Download presentation
Presentation is loading. Please wait.

1
Psychological Disorders
Chapter 13 Psychological Disorders 1-

2
Discuss: What is your definition of “abnormal behavior”? Or, what constitutes abnormal behavior? What is “normal behavior”?

3
Instructions: Write "A" over the blank if you think that the behavior being described can be classified as abnormal, and "N" if you believe that it is reasonably normal. 1. A pregnant woman is so afraid of sleeping near a window as she believes that a manananggal will come to take her unborn baby away. She is able to sleep well for as long as she stays away from any opening in their house. N Although this behavior may constitute delusional thinking in some cultures, it is a widespread folk belief in our culture. Most Filipino professionals will not consider this abnormal for as long as there is no impairment in functioning, and the pregnant woman is not preoccupied with the thought that her unborn child will be taken. 2. When he was a young child, Kenneth witnessed a violent fight between his father and mother, which eventually led into their separation. At that point, a bird flew right before him. Since then, he would tremble in fear at the sight of any kind of bird. In other situations, however, he seems to function like everyone else. A This is an example of a phobia. Many irrational fears like this are strictly confined to the target object, which have been associated with the traumatic event. 3. Whenever he comes home, Jon has the routine of going through each room in his house cleaning and fixing every single fixture. His routine often takes him about 2 hours although he has a domestic helper who cleans his house everyday. A Some people who suffer from obsessive compulsive disorder may manifest this behavior. They feel that they need to be clean, and their surroundings neat at all times, even if their routines take up so much of their time. They just can't help themselves.

4
4. Ben is only 7 years old. He saw a nice, expensive ballpen lying around the living room of his uncle's house. He took it home without asking permission. When asked by his parents where he got the pen, he casually (and guiltlessly) answered where. N Although many parents may consider this stealing, it is actually not. A child developmentally needs to learn a sense of proprietorship, and can have some lapses like this. Children who steal habitually usually fear being reprimanded, and so lie about the origin of the object in question. 5. Henry is now 10 years old. He has been having school problems since he was younger, as he cannot keep still in his seat. While listening to the teacher's lecture, Henry's attention cannot be sustained, so he starts talking to his seatmates, draws on his notebook, or stands up and goes around the classroom. During a 40-item test, Henry was only able to complete 10 items in the test, despite demonstrating adequate understanding of the instructions. A Henry shows some symptoms of a child suffering from Attention-Deficit/Hyperactivity Disorder: inattention, hyperactivity and impulsiveness. 6. Jenny firmly believes that there is a family of duwendes living in her backyard. She often leaves toys and food outside for them to enjoy. N Belief in duwendes is accepted in our culture. Moreover, for as long as this belief does not disrupt the everyday functioning of the people in her household, this may not be considered a delusion.

5
7. Gina is devastated and attempts to commit suicide by slashing her wrists with a blade after her boyfriend broke up with her. A Although this attempt appears to be a call for attention, it is an act characterizing a person who is highly unstable. While suicides are usually associated with people who are feeling depressed, it is also a symptom of people who suffer from Borderline Personality Disorder. 8. Troy often forgets his things. He usually comes to school without his homework, and often loses his ballpens and notebooks. N Although this forgetfulness can be a form of cognitive loss that may be due to another medical condition, it cannot be considered a mental illness on its own. There are some techniques that can be used by Troy in order to overcome his absent-mindedness. 9. Everyday for the past 2 months, after coming home from work, Ronnie locks himself in his bedroom and takes shabu while watching television. All his salary goes to the drugs. He then wakes up early to go to work the next day and takes pains to ensure that no one finds out about his drug abuse. A Although Ronnie's work may not seem to be affected by his drug abuse, other areas of his life are already negatively affected by his addiction: his inability to stop spending his salary all on drugs, his social isolation by spending all his free time alone in his room, and lying to others about his drug abuse by making sure that no one finds out.

6
10. When she is in a bad mood, which is almost every day, Tina cannot help but exhibit temper tantrums. A This volatile emotionality can be seen among many people suffering from Borderline Personality Disorder or an impulse control problem. They are easily provoked, and have difficulty controlling their anger. 11. When asked what her name was, Abel answered that the "moon jumped together with the sun over the rainbow". A This shows disorganized thought as a disturbance in the form of thought of a person suffering from Schizophrenia. 12. Without any effort to diet, Lily loses at least 5% of her body weight every month for a period of about 3 months. A Depression usually brings about either a sudden weight gain or loss.

