Download presentation
Presentation is loading. Please wait.

1
Pediatric Clinical Diagnosis
Hartono Gunardi, Sudigdo Sastroasmoro, Irawan Mangunatmadja, Department of Child Health, Medical School University of Indonesia, Jakarta

2
Differences Adult and Pediatrics
A child is not a small adult ! History is given by second person. The parents may place their own interpretation on events(any fever may be called tonsillitis). The cooperation of the child cannot be guarantied The expression of the disease may be influenced by the child’s developmental status (hypothermia may indicates severe infection in newborn)
. The cooperation of the child cannot be guarantied. The expression of the disease may be influenced by the child’s developmental status (hypothermia may indicates severe infection in newborn)")
3
Differences Adult and Pediatrics
The predominant impact of the disease may be on growth and development (UTI, Chronic illness). Physiological norms are more constant in adults, variable with age in infants and children( HR, RR) Clinical signs of the disease may differ from those of adults (Liver is palpable in infancy).
. Physiological norms are more constant in adults, variable with age in infants and children( HR, RR) Clinical signs of the disease may differ from those of adults (Liver is palpable in infancy).")
4
Clinical exam in infants and children: Why special attention?
A child is not a small adult! Keywords: growth and development Any information about history, physical, and laboratory / supporting exams should be judged in relation with the child’s stage of growth and development.

5
The diagnostic paradigm:
History Physical Routine lab Special investigations

6
Pediatric History (Anamnesis)
Auto-anamnesis: self reporting by the patient Allo-anamnesis: any information other than by patient

7
Listen to them; they are telling you the diagnosis!!!
History: ≥80% Supporting exam: 5% Physical exam 10-20% Listen to them; they are telling you the diagnosis!!!

8
Pediatric history Introduce yourself to the parents and child.
A warm greeting and friendly smile to allay anxiety and promote confidence. Encourage the parents to tell the story with minimum of interruption and listen carefully. You should not swallow the diagnosis given by the parents. It is essential to find out what the concern of the parents are.

9
Anatomy of history taking
Patient’s identity Chief complaint Clinical course Previous illness History of maternal pregnancy History of delivery Feeding history Immunization status Growth and development Family history Environment

10
Pediatric history Presenting/Chief Complaint. Develop DD/
History of present illness and important related positive & negative symptoms. to exclude by anamnesis Systems review Past history

11
Pediatric history Maternal history (Pre-natal). Birth history (Natal).
Post-natal history. Nutritional history. Immunization Growth and development Family history Social and environmental history

12
Maternal history Multiparity, any miscarriages, stillbirth or congenital malformation. Maternal health during pregnancy (hypertension, TORCH), regular antenatal care, Rh iso-immunization. History of drugs ingestion during pregnancy, oligohydroamnios or polyhydroamnios
, regular antenatal care, Rh iso-immunization. History of drugs ingestion during pregnancy, oligohydroamnios or polyhydroamnios.")
13
Birth history Mode of delivery. Crying immediately or not. Apgar score
History of asphyxia Meconium stained amniotic fluid.

14
Post-natal history NICU admission?
How long did the baby stay in the nursery. Did the baby required mechanical ventilation ? Oxygen was given ? Duration of oxygen. Baby had history of jaundice? Exchange transfusion done? Any illness during first month of life: meningitis, convulsion, fever ..etc.

15
Nutritional history Breast feeding or bottle feeding Type of formula
How much milk is given , number of feeds/day How is the milk prepared When the solid food or cereals is introduced, content of food, any allergy to the food.

