Download presentation
Presentation is loading. Please wait.

1
HEART FAILURE IN NEONATE AND INFANT

2
Congestive heart failure (CHF) refers to a clinical state of systemic and pulmonary congestion resulting from inability of the heart to pump as much blood as required for the adequate metabolism of the body. Clinical picture of CHF results from a combination of “relatively low output” and compensatory responses to increase it

3
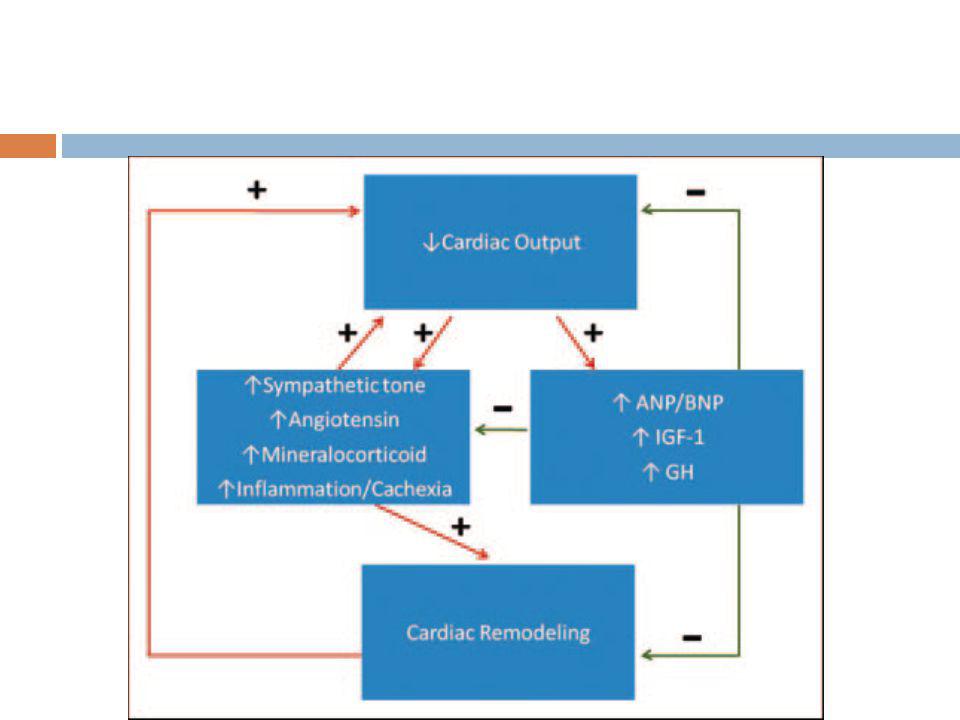
PATHOPHYSIOLOGY Unmet tissue demands for cardiac output result in activation of Renin-aldosterone angiotensin system Sympathetic nervous system Cytokine-induced inflammation “signaling” cascades that trigger cachexia.

5
Longstanding increases in myocardial work and myocardial
oxygen consumption (MVO2) ultimately worsen HF symptoms and lead to a chronic phase that involves cardiac remodeling
 ultimately worsen HF. symptoms and lead to a chronic phase that involves cardiac remodeling.")
6
CARDIAC REMODELING? Maladaptive cardiac hypertrophy
Expansion of the myofibrillar components of individual myocytes (new cells rarely form) An increase in the myocyte/capillary ratio Activation and proliferation of abundant nonmyocyte cardiac cells, some of which produce cardiac scarring Produce a poorly contractile and less compliant heart
 An increase in the myocyte/capillary ratio. Activation and proliferation of abundant nonmyocyte cardiac cells, some of which produce cardiac scarring. Produce a poorly contractile and less compliant heart.")
7
Endogenous mechanisms defend progressive HF
Stimulation of insulin like growth factor and GH ANP and BNP are hormones secreted by the heart in response to volume and pressure overload that increase vasodilation and diuresis acutely and chronically prevent inflammation, cardiac fibrosis and hypertrophy.