7
Abnormal behavior What is abnormal behavior?
Deviation from statistical norms Ex. Extremely low IQ scores Deviation from social norms Maladaptiveness of behavior Ineffective, unproductive, unlawful Affect daily functioning/relationships Level of personal distress

8
Abnormal behavior What is normal behavior? (“well-adjusted”)
Efficient perception of reality Ability to exercise voluntary control over behavior Ability to form affectionate relationships Productivity

9
Attention deficit in an 8-year old child – A) statistical deviation – a behavioral symptom of AD/HD in children, 8-year olds are developmentally expected to be able to focus on tasks for at least 15 minutes, so this is an atypical lag for a child this age Depression – D) personal distress – a person suffering from depression may feel anxious, numb, have loss of appetite, and may have some aches and pains. Loss of memory of one’s childhood – A) statistical deviation – A symptom of DID, this may not cause personal distress and may not be maladaptive, but it is certainly statistically uncommon for people not to remember whole chunks of their childhood
 statistical deviation – A symptom of DID, this may not cause personal distress and may not be maladaptive, but it is certainly statistically uncommon for people not to remember whole chunks of their childhood .")
10
Frequent alcohol intoxication –
Frequent alcohol intoxication – A) social norms - Social norms encourage drinking only in moderation; frequently getting intoxicated from alcohol is unacceptable Preference to be alone and avoid any social contact – C) maladaptive behavior – “No man is an island” as the song goes; human beings are also social beings as they contribute something to keep society progressive and productive; by preferring to be alone and avoiding social contact, the person deprives oneself and society of maximizing his or her gifts and talents Belief that one is sick and needs medical attention even when there are no physical evidence to support this – C) maladaptive behavior – only persons who are truly sick will seek intervention for their illness
 social norms - Social norms encourage drinking only in moderation; frequently getting intoxicated from alcohol is unacceptable. Preference to be alone and avoid any social contact – C) maladaptive behavior – No man is an island as the song goes; human beings are also social beings as they contribute something to keep society progressive and productive; by preferring to be alone and avoiding social contact, the person deprives oneself and society of maximizing his or her gifts and talents. Belief that one is sick and needs medical attention even when there are no physical evidence to support this – C) maladaptive behavior – only persons who are truly sick will seek intervention for their illness.")
11
Early Explanations of Mental Illness
In ancient times holes were cut in an ill person’s head to let out evil spirits in a process called trepanning. In the Middle Ages, the mentally ill were labeled as witches. Menu

12
Understanding Psychological Disorders
Theoretical Approaches to Psychological Disorders The Biological Approach Medical Model Structural Views Biochemical Views Genetic Views Medical Model A biological approach that describes psychological disorders as medical diseases with a biological origin. 1-

13
Understanding Psychological Disorders
Theoretical Approaches to Psychological Disorders The Psychological Approach Psychoanalytic Perspective Behavioral and Social Cognitive Perspective Humanistic Perspective 1-

14
Understanding Psychological Disorders
The Causes of Psychological Disorders Sociocultural Factors An Interactionist Approach: Bio-Psycho-Social

15
Culture-Related Disorders

16
LO 14.7 Types of psychological disorders
Menu

17
LO 14.7 Types of psychological disorders
Menu

18
DSM: Classifying Abnormal Behavior
DSM-IV Stands for Diagnostic and Statistical Manual of Mental Disorders, fourth edition; the most recent major classification of psychological disorders. Classifying Abnormal Behavior Axis I: All Categories Except Personality Disorders and Mental Retardation primary diagnosis Axis II: Personality Disorders and Mental Retardation other long-standing psych condition Axis III: General Medical Conditions physical Axis IV Psychosocial and Environmental Problems personal difficulties/stressful events that precipitated disorder Axis V Current Level of Functioning On a scale of 100: assess general level of functioning