16
Immunization history Vaccination program in details (National)
Any special vaccination was given. When the last vaccine was given Any complication of given vaccine (Any contraindications for certain vaccine?)
")
17
Growth and development history
- Details of weight increment (KMS) Details of development milestones: smiling , sitting, standing, walking, speech Bladder and bowel control School performance, behavioral and emotional history.
 Details of development milestones: smiling , sitting, standing, walking, speech. Bladder and bowel control. School performance, behavioral and emotional history.")
18
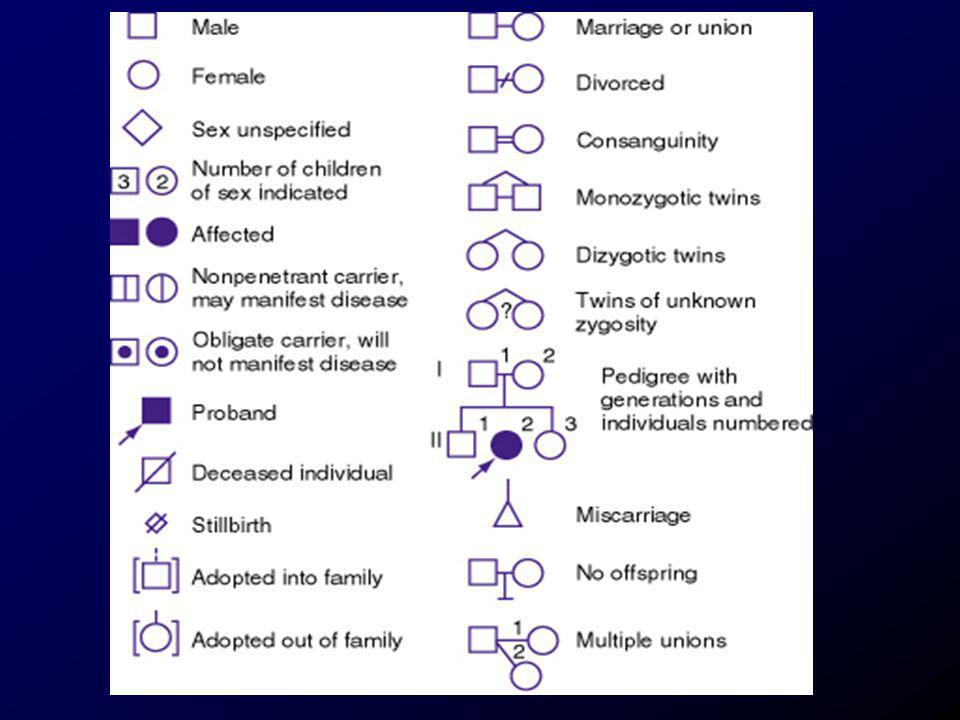
Family history Father and mother age, consanguinity, level of education and they are healthy or not. History of smoking in either parent Siblings: number, sex, and their ages. History of similar disease, chronic ds (TB), unexplained death and genetic diseases. Draw family pedigree
, unexplained death and genetic diseases. Draw family pedigree.")
21
Social & Environmental history
It is necessary to build up a picture of the child’s social and cultural environment Appreciate fears and stresses at home( parental attitudes, separation, divorce, absence of parent) Jealously at the arrival of a new baby Unexplained injuries may raise the possibility of child abuse.
 Jealously at the arrival of a new baby. Unexplained injuries may raise the possibility of child abuse.")
22
Should complete history be obtained in all patients irrespective of their illness?
A 8-year old girl, 30 kg, 130 cm, 3rd grade of elementary school, repeatedly had good ranking in class. She was brought to the clinic due to 3-day high grade fever, stomach ache, and epistaxis 2. A 12-year old boy, basketball player, suspected of suffering from radial fracture.

23
The “My 5 Moments for Hand Hygiene” approach

25
Pediatric Examination
Important points to remember: The examination of infants and children is an art, demanding qualities of understanding, sympathy and patience. Heart rate, Respiratory rate, BP, liver size, heart size varies with age. Keep disturbing or painful procedures to the end. It is not necessary to be systemic in your examination , but should be complete.