8
CLINICAL MANIFESTATIONS IN INFANTS WITH HF
Variety of age dependent clinical presentations In neonates, the earliest clinical manifestations may be subtle

9
CLINICAL MANIFESTATIONS IN INFANTS WITH HF
Pulmonary rales Peripheral edema Easy fatigability. Sweating Irritability failure to thrive. Feeding difficulties Rapid respirations Tachycardia Cardiac enlargement Gallop rhythm (S3) Hepatomegaly
 Hepatomegaly.")
10
Feeding difficulties & increased fatigability
Important clue in detecting CHF in infants Often it is noticed by mother Interrupted feeding (suck- rest -suck cycles) Infant pauses frequently to rest during feedings Inability to finish the feed, taking longer to finish each feed (> 30 minutes) Forehead sweating during feeds –due to activation of sympathetic nervous system –a very useful sign Increasing symptoms during and after feedings
 Infant pauses frequently to rest during feedings. Inability to finish the feed, taking longer to finish each feed (> 30 minutes) Forehead sweating during feeds –due to activation of sympathetic nervous system –a very useful sign. Increasing symptoms during and after feedings.")
11
Rapid respirations Tachypnea > 60/min in 0-2mth
>50/mt in 2mth to 1yr >40/mt 1-5 yr in calm child Happy tachypnea- tachypnea with out much retractions Grunting (a form of positive end-expiratory pressure) In cyanotic heart disease rapid respirations may be due to associated brain anoxia and not CHF -treatment for these two conditions is entirely different Fever especially with a pulmonary infection may produce rapid respirations.
 In cyanotic heart disease rapid respirations may be due to associated brain anoxia and not CHF -treatment for these two conditions is entirely different. Fever especially with a pulmonary infection may produce rapid respirations.")
12
Tachycardia Rate is difficult to evaluate in a crying or moving child
Tachycardia in the absence of fever or crying when accompanied by rapid respirations and hepatomegaly is indicative of HF Persistently raised heart rate > 160 bpm in infants > 100 bpm in older children. Consider SVT if heart rate > 220 bpm in infants and > 180 bpm in older children.

13
Cardiomegaly Consistent sign of impaired cardiac function, secondary to ventricular dilatation and/or hypertrophy. May be absent in early stages, especially with myocarditis, arrhythmias, restrictive disorders and pulmonary venous obstruction(obstructed TAPVC) Apex 4th space 1cm outside MCL in newborn
 Apex 4th space 1cm outside MCL in newborn.")
14
Hepatomegaly Lower edge of the liver is palpable 1 to 2 cms below right costal margin normally in infancy In the presence of respiratory infection increased expansion of the lungs displace liver caudally Usually in such circumstances the spleen is palpable Hepatomegaly is a sign of CHF Decrease in size is an excellent criterion of response to therapy

15
Pulmonary rales Of not much use in detecting CHF in infants
Rales may be heard at both lung bases When present are difficult to differentiate from those due to the pulmonary infection which frequently accompanies failure

16
Peripheral edema Edema is a very late sign of failure in infants and children Presacral and posterior chest wall edema in young infants It indicates a very severe degree of failure. Daily wt monitoring is useful in neonates -- rapid increase in wt > 30 gm /day may be a clue to CCF and is useful in monitoring response to treatment.

17
Cold extremity, low blood pressure, skin mottling are signs of impending shock
Pulsus alternans (alternate strong and weak contractions of a failing myocardium),or pulsus paradoxus (decrease in pulse volume and blood pressure with inspiration) are frequently observed in infants with severe CHF
,or pulsus paradoxus (decrease in pulse volume and blood pressure with inspiration) are frequently observed in infants with severe CHF.")
18
CLASSIFICATION NYHA Heart Failure Classification is not applicable
Ross Heart Failure Classification was developed for global assessment of heart failure severity in infants Modified to apply to all pediatric ages Modified Ross Classification incorporates Feeding difficulties Growth problems Symptoms of exercise intolerance

19
MODIFIED ROSS HEART FAILURE CLASSIFICATION FOR CHILDREN
Asymptomatic Class II Mild tachypnea or diaphoresis with feeding in infants Dyspnea on exertion in older children Class III Marked tachypnea or diaphoresis with feeding in infants Marked dyspnea on exertion Prolonged feeding times with growth failure Class IV Symptoms such as tachypnea, retractions, grunting, or diaphoresis at rest