19
DSM Diagnostic Categories
Disorders usually first diagnosed in infancy, childhood, or adolescence Mental Retardation IQ tests Usually genetic factors, head trauma, infection, toxic substances Learning Disorders lag in reading, writing, math Pervasive Developmental Disorders severe impairment, odd behavior Ex. Autism – hand-flapping, poor eye contact, prefer to play alone High-functioning autistic – may attend regular schools Savant Attention-Deficit/Hyperactivity Disorder (ADHD) Lack of focus, hyperactivity, poor impulse control
 Lack of focus, hyperactivity, poor impulse control.")
20
DSM Delirium, dementia, amnestic, & other cognitive disorders
Impairment of brain functioning (aging etc.) Mental disorders due to a general medical condition Consequence of a medical condition Substance-related disorders Effects of meds, drug abuse, toxic substances Schizophrenia and other psychotic disorders Impairment of reality testing, bizarre behavior, highly disordered thought processes Delusions (false beliefs) “I am Napoleon!” Hallucinations (false sensory perceptions)
 Mental disorders due to a general medical condition. Consequence of a medical condition. Substance-related disorders. Effects of meds, drug abuse, toxic substances. Schizophrenia and other psychotic disorders. Impairment of reality testing, bizarre behavior, highly disordered thought processes. Delusions (false beliefs) I am Napoleon! Hallucinations (false sensory perceptions)")
21
Schizophrenia

22
Schizophrenia Menu

23
Probability of Developing Schizophrenia
1-

24
Schizophrenia Causes of Schizophrenia Biological Factors
Heredity Structural Brain Abnormalities Neurotransmitter Deregulation Psychological Factors Diathesis-Stress Model Sociocultural Factors Diathesis-Stress View Argues that a combination of biogenetic disposition and stress cause schizophrenia. 1-

25
Mood disorders Menu

26
DSM Mood disorders Psychological disorders in which there is a primary disturbance in mood. Prolonged emotion that colors the individuals entire emotional state. Two main types are the depressive disorders and bipolar disorder. Depressive disorder – sadness, loss of gratification, negative thoughts, lack of motivation Bipolar disorder – alternate bouts of depression & mania

27
DSM Major Depressive Disorder – must have 5 of the 9 symptoms during a 2 week period Depressed mood for most of the day Reduced interest or pleasure in most activities Significant weight loss or gain, significant decrease or increase in appetite Trouble sleeping or sleeping too much Psychomotor agitation or retardation Fatigue or loss of energy Feeling worthless or guilty in an excessive or inappropriate manner Problems thinking, concentrating, or making decisions Recurrent thought of death or suicide

28
DSM Depression/Mood Disorders Psychoanalytic
Reaction to loss; anger towards self Behavioral Lack of positive reinforcement Negative experiences throughout life Learned Helplessness Cognitive How people view themselves or the world Biological Heredity Neurophysiological Abnormalities Neurotransmitter Deregulation Hormones Sociocultural Factors Interpersonal Relationships Socioeconomic and Ethnic Factors Cultural Variations Gender

29
Mood Disorders Major Depressive Disorder
Gender Differences in Depression Across Cultures

30
Mood Disorders Bipolar Disorder

31
PANIC! PANIC! PANIC! PANIC!
Anxiety Disorders sweating racing heart chest pain shortness of breath dizziness nausea hot flashes/chills trembling terror desire to escape PANIC! PANIC! PANIC! PANIC! Menu