26
Physical examination In general similar to that in adults, i.e. to obtain accurate physical status irrespective of the approach Needs modification due to nature of infants & children: Start with inspection Followed by auscultation: abdomen & heart End with examination using equipment

27
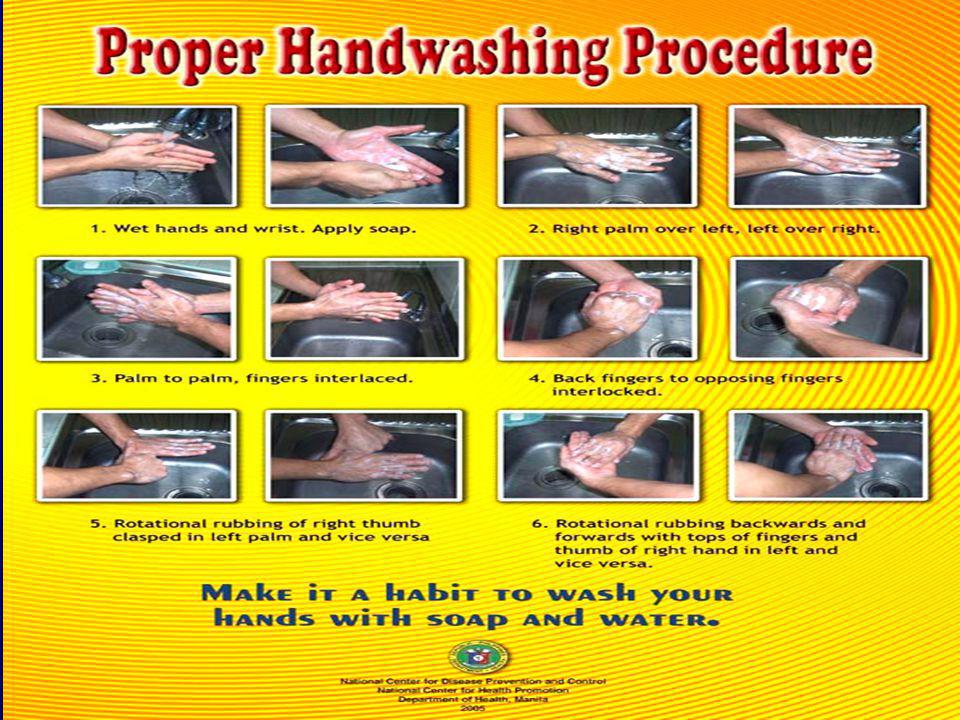
Pre-exam checklist: WIPE
:Wash your hands [thus warming them]. Introduce yourself to pt, explain what going to do. Position pt [+/- on parent's knee]. Expose area as needed [parent should undress]. Any unusual behavior. If asleep, do the heart, lungs and abdomen first.

28
Pre-exam checklist Parent-child interaction, reaction to someone new walking entering the room (child abuse). Ask if tenderness anywhere, before start touching them.

29
Steps in physical exam General condition Vital signs
Anthropometric measurements Systematic exam

30
General condition 1. Consciousness : alert, apathetic, somnolent, soporous, comatous 2. Appearance : health, mild / moderate / severely ill, distressed 3. Color : pale, jaundiced, cyanotic 4. Specific facies : syndromes, facies cholerica, fish-mouth, facies leonina, Cooley’s facies

31
B. Vital signs 1. Pulse : rate, regularity, volume, equality
2. Respiration : rate, regularity, pattern 3. Blood pressure : of 4 extremities 4. Temperature : oral, axillary, rectal Note: always describe complete pulse & respiration!