20
The time of onset of CHF holds the key to the etiological diagnosis in this age group

21
Parallel circulation becomes series at birth
Cardiac anomalies present at that point are Critical AS HLHS Mitral atresia

22
Functional closure PDA 1 to 2weeks
PDA dependent lesions ,depend on patent duct for either pulmonary blood flow- Fallots with pulmonary atresia systemic blood flow-IAA/COA mixing of systemic and pulmonary blood-TGA Present at 1 to 2weeks

23
Anatomic closure of PDA by 2to4 weeks
Coarctation of aorta

24
Pulmonary vascular resistance falls 4to 6weeks
Congestive heart failure due to L-R shunt Large VSD PDA ALCAPA

25
CHF in the fetus Disorders that are fatal in the immediate neonatal period are often well tolerated in the fetus due to the pattern of fetal blood flow (e.g. TGA) Causes of CHF in the fetus SVT Severe bradycardia due to CHB Anemia Severe TR due to Ebstein’s anomaly or MR from AV canal defect Myocarditis
 Causes of CHF in the fetus. SVT. Severe bradycardia due to CHB. Anemia. Severe TR due to Ebstein’s anomaly or MR from AV canal defect. Myocarditis.")
26
FETAL BLOOD FLOW

27
Most of these are recognized by fetal echo
Severe CHF in the fetus produces hydrops fetalis with ascites, pleural and pericardial effusions and anasarca. Digoxin or sympathomimetics to the mother may be helpful in cases of fetal tachyarrhythmia or CHB respectively.

28
Premature neonates PDA poor myocardial reserve Fluid overload

29
CHF on first day of life Myocardial dysfunction secondary to asphyxia, hypoglycemia, hypocalcaemia or sepsis are usually responsible for CHF on first day Few structural heart defects cause CHF within hours of birth HLHS, severe TR or PR, Large AV fistula TR secondary to hypoxia induced papillary muscle dysfunction or Ebstein’s anomaly of the valve Improves as the pulmonary artery pressure falls over the next few days

30
CHF in first week of life
Serious cardiac disorders which are potentially curable but carry a high mortality if untreated often present with CHF in the first week of life A sense of urgency should always accompany evaluation of the patient with CHF in the first week Closure of the ductus arteriosus is often the precipitating event Prostaglandins E1 should be utilised

31
Peripheral pulses and oxygen saturation (pulse oximeter) should be checked in both the upper and lower extremities A lower saturation in the lower limbs means right to left ductal shunting due to PAH or AAI ASD or VSD does not lead to CHF in the first two weeks of life, an additional cause must be sought (eg.COA or TAPVC).
.")
32
TGA no VSD -1ST week VSD and no PS-6-8 weeks Critical AS or PS Obstructive TAPVC Adrenal insufficiency due to enzyme deficiencies or neonatal thyrotoxicosis could present with CHF in the first few days of life

33
ALPROSTODIL Prostaglandins E1 Maintain patency of ductus
Cyanotic lesions TGA LT sided obstructive lesions HLHS, critical AS,COA,IAA Available as inj 500microgm/ml IV 0.05 to0.1microgm /kg/min 0.01 to 0.05 microgm /kg/min maintainance Vasodilation of all arteries including ductus

34
Monitor spo2,RR, HR,BP,ECG,temp
Complications apnea, Seizure Hypotension Bradycardia Tachycardia cardiac arrest fever Extravasation may cause sloughing and necrosis

35
CHF beyond second week of life
Most common cause of CHF in infants is VSD Presents around 6-8 weeks of age. Left to right shunt increases as the PVR falls Murmur of VSD is apparent by one week Full blown picture of CHF occurs around 6-8 weeks. Other left to right shunts like PDA present similarly Fall in PVR is delayed in presence of hypoxic lung disease and at high altitude and can alter the time course Spontaneous improvement in CHF -development of obstructive pulmonary arterial hypertension even in early childhood