32
Anxiety disorders include these features: motor tension, hyperactivity, and apprehensive expectations and thoughts. Generalized Anxiety Disorder An anxiety disorder that consists of persistent anxiety for at least one month; the individual with this disorder cannot specify the reasons for the anxiety. Panic Disorder An anxiety disorder marked by the recurrent sudden onset of intense apprehension or terror. Agoraphobia A cluster of fears centered around public places and being unable to escape or find help should one become incapacitated. Phobic Disorder Commonly called phobia, an anxiety disorder in which the individual has an irrational, overwhelming, persistent fear of a particular object or situation. Obsessive-Compulsive Disorder (OCD) An anxiety disorder in which the individual has anxiety-provoking thoughts that will not go away (obsession) and/or urges to perform repetitive, ritualistic behaviors to prevent or produce some future situation (compulsion). DSM
 An anxiety disorder in which the individual has anxiety-provoking thoughts that will not go away (obsession) and/or urges to perform repetitive, ritualistic behaviors to prevent or produce some future situation (compulsion). DSM.")
33
Anxiety Disorders Post-Traumatic Stress Disorder (PTSD) PTSD Symptoms
Combat and War-Related Traumas Abuse Natural and Unnatural Disasters Post-Traumatic Stress Disorder (PTSD) An anxiety disorder that develops through exposure to a traumatic event, such as a war; severely oppressive situations, such as the holocaust; severe abuse, as in rape; natural disasters, such as floods and tornados; and accidental disasters, such as plane crashes. 1-
 An anxiety disorder that develops through exposure to a traumatic event, such as a war; severely oppressive situations, such as the holocaust; severe abuse, as in rape; natural disasters, such as floods and tornados; and accidental disasters, such as plane crashes. 1-")
34
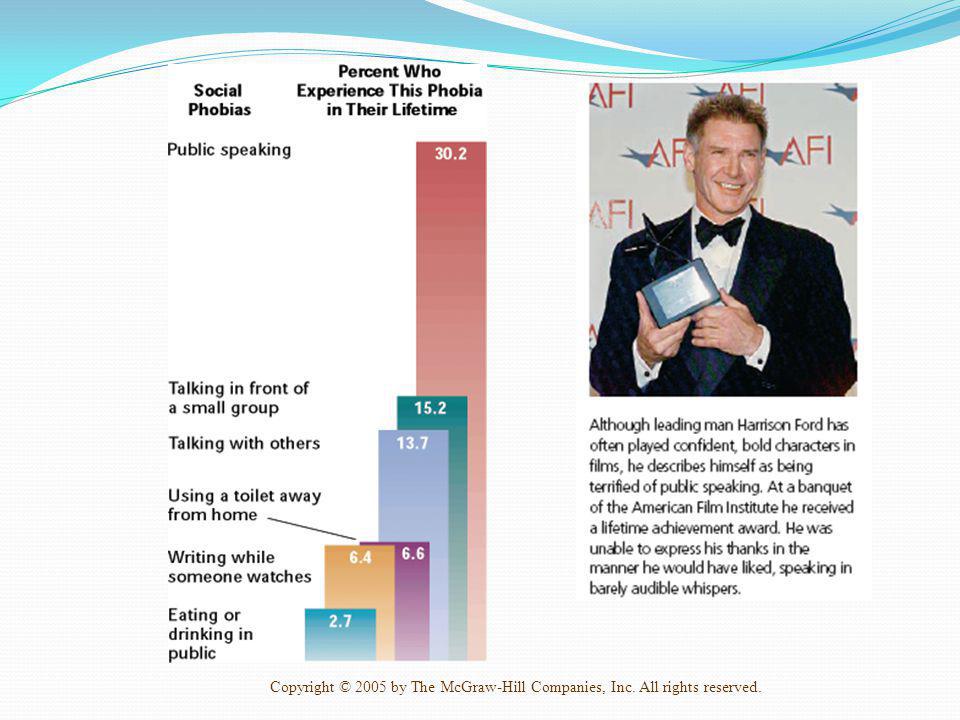
Phobias 1-

36
DSM Anxiety disorders Psychoanalytic
Punitive disciplining strategy while toilet-trained Behavioral Phobia was a learned response Cognitive Thoughts? Overestimation of the feared event. Belief that rituals will prevent disaster. Biological

37
DSM Somatoform disorders Factitious disorders Dissociative disorders
Physical symptoms with no biological basis Factitious disorders Intentionally feigning symptoms with no apparent gain Dissociative disorders Psychological disorders that involve a sudden loss of memory or change in identity.

38
Types of somatoform disorders
Menu

39
DSM Dissociative disorders
Dissociative Amnesia A dissociative disorder involving extreme memory loss caused by extensive psychological stress. Dissociative Fugue A dissociative disorder in which the individual not only develops amnesia but also unexpectedly travels away from home and establishes a new identity. Dissociative Identity Disorder (DID) Formerly called multiple personality disorder, this is the most dramatic but least common dissociative disorder; individuals suffering from this disorder have two more distinct personalities or selves.
 Formerly called multiple personality disorder, this is the most dramatic but least common dissociative disorder; individuals suffering from this disorder have two more distinct personalities or selves.")
40
DSM Dissociative disorders
Many have experienced sexual or physical abuse as children Why create new identities in such a situation?