32
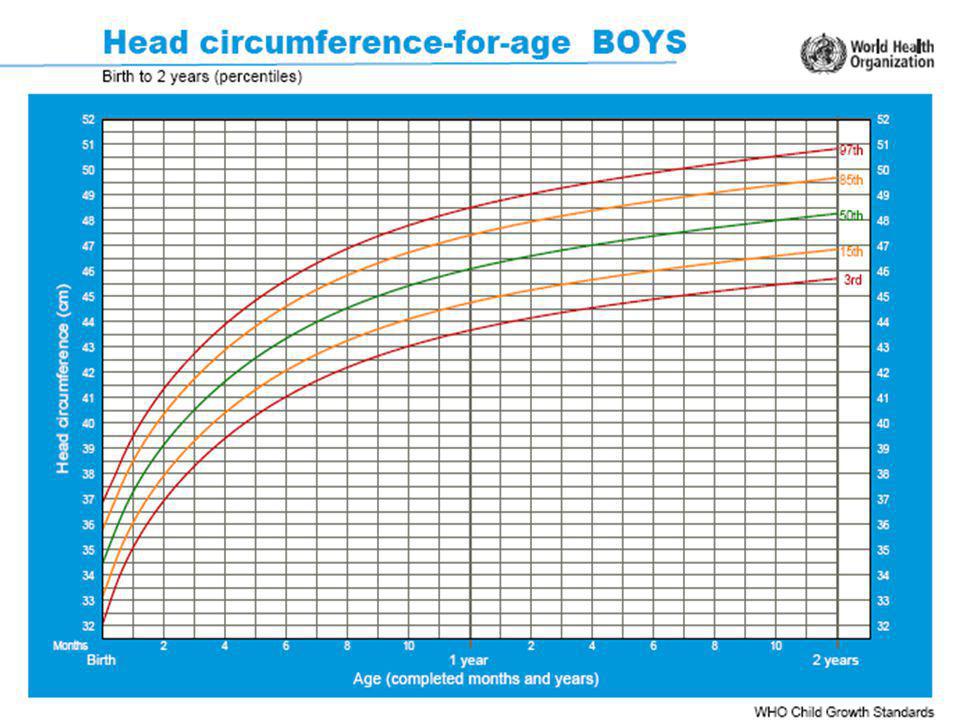
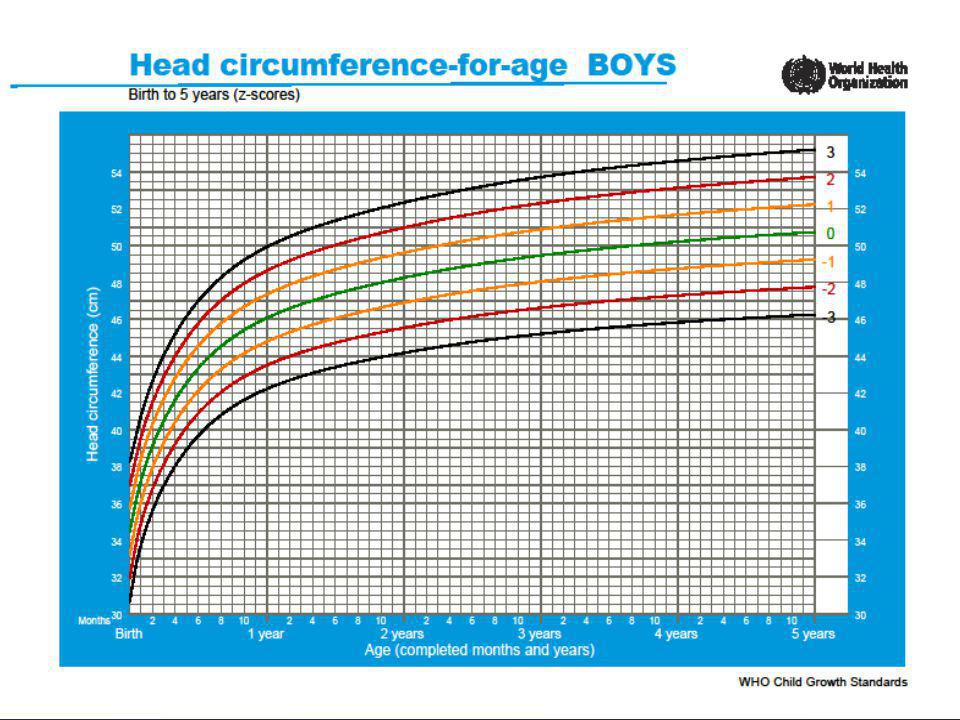
C. Anthropometric measurements
1. Body length / height: sitting, standing 2. Body weight 3. Head circumference 4. Arm circumference 5. Abdominal circumference 6. Nutritional status: W/A, H/A, W/H plot in standard normal curve (WHO or NCHS)
")
39
D. Systematic examination
Head and neck Chest Abdomen Genitals Extremities Skin, hair, lymph nodes Neurological