36
ALCAPA a rare disease in this age group
It is curable As the pulmonary artery pressure decreases in the neonatal period, these babies suffer from episodes of excessive crying with sweating (angina) and myocardial infarction. ECG shows pathologic q waves Often misdiagnosed as having “dilated cardiomyopathy”
 and myocardial infarction. ECG shows pathologic q waves. Often misdiagnosed as having dilated cardiomyopathy")
37
CAUSES OF HF IN CHILDREN
CARDIAC Congenital structural malformations ● Excessive Preload ● Excessive Afterload ● Complex congenital heart disease No structural anomalies ● Cardiomyopathy ● Myocarditis ● Myocardial infarction ● Acquired valve disorders ● Hypertension ● Kawasaki syndrome ● Arrhythmia (bradycardia or tachycardia) NONCARDIAC ● Anemia ● Sepsis ● Hypoglycemia ● Diabetic ketoacidosis ● Hypothyroidism ● Other endocrinopathies ● Arteriovenous fistula ● Renal failure ● Muscular dystrophies
 NONCARDIAC ● Anemia ● Sepsis ● Hypoglycemia ● Diabetic ketoacidosis ● Hypothyroidism ● Other endocrinopathies ● Arteriovenous fistula ● Renal failure ● Muscular dystrophies")
38
CONGENITAL STRUCTURAL MALFORMATIONS

39
VOLUME OVERLOAD (EXCESSIVE PRELOAD)
Left-to-right shunting VSD PDA AP window AVSD ASD(rare) Total/Partial Anomalous Pulmonary Venous Connection AV or semilunar valve insufficiency AR in bicommissural aortic valve/after valvotomy MR after repair of AVSD PR after repair of TOF Severe TR in Ebstein anomaly
 Total/Partial Anomalous Pulmonary Venous Connection. AV or semilunar valve insufficiency. AR in bicommissural aortic valve/after valvotomy. MR after repair of AVSD. PR after repair of TOF. Severe TR in Ebstein anomaly.")
40
Right-sided volume loading
Large ASD or anomalous pulmonary vein connections Congenital or surgically acquired PR especially if downstream pulmonary arterial narrowing Highly compliant RV accepts significant volume -without increasing filling pressure Rarely causes HF early in life

41
PRESSURE OVERLOAD (EXCESSIVE AFTERLOAD)
Left sided obstruction Congenital AS Aortic coarctation Lethal arrhythmias - severe afterload stress? ?HTN Right-sided obstruction Severe PS

42
Left heart obstructive lesions
First postnatal week-ductus arteriosus closes Increased LVEDP and a decreased pressure gradient between the aorta and ventricle at end-diastole produce subendocardial ischemia due to inadequate coronary flow Increased afterload and subendocardial ischemia result in HF syndrome

43
COMPLEX CONGENITAL HEART DISEASE
Abnormal RV CCTGA D TGA Single ventricle physiology HLHS Unbalanced AVSD Post Fontan procedure

44
Often combined volume and pressure overload
Both systemic and pulmonary circulations can be affected Cyanosis in CCHD-risk of subendocardial ischemia contributing to impaired ventricular performance Molecular abnormalities in transcription factors that lead to congenital structural abnormalities – also associated with abnormal myocardial performance and arrhythmias

45
ABNORMAL RV In pediatric heart disease much of the pathology is due to an abnormal RV RV myocytes appear to be structurally identical to LV myocytes Differences in contraction compared to the LV are due to the shape of the RV and myocardial organization

46
Gene expression patterns are different in the RV and the LV, which may affect function.
Genes that affect angiotensin and adrenergic receptor signaling showed lower expression in the RV than the LV Genes that contribute to maladaptive signaling showed higher expression in the RV

47
Hypoplastic right heart syndromes -3 parts of the RV do not form normally or may be missing entirely. Defects in the IVS or abnormal LV function- Adversely affect the third phase of normal RV contraction through its interdependence on normal septal function

48
Volume overload of the RV
Can arise through significant PR or TR Compensatory dilation to decompensated dilation occur slowly

49
Increased RV afterload
RVOT obstruction RV serving as the systemic ventricle Usually can adapt if present at birth Once the RV assumes a mature, thin-walled configuration, it cannot always mount a hypertrophic response RV is able to support the systemic circulation for many years but function often deteriorates over time