41
DSM Sexual & gender identity disorder Eating disorders Sleep disorders
Distress over sexual identity, sexual performance Eating disorders Self-induced starvation, binge eating, innaccurate perception of body image Sleep disorders Impulse control disorders Anger, gamble, set things on fire, pull one’s hair, steal

42
DSM Adjustment disorders
psychological response from an identifiable stressor or group of stressors that causes significant emotional or behavioral symptoms that does not meet criteria for more specific disorders like loss of a boyfriend, a poor report card, or moving to a new

43
DSM Personality disorders
Chronic, maladaptive cognitive-behavioral patterns that are thoroughly integrated into the individual's personality. Paranoid Sensitivity to rejection, resentfulness, distrust, as well as the inclination to distort experienced events. Neutral and friendly actions of others are often misinterpreted as being hostile or contemptuous. Histrionic attention-seeking and excessively dramatic behaviors Narcissistic grandiose sense of self-importance; preoccupied with fantasies of unlimited success, power, brilliance, beauty, or ideal love ; sense of entitlement

44
DSM Personality disorders
Antisocial lack of remorse, morality commit crimes Passive-aggressive Pattern of negativistic attitude, passive resistance to perform adequately Procrastination, stubbornness, and forgetfulness Borderline psychological instability, fear of abandonment; have unstable moods, relationships; high number experienced abuse as children Other conditions that may be the focus of clinical attention

45
Neurotic? Or Psychotic? Neuroses – feelings of anxiety etc.
Psychoses – loss of contact with reality Delusions (false beliefs) Hallucinations (false sensory perceptions) Ex. Dr. John Nash Ex. Psychotic depression, Neurotic depression
 Hallucinations (false sensory perceptions) Ex. Dr. John Nash. Ex. Psychotic depression, Neurotic depression.")
46
DSM Evaluation Use of Labels The medical model disease Culture

47
Explaining Abnormal Behavior
Biological perspective Ex. Depression (Psychiatrist, Psychologist) Psychoanalytic perspective Unconscious conflicts/ maladaptive use of defense mechanisms Behavioral perspective Learned Cognitive perspective mental processes Biopsychosocial approach interactionist
 Psychoanalytic perspective. Unconscious conflicts/ maladaptive use of defense mechanisms. Behavioral perspective. Learned. Cognitive perspective. mental processes. Biopsychosocial approach. interactionist.")
48
SUICIDE Discuss: What do you think of people who think of committing suicide or have actually committed suicide? Have you ever had to deal with a friend with suicidal thoughts? What did you say to the person? Have you personally ever thought of committing suicide? If so, how far did you go in terms of thought process or behavior?

49
Suicide Philippines, commonly used: Paracetamol Bleach Pesticides
Prescription drugs Muriatic acid Also, Hanging, shooting oneself, carbon monoxide poisoning

50
Suicide Usually after a fight with family or boyfriend/girlfriend
Not all intend to die Hurt someone Gain attention Release tension In the U.S., suicide has quadrupled since 1950 Girls: 3x more attempts than boys Completed suicides: 5x higher among boys than girls

