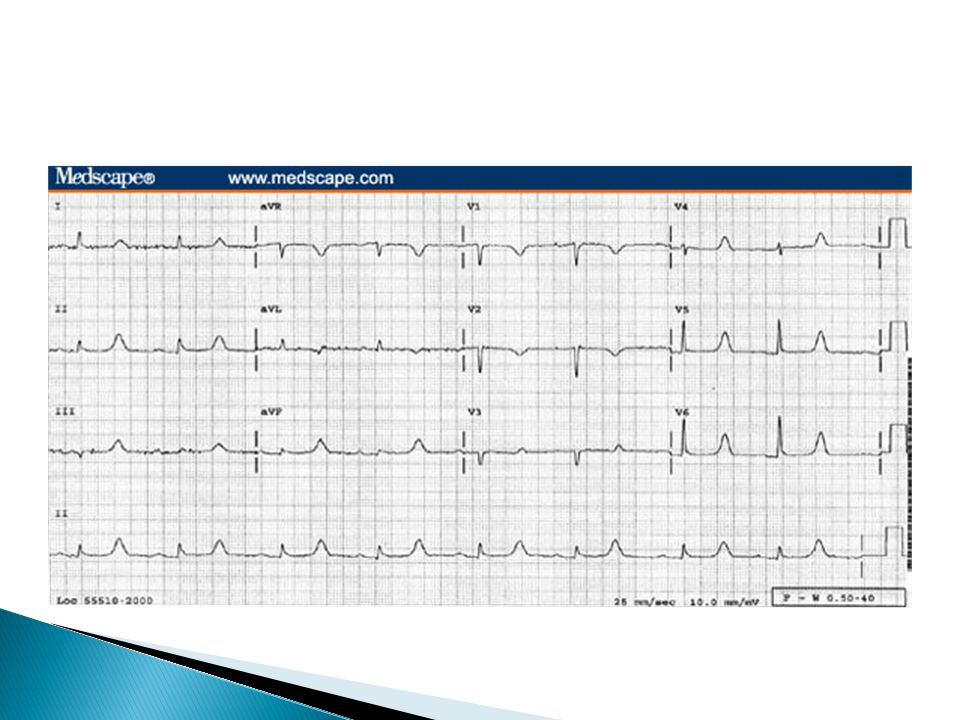
11
DONCKIER, J. E et al. Heart 2001;85:679
Copyright ©2001 BMJ Publishing Group Ltd.

13
Hyper K+ Peaked T waves P wave flattening, PR prolongation, eventual loss of p waves QRS widening Sine wave appearance

16
Hypo K Depression of T waves ST depression (> 0.5 mm)
Appearance of U waves

19
Hypothyroidism Sinus brady Low voltage complexes
Prolonged pr and qt intervals Flattened or inverted T waves Pericardial effusions occur in 30% of patients and may account for some of the changes

20
Hyperthyroid Sinus Tach – 40 % A. Fib – 10 – 22 %
Nonspecific ST-T abnormalities – 25 % Interventricular conduction disturbances – LAFB most common – 15 %

22
HyperCa Shortenes plateau phase (phase 2) of action potential and shortens effective refractory period ST shortening Short QT interval

24
Two abnormalities?

26
Hypothermia T < 35.0 Tremor arifact
One of earliest signs – secondary to shivering Slowing of sinus rate - > bradycardia Prolongation of PR and QT intervals Osborn/J wave

27
Osborn or J wave “Camel Hump sign”
Extra deflection off of terminal portion of QRS and ST segment takeoff Size correlates directly with degree of hypothermia Usually present when temp < 32.0 deg. C Can occur in HyperCa, Massive head injury, subarachnoid hemmorrhage

28
Back to the case Cardiology consulted
Not concerned about an acute event because patient completely asymptomatic Decided to admit patient for pre-op workup since he next in queue for surgery Led to angiogram - > normal Booked for surgery

Similar presentations


















 Cardiovascular System Physiology Lab Interpretation Dr.Mohammed Sharique Ahmed Quadri Asst. professor in physiology بسم الله الرحمن.>")