50
SINGLE VENTRICLE PHYSIOLOGY
Ventricular morphology (left, right, indeterminate, or unbalanced) results in a single functional pumping chamber At birth presentation depends on the morphology Range from well-tolerated cyanosis to decompensated heart failure and cardiogenic shock double inlet ventricle(SV), HLHS , Tricuspid atresia, isomerism
 results in a single functional pumping chamber. At birth presentation depends on the morphology. Range from well-tolerated cyanosis to decompensated heart failure and cardiogenic shock. double inlet ventricle(SV), HLHS , Tricuspid atresia, isomerism.")
53
These factors can occur individually or in various combinations
Pathophysiological factors associated with heart failure in SV physiology in the newborn period are Unobstructed pulmonary blood flow Obstruction to systemic flow Obstruction to pulmonary venous return Insufficiency of the atrioventricular valve Myocardial abnormalities or dysfunction Coronary hypoperfusion. These factors can occur individually or in various combinations

54
Functional single ventricle heart is volume-loaded because of the need to supply the pulmonary and systemic circulations, until the creation of the cavo-pulmonary anastomosis at 6 months of age. Elevated BNP levels before the surgery; afterward, they return to normal

55
After the Fontan procedure
Diastolic filling properties often remain abnormal for some time Ventricular function depend on morphology Single RV has a lower mass: volume ratio which creates a relative increase in wall stress -poorer performance Single RV does not have the functional benefit of the interdependence with the LV and interventricular septum that the RV has in 2-ventricle physiology

56
Fontan procedure

57
Conduction and rhythm abnormalities is relatively high after Fontan procedure
Fontan procedure is often well-tolerated for many years As increasing numbers of these patients survive to adulthood, the prevalence of so-called Fontan failure is increasing

58
CHF WITH NO CARDIAC MALFORMATIONS
PRIMARY CARDIAC Cardiomyopathy Myocarditis Cardiac ischemia Acquired valve disorders Hypertension Kawasaki syndrome Arrhythmia (bradycardia or tachycardia) NONCARDIAC Anemia Sepsis Hypoglycemia Diabetic ketoacidosis Hypothyroidism Other endocrinopathies Arteriovenous fistula Renal failure Muscular dystrophies
 NONCARDIAC. Anemia. Sepsis. Hypoglycemia. Diabetic ketoacidosis. Hypothyroidism. Other endocrinopathies. Arteriovenous fistula. Renal failure. Muscular dystrophies.")
59
DISORDERS OF CONTRACTILITY
Cardiomyopathy is a genetically triggered or acquired disease Occurs in approximately 1.13 in 100,000 children HF (less commonly, dysrhythmia) is the presenting feature DCM Characterized by enlarged ventricular chambers and impaired systolic and diastolic function Usually idiopathic Infection (myocarditis viral-enterovirus) Operative injury Consequence of degenerative or metabolic diseases Muscular dystrophies Mitochondriopathy, Hyperthyroidism carnitine deficiency
 is the presenting feature. DCM. Characterized by enlarged ventricular chambers and impaired systolic and diastolic function. Usually idiopathic. Infection (myocarditis viral-enterovirus) Operative injury. Consequence of degenerative or metabolic diseases. Muscular dystrophies. Mitochondriopathy, Hyperthyroidism. carnitine deficiency.")
60
Restrictive cardiomyopathy
Idiopathic Infiltrative or storage diseases hemochromatosis Pompe disease Hypertrophic cardiomyopathy Idiopathic hypertrophic subaortic stenosis, rarely associated with pediatric HF.