51
Suicide 1. People generally think about suicide.
Instructions: Write "T" over the blank if you think that the behavior being described is true and “F” if you think it is false. 1. People generally think about suicide. Ordinarily, people think about suicide at one point in time in their lives. This may happen especially during stressful moments. 2. A person who talks about committing suicide may seriously do it. While there are people who talk about suicide but do not attempt it at all, those who have a history of attempts are more likely to do it again. Moreover, if the person has detailed plans of how one will kill oneself and has easy access to materials to implement it, the more likely the attempt will be made. 3. A person who commits suicide usually warns others about it. Usually, a person warns others that he or she is thinking of committing suicide. It may be as clear as a threat or may be so subtle (i.e. said in a joking manner) such that it was easily dismissed and realized only in hindsight. 4. A number of people who commit suicide do not actually intend to die. While there are a number of people who intend to die when they commit suicide, others do it impulsively to cope with a stressful situation, to gain attention, to hurt someone back, or to relieve themselves of pain.
 such that it was easily dismissed and realized only in hindsight. 4. A number of people who commit suicide do not actually intend to die. While there are a number of people who intend to die when they commit suicide, others do it impulsively to cope with a stressful situation, to gain attention, to hurt someone back, or to relieve themselves of pain.")
52
Suicide 5. If one has a history of previous suicide attempts, he may likely do it again. Those who have attempted suicide in the past are more likely to do so again especially if proper aftercare and treatment was not given and the person has not learned better and healthier coping skills needed. 6. It is difficult to identify a person who is likely to commit suicide. Sudden changes in a person's behavior especially a display of depressive symptoms may be a warning that he or she wants to commit suicide. At other times, however, one can barely see any change in behaviors as the person who later attempts went normally about his or her daily routine right before it. 7. Talking with the person about his or her suicidal thoughts and plans may help the person abandon his or her plans of actually putting these thoughts into action. During this stressful moment, a person who thinks of suicide may be in great need of someone who shows compassion and care. Being able to talk about it to someone may also relieve him or her of anxiety and may make him or her feel understood. 8. A person who commits suicide may suffer from a mental disorder. Studies show that a number of people who commit suicide are diagnosed to have depression, borderline personality disorder, schizophrenia, or substance abuse. With the correct diagnosis, proper treatment may be given to them. Note: All answers on the worksheet are T for True

53
Suicide

54
Instructions: For each of the following brief case studies, identify the disorder.
1. Edwina is worried, anxious, and sure that something terrible is going to happen to her. She’s not sure what it would be, but she “just knows.” The feeling occurs on almost a daily basis and frequently keeps her awake at night. In addition, for the last few weeks, she has been plagued with chronic headaches, upset stomachs, and upper back pain. 2. Last week, Roger suddenly quit his job. He told his family he had decided to learn carpentry. He purchased a truckload of wood and nails, which now sits in his driveway because he changed his mind and decided to enroll in a school for massage therapy. The school confirms that he registered but that he has not attended class. Roger claims that he can learn all he needs simply from reading the books. For the last three days, he has not slept. He started to read the massage therapy books but became so upset by the lack of quality photos in the texts that he bought a camera. Today, he is taking photos for his new career as a photojournalist. 3. George enters the clinic with his wife who says she “can’t take it anymore!” She states that George is carrying around a notebook in which he is constantly scribbling cryptic notes about everyone that he meets. He is parking his car a few blocks away from the house so he can watch who drives down the street and past his home. Yesterday, he came home early and taped all the shades down over the windows in the house.

55
4. Susanna appears in court this morning on check forgery charges
4. Susanna appears in court this morning on check forgery charges. She is dressed in a black leather miniskirt, thigh-high black boots, a bright red, low-cut tank top, and earrings with bells that jingle when she moves. Throughout the proceedings, Susanna methodically files her fingernails. She adamantly states that she is not to blame for writing the bad checks despite the fact that she admits to stealing them from her father and signing his name. She makes it clear that her father owes her the money because he refused to pay for medical school (despite the fact that she never graduated from college) and ruined her career as a brilliant physician. 5. Anichka was walking her dog when suddenly and without warning, her heart began to pound, her legs began to tremble, and she became very dizzy. She was convinced she was having a heart attack right there on the street. 6. Noah is having trouble staying awake at work. Throughout the night he hears someone that tells him something is on fire in the house. He has been getting up 15 to 20 times during the night to check for smoke and to check the smoke alarm.
 and ruined her career as a brilliant physician. 5. Anichka was walking her dog when suddenly and without warning, her heart began to pound, her legs began to tremble, and she became very dizzy. She was convinced she was having a heart attack right there on the street. 6. Noah is having trouble staying awake at work. Throughout the night he hears someone that tells him something is on fire in the house. He has been getting up 15 to 20 times during the night to check for smoke and to check the smoke alarm.")
56
7. John is seen in the emergency room because his mother brought him in. He is dressed in a blue baseball cap, red striped pajamas, army combat boots, and large women’s clip-on earrings. He claims he has been “swatting sprocketgens” and “pounding the batjunkins with rose perfume.” 8. Maurice is sleeping 12 to 16 hours a day. Over the last two months, his weight has dropped 10 pounds, and he feels as if it takes all his effort to fix a simple bowl of soup. He feels as if he is sitting at the bottom of a hole and simply can’t climb out.

Similar presentations
>")


















