Download presentation
Presentation is loading. Please wait.

1
Stress, Injury, PED’s and Burnout
Problems in Sport Stress, Injury, PED’s and Burnout

2
Stress and Injury Stress is leading cause of injury, misuse of PED’s and burnout Finch et al (1998): 20-30% of total injuries in a given population are sports related Research: increased stress in life = increased injury in sports Smith et al (1990): 452 m/f high school athletes, assessed stress, social support, coping skills and # of days off related to injury Results showed a correlation between stressors and injury, other factors included low social support and low coping skills
: 20-30% of total injuries in a given population are sports related. Research: increased stress in life = increased injury in sports. Smith et al (1990): 452 m/f high school athletes, assessed stress, social support, coping skills and # of days off related to injury. Results showed a correlation between stressors and injury, other factors included low social support and low coping skills.")
4
Explaining the Relationship Between Stress and Injury
Williams et al (1991); stress disrupts attention, reduces peripheral awareness Anderson & Williams (1999): negative life event stressors were the only significant predictor of injury in 196 college athletes Smith et al (2000): muscle tension caused by stress interferes with normal coordination, thus increasing rick of injury
; stress disrupts attention, reduces peripheral awareness. Anderson & Williams (1999): negative life event stressors were the only significant predictor of injury in 196 college athletes. Smith et al (2000): muscle tension caused by stress interferes with normal coordination, thus increasing rick of injury.")
5
Stress and Recovery Cramer et al (2000): natural healing disrupted by high glucocorticoids, impairing the immune response and inhibiting production of growth hormones Cortisol inhibits recovery of damaged tissues Perna et al (2003): stress caused impaired sleep patterns and protein synthesis-essential for recovery process
: natural healing disrupted by high glucocorticoids, impairing the immune response and inhibiting production of growth hormones. Cortisol inhibits recovery of damaged tissues. Perna et al (2003): stress caused impaired sleep patterns and protein synthesis-essential for recovery process.")
7
Responding To Injury Grief Response Model (Hardy, Crace, 1990)
Coping with 3 stressors (Physical, Psychological and Social) essential to rehab process takes one of 2 forms Denial: injured players pushes it and make it worse Anger: about injury’s impact on ability/career Bargaining: deal making to mitigate the injury Depression: reality of injury Acceptance/reorganization: coping can begin Similar to Kubler-Ross 5 Stages of Grief Petitpas & Danish (1995): Identity Loss—injury low self –efficacydepressionlow self confidencelow status and motivationidentity loss
 essential to rehab process takes one of 2 forms. Denial: injured players pushes it and make it worse. Anger: about injury’s impact on ability/career. Bargaining: deal making to mitigate the injury. Depression: reality of injury. Acceptance/reorganization: coping can begin. Similar to Kubler-Ross 5 Stages of Grief. Petitpas & Danish (1995): Identity Loss—injury low self –efficacydepressionlow self confidencelow status and motivationidentity loss.")
8
Cognitive Appraisal Model (Urdy et al, 1997)
“Information Processing” About Injury (Urdy et al) Stage 1: Amount/type of pain, how/why it happened, consequences and rehab options Stage 2: emotional upheaval, reactive behaviors—anger, frustration Stage 3: Developing, outlook and coping
 Stage 1: Amount/type of pain, how/why it happened, consequences and rehab options. Stage 2: emotional upheaval, reactive behaviors—anger, frustration. Stage 3: Developing, outlook and coping.")
9
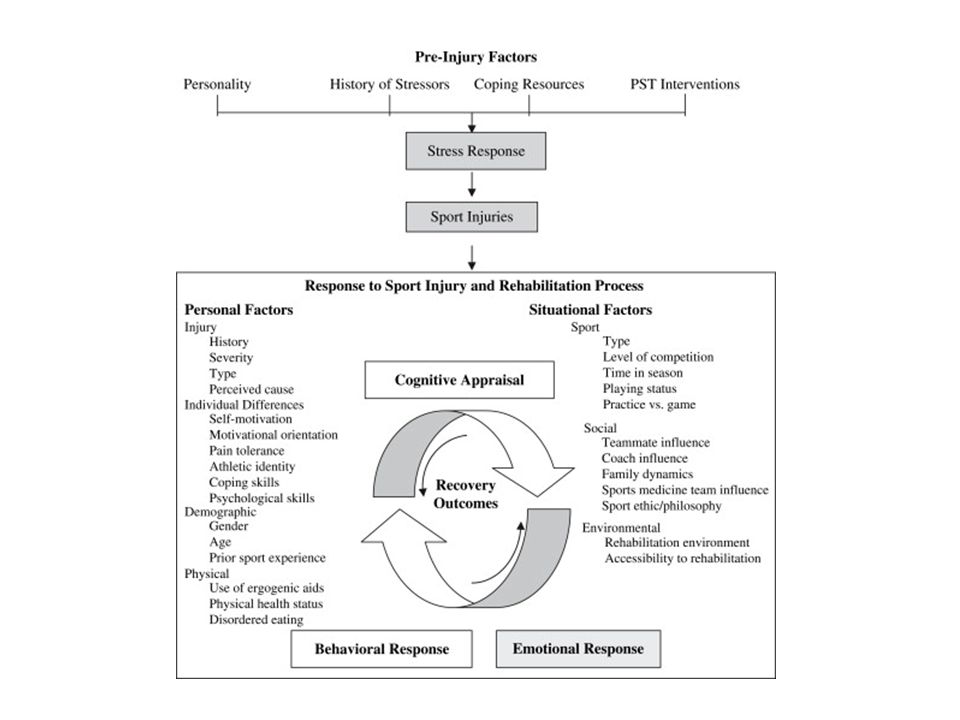
Cognitive Appraisal Model (Wiese, Bjornstal, 1998)
Primary Appraisal: what is at stake, challenge, threat, benefit or loss Secondary Appraisal: how can you cope, options available