61
ARRHYTHMIAS Arrhythmias cause HF when the heart rate is too fast or too slow to meet tissue metabolic demands

62
TACHYCARDIA Diastolic filling time shortens to and cardiac output is decreased. Most common childhood tachyarrhythmia is SVT Often presents in the first few months of life Rarely cause heart failure Occasionally PJRT ,ectopic atrial tachycardia and VT

63
CHRONIC BRADYCARDIAS LV enlarges to accommodate larger stroke volumes
Chamber dilation reaches a limit that cannot be compensated without increase in heart rate Febrile states are particularly stressful Congenital CHB may be well-tolerated in utero Dysfunction cause hydrops and intrauterine demise After birth, progression to HF depends on the ventricular rate and the speed of diagnosis and intervention Children with congenital CHB who are pacemaker dependent are at risk of subsequent pacemaker-mediated cardiomyopathy

64
CARDIAC ISCHEMIA Relatively rare in children ALCAPA
Palliative surgery that requires reconstruction of or near the coronary arteries e.g. Ross procedure, arterial switch operation

65
HIGH OUTPUT HF +EXCESSIVE PRELOAD
Septic shock causes Volume load on both sides of the heart Increased SV associated with hyperdynamic systolic function Elaboration of vasoactive molecules such as endotoxin and cytokines such as TNF-alpha leads to decreased SVR Cardiac output is increased Precapillary shunting Decreased tissue perfusion and lactic acid production Increased vascular permeability -increased total body fluid volume Toxin or direct microbial actions -negative inotropic effects Stresses produce demands for cardiac output and MVO2

66
LABORATORY STUDIES PULSE OXIMETRY ECG ABG

67
CXR Size of the heart is difficult to determine radiologically, particularly if there is a superimposed thymic shadow. Enlarged cardiac shadow unassociated with signs of CHF- suspect that shadow noncardiac Absence of cardiomegaly in a good inspiratory film (with diaphragm near the 10th rib posteriorly) practically excludes CHF except due to a cause like obstructed total anomalous pulmonary venous connection (TAPVC)
 practically excludes CHF except due to a cause like obstructed total anomalous pulmonary venous connection (TAPVC)")
68
CT Ratio method, > 60% Massive cardiomegaly RA dilation Pulm plethora LV Dialatation

69
ECHOCARDIOGRAPHY Not useful for the evaluation of HF, which is a clinical diagnosis Essential for identifying Causes of HF such as structural heart disease Ventricular dysfunction (both systolic and diastolic) Chamber dimensions Effusions (both pericardial and pleural)
 Chamber dimensions. Effusions (both pericardial and pleural)")
70
Assessment of right and single ventricular function is more complicated because of altered geometry
RV tissue Doppler imaging correlates with measurements of RVEDP obtained during cardiac catheterization Doppler myocardial performance index has been used to assess function in children with SVs and abnormal RVs Single (left) ventricle physiology-remodeling to a spherical shape associated with deterioration
 ventricle physiology-remodeling to a spherical shape associated with deterioration.")
71
CMR- Geometric assessment of RV and SV function
3D echo -additional detail of intracardiac anatomy

72
Worse EF and FS at presentation -poor outcome in children with DCM
LV remodeling to a more spherical shape -predict a poorer prognosis in children with DCM Myocarditis- children can present with severely depressed ventricular function but recover normal function within a few weeks to months Lack of improvement in EF % over time –correlate worse outcome.

73
HF BIOMARKERS Released primarily in response to atrial stretching
Sensitive marker of cardiac filling pressure and diastolic dysfunction BNP levels can distinguish between cardiac and pulmonary causes of respiratory distress in neonates and children

74
In acute decompensated heart failure due to cardiomyopathy a BNP level 300 pg/Ml strongly correlate with poor outcome than symptoms or echocardiographic findings BNP levels can be different in children with DCM and congenital heart disease despite similar NYHA class, EF, and MVO2

75
PRINCIPLES OF MANAGING HEART FAILURE
Recognition and treatment of underlying systemic disease Timely Surgical Repair of Structural Anomalies Afterload Reduction ACE inhibitors ARB Milrinone Type 4 phosphodiesterase inhibitors Nitrates Recombinant BNP

76
Preload Reduction Diuretics BNP Sympathetic Inhibition Beta blockers Recombinant BNP Digoxin Cardiac Remodeling Prevention Mineralocorticoid inhibitors Inotropy

77
MEDICAL THERAPY Medical management aims to maximize cardiac output and tissue perfusion while minimizing stresses that increase MVO2 Goals are accomplished by reducing afterload stress and preload Treatments that “rest” the heart such as vasodilators are preferred to inotropic agents that increase MVO2