40
Head Examine the head for shape, asymetry Sutures, Bone defects
Size and tension of fontanelles Head circumference, rate of growth. microcephaly, macrocephaly other visible abnormalities The hair and scalp should be examined

41
Position

42
Eye Examination Look for palpebral edema, ptosis, exopthalmus
Examine the conjunctivae for anemia and sclerae for jaundice and the cornea for haziness and opacities Pupils size and shape, pupil reflex Evaluate for strabismus by position of the light reflex and the cover test. Strabismus is normal before 4-6 months. Look for nystagmus Fundoscopic examination Visual fields should be tested in all children old enough to cooperate

43
Eye abnormality?

44
Ears Examination Exam position: same as eye, but child faces the side.
Check for position (low set ) and shape of both ears. Discharge, canals, external ear tenderness. Otoscope to examine ear drums. Evaluate hearing. The mastoid also need to be checked
 and shape of both ears. Discharge, canals, external ear tenderness. Otoscope to examine ear drums. Evaluate hearing. The mastoid also need to be checked.")
46
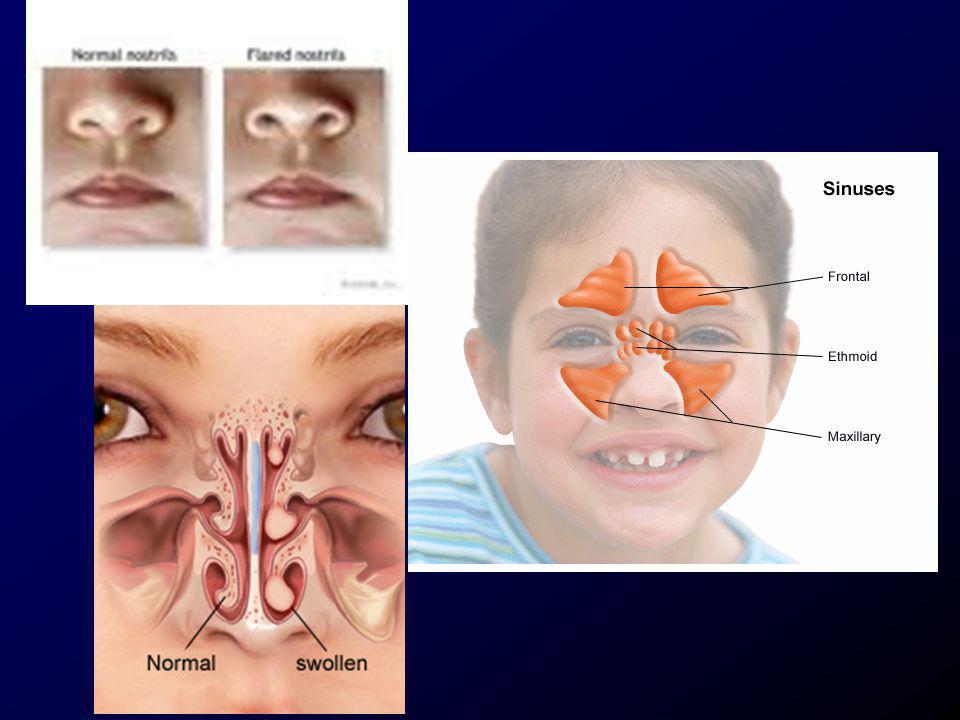
Nose and sinuses The nasal examination is performed to detect deformities. Deviation of the septum Color and state of the mucosa and turbinates Presence of foreign body Examine the sinuses for tenderness

48
Mouth and throat Breath odor The color of lips and mucosa
The condition of teeth, gums (hypertrophy in phenytoin) and buccal mucosa Look for tongue (geographic tounge), palate, tonsils and pharynx Listen to the voice and the quality of cry and the presence of stridor
 and buccal mucosa. Look for tongue (geographic tounge), palate, tonsils and pharynx. Listen to the voice and the quality of cry and the presence of stridor.")
49
Tonsils

51
Neck Examine for nuchal rigidity Swelling Webbing
Lymph node : location, consistency, size, tenderness Thyroid gland The position of trachea