11
PED use in last 20 Years Physical considerations
Strength, endurance, alertness, aggression, fatigue, anxiety, wt. gain/loss all can be impacted by PED’s Psychological considerations Coping w/stress, self esteem, confidence, respond to external pressures

12
Social considerations
Social learning theory: see model (Bonds, Canseco, Ben Johnson) do it without getting caught (Bandura; Anshel, 1998) Conformity, coercion, peer pressure “Game Theory” (Axelrod, 1984): if you don’t use you will be left behind by the using competition (e.g. EPO doping in the Tour de France, roids in MLB), leads to cognitive rationalization that the rewards outweigh the risks of getting caught
 do it without getting caught (Bandura; Anshel, 1998) Conformity, coercion, peer pressure. Game Theory (Axelrod, 1984): if you don’t use you will be left behind by the using competition (e.g. EPO doping in the Tour de France, roids in MLB), leads to cognitive rationalization that the rewards outweigh the risks of getting caught.")
14
Physical Effects of Steriods
synthetic derivatives of testosterone, anabolic effects retention of protein to build muscle “stacking”: combo of different types can be permanent Injections increase risk of Hepatitis B, HIV Damage may take years to see (Lyle Alzado) Feminization Effect in men Women have “Masculinization Effect” Acne, wt. gain, liver damage, heart attack, stroke, increased cholesterol, weak tendons (see Bo Carrol), permanent growth halt in teens in both males and females
 Feminization Effect in men. Women have Masculinization Effect Acne, wt. gain, liver damage, heart attack, stroke, increased cholesterol, weak tendons (see Bo Carrol), permanent growth halt in teens in both males and females.")
16
Psychological Effects of Steroids
Mood swings, extreme irritability/aggression (“roid rage”), addiction and withdrawal issues
, addiction and withdrawal issues.")
17
Effects of Other PED’s Beta blockers: reduce anxiety, blood pressure, heart rate, depresses CNS Diuretics: wt. loss, dehydration, cramping, kidney stones, increased cholesterol EPO (erythropoietin): increased oxygen and stamina, risks for blood clots, heart attack, stroke Narcotics: mask pain, failure to feel injury, overdose threat
: increased oxygen and stamina, risks for blood clots, heart attack, stroke. Narcotics: mask pain, failure to feel injury, overdose threat.")
18
Causes of Burnout Cognitive-Affective Stress Model (Smith 1986) how thoughts and feelings influence athlete’s burnout Stage 1: Situation Demands: demands exceed resources = stress Stage 2: Cognitive Appraisal: threat vs. challenge appraisal of situation = anxious or excited Stage 3: Physiological Responses: fight or flight due to appraisal Stage 4: Behavioral Response: performance issues, cohesion problems, withdrawal

19
Hardiness (Kobasa, 1986) is the key factor to overcoming stressors and resisting burnout; based on 3 factors Control: person’s ability to influence events Commitment: person’s refusal to give up Challenge: person’s willingness to change

20
Mental Toughness Model (Clough and Earle, 2001)
Mental toughness questionnaire resulted in a group of mentally tough subjects and non mentally tough who then did 3 30 minute cycling trials at 30, 50 and 70% max; oxygen uptake and reactions of subjects was recorded Results showed MT subjects reported lower perceived exertion, even at 70% suggesting MT helps withstand stress/burnout

21
Self Determination Theory (Raedeke, 1997)
Burnout results from lack of intrinsic motivation or control over participation; “have to” rather than “get to” attitude Factors include: identity = sport, entrapment, social support/demands

22
Preventing Burnout Cognitive Affective Stress Management (Smith, 1980)
Mental/physical coping strategies designed to prevent burnout in 4 steps Pre-treatment Assessment: interviews to assess the athlete’s stress response and appraisal Treatment Rationale: athlete analyzes and gains understanding of personal stress reactions Skill Acquisition: athlete learns relaxation, cognitive restructuring and self talk Skill Rehearsal: stress is induced to allow athlete to practice new stress reducing skills

23
Stress Inoculation Theory (SIT) Meichenbaum, 1985
Athlete is exposed to increasing levels of stress in 3 stages, thereby enhancing his/her immunity “Learned Resourcefulness” Stage 1: Conceptualization: athlete becomes aware of +/-- thoughts, self talk, imagery Stage 2: Rehearsal: practice Stage 3: Application: athlete encounters low stress and then moves up to moderate then high and applies what was rehearsed in stage 2 Prepare--control--cope--evaluate--overcome

Similar presentations







 that is believed to enhance one’s performance above normal standards The IOC definition: “The administration or use of substances.>")

 Cognitive-affective stress management Training (SMT) Systematic Desensitization Self-talk strategies.>")