78
Few drugs have evidence based efficacy compared to adults
Pediatric dosing is necessary Scaling adult doses for pediatric use solely based on weight can result in either inadequate or excessive drug levels

79
GENERAL MEASURES Bed rest and limit activities
Nurse propped up or in sitting position Control fever Expressed breast milk for small infants Fluid restriction in volume overloaded Optimal sedation Correction of anemia ,acidosis, hypoglycemia and hypocalcaemia if present Oxygen –caution in LT-RT shunt as pulmonary vasodilation my increase shunt CPAP or mechanical ventilation as necessary

81
CONGENITAL HEART DISEASE: VOLUME OVERLOAD
General therapeutic approach is to minimize symptoms and optimize growth until a definitive procedure can be performed. Mainstays of medical therapy are digitalis and diuretics.

82
DIGITALIS Digitalis considered as essential component
Evidence for efficacy is less in volume-overload lesions with normal function where the mild inotropic effect of digitalis is unnecessary Sympatholytic properties may modulate pathological neurohormonal activation

83
LOOP DIURETICS Furosemide improved clinical symptoms on a background of digitalis administration Decrease pulmonary congestion and thus decrease the work of breathing It is one of the least toxic diuretics in pediatrics Associated with sensorineural hearing loss after long-term administration in neonatal respiratory distress Deafness related to speed of infusion Torasemide is also safe and effective in this group

84
26. Faris R FM, Purcell H, Poole‐Wilson PS, Coats AJS
26. Faris R FM, Purcell H, Poole‐Wilson PS, Coats AJS. Diuretics for heart failure. Cochrane Database of Systematic Reviews 27. Ward OC, Lam LK. Bumetanide in heart failure in infancy. Arch Dis Child Nov;52(11):877‐82. 28. Muller K, Gamba G, Jaquet F, Hess B. Torasemide vs. furosemide in primary care patients with chronic heart failure NYHA II to IV‐‐efficacy and quality of life. Eur J Heart Fail Dec;5(6):793‐801. 29. Senzaki H, Kamiyama MP, Masutani S, Ishido H, Taketazu M, Kobayashi T, et al. Efficacy and safety of Torasemide in children with heart failure. Arch Dis Child Mar 12. 30. Lowrie L. Diuretic therapy of heart failure in infants and children. Prog Pediatr Cardiol Nov 4;12(1):45‐55. 31. Arnold WC. Efficacy of metolazone and furosemide in children with furosemide‐resistant edema. Pediatrics Nov;74(5):872‐5. 32. Rosenberg J, Gustafsson F, Galatius S, Hildebrandt PR. Combination therapy with metolazone and loop diuretics in outpatients with refractory heart failure: an observational study and review of the literature. Cardiovasc Drugs Ther Aug;19(4):301‐6.
:877‐ Muller K, Gamba G, Jaquet F, Hess B. Torasemide vs. furosemide in primary care patients with chronic heart failure NYHA II to IV‐‐efficacy and quality of life. Eur J Heart Fail Dec;5(6):793‐ Senzaki H, Kamiyama MP, Masutani S, Ishido H, Taketazu M, Kobayashi T, et al. Efficacy and safety of Torasemide in children with heart failure. Arch Dis Child Mar Lowrie L. Diuretic therapy of heart failure in infants and children. Prog Pediatr Cardiol Nov 4;12(1):45‐ Arnold WC. Efficacy of metolazone and furosemide in children with furosemide‐resistant edema. Pediatrics Nov;74(5):872‐ Rosenberg J, Gustafsson F, Galatius S, Hildebrandt PR. Combination therapy with metolazone and loop diuretics in outpatients with refractory heart failure: an observational study and review of the literature. Cardiovasc Drugs Ther Aug;19(4):301‐6.")
85
ACE INHIBITION Improved growth was seen in some children with CHF
Captopril and enalapril Concerning incidence of renal failure particularly in premature and very young infants. No efficacy data on ARBs in children with heart failure