52
Chest Inspection The general shape (pectus excavatum or pectus carinatum) Abnormal signs : beading (rosary), asymmetry of expansion Asess rate,pattern and effort of breathing Identify variations of respiration and signs of respiratory distress Recognize grunting, stridor

54
Chest Palpation Percussion
Auscultation: breath sounds in children are usually bronchovesicular. Recognize : wheezing, crackles and asymmetric breath sounds

55
Cardiovascular system:
Inspection : Precordial bulge, apical heave. Palpation: apex beat : in the 4th intercostals space in the midclavicular line in children < 7 years ; after that apex : the 5th ics. Thrill ? Percussion Auscultation: heart sound, murmur Note the effect of changing of position and exercise on the murmur. Splitting of the 2nd heart sound is common in normal children

56
Heart Sounds

57
Abdomen (1) Inspection: Shape: Distension, Scaphoid abdomen,
Visible swellings, hernias. Umbilicus, veins. Visible peristalsis. Auscultation: Bowel sounds.

58
Abdomen (2) Palpation: Masses.
Areas of ternderness, rebound, guarding. Liver, spleen: <6 years may palpate up to 2cm below costal margin. Kidneys, bladder. Percussion : Fluid wave, shifting dullness. Liver, spleen.

60
Genitalia Recognize genital abnormalities in a boy : cryptorchidism, hypospadias, phymosis, hydrocele Palpate the testes Recognize genital abnormalities in a girl: signs of virilization, labial adhesions and signs of injury

61
Back Inspection and palpation: Posture : lordosis, kyphosis, scoliosis
Masses Tenderness Limitation of motion Spina bifida

62
Anus Patency (imperforated anus)
Presence of fissure, fisulae or hemorrhoids Rectal examination if indicated

63
Musclo-skeletal system
Assess symmetry of length and size. Observe shape of bones, temp, and color. Observe for bowlegs: space b/t the knee more than 5 CM. should disappear after 2-3Y. Inspect for knock-knee: from 2-7Y, and distance between two ankle should not exceed 3 CM. Palpate for presence on edema. Assess muscle strength and muscle tone estimation. Always s examine for congenital dislocation of the hip in infants

65
Extremities (1) Examine the hips of a newborn for congenital dysplasia using Ortolani maneuvers
 Examine the hips of a newborn for congenital dysplasia using Ortolani maneuvers")
66
Extremities (2) Identify age-related changes in gait
Identify age- related variations ,tibial torsion,genu valgus,flat feet

68
Neurological Examination
Observation Mental status Cranial nerves Cerebellar function Motor system Sensory system Reflexes-primitive (neonatal reflexes, deep and superficial reflexes.

69
Neurologic (1) Abnormalities during play.
Limbs: movement, tone, limp, Gower's sign. Head control.

70
Neurologic (2) Reflexes: Moro and tonic neck reflexes <3months.
Babinski's sign positive <12-15 months. Hypertonicity commonly is normal infants, but hypotonicity is abnormal. Other reflexes: grasp, suck, root, stepping and placing.

71
Moro reflex

73
Neurologic (3) Meningitis signs if indicated: Kernig, Brudzinski.
 Meningitis signs if indicated: Kernig, Brudzinski.")
74
Use of stethoscope Use binaural stethoscope
Bell-shaped side: for low & medium pitched sounds Membrane (diaphragm): for medium to high pitched sounds For heart exam use bell-shaped side first start without pressure, then with pressure End with diaphragm side
: for medium to high pitched sounds. For heart exam. use bell-shaped side first. start without pressure, then with pressure. End with diaphragm side.")
75
performing examination
Common mistakes in performing examination History Fail to identify the patient first Make an incomplete history Provide a disorganized history Physical exam: Fail to describe general condition & vital signs first Incomplete description of features, e.g. pulse rate only or respiratory rate only without further characteristics

76
How can you be a good examiner?
THINK, PRACTICE, PRACTICE !!!

77
Thank you

Similar presentations















MRCP(LONDON) ASSOCIATE PROFESSOR MEDICINE.>")