87
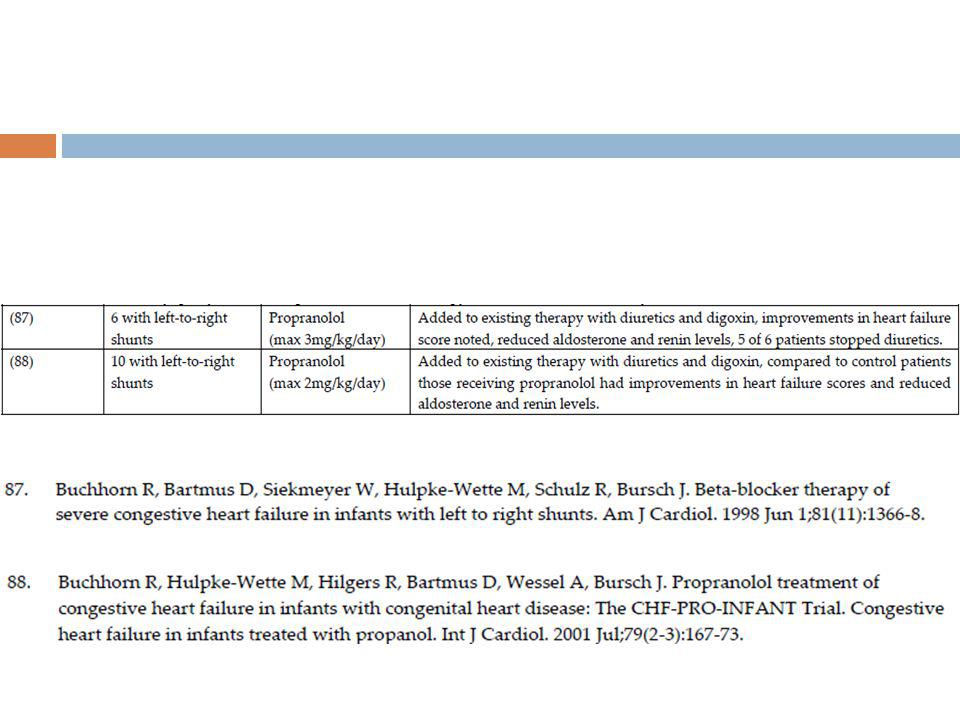
B BLOCKER Propranolol to the combination of digoxin and diuretics shown to improve HF symptoms and improve growth

89
SPIRONOLACTONE Literature supporting the role in paediatric HF is limited 61. Hobbins SM, Fowler RS, Rowe RD, Korey AG. Spironolactone therapy in infants with congestive heart failure secondary to congenital heart disease. Arch Dis Child Dec;56(12):934‐8. 62. Buck ML. Clinical experience with spironolactone in pediatrics. Ann Pharmacother May;39(5):823‐8.
:934‐ Buck ML. Clinical experience with spironolactone in pediatrics. Ann Pharmacother May;39(5):823‐8.")
90
NESIRITIDE Recombinant form of BNP
Promotes both diuresis and vasodilation Drug reduces both preload and afterload Directly inhibits the sympathetic nervous system, mineralocorticoid expression, and cardiac fibroblast activation and promotes myocyte survival. Studies in the pediatric age group are lacking

91
INTRACARDIAC REPAIR Early transcatheter or surgical intervention, often before age 6 months is possible Minimizes time of significant symptoms or medication Minimizes the risk of pulmonary vascular disease. Contemporary data indicate that early repair of a VSD, even in the first month of life and at weights 4 kg, does not confer increased risk compared with older, larger infants.

92
TRANSCATHETER DEVICE CLOSURE
Transcatheter device closure of muscular VSD Weight atleast 5.2 kg.

93
CONGENITAL HEART DISEASE PRESSURE OVERLOAD
Ventricular response to pressure overload is determined by the severity and duration of the load Critical AS can cause acute LV failure in early infancy “Critical "implies a requirement for maintaining PDA with prostaglandin infusion

94
Optimizing hemodynamics until urgent intervention
Balloon valvuloplasty, first described in neonates in replaced surgical valvotomy, as the first-line intervention in uncomplicated AS, including critical AS. Ventricular function improves and usually normalizes after catheter based or surgical intervention.

95
Higher AV gradient -associated with lower FS, decreased exercise capacity, increased risk of SCD and serious arrhythmias Severe AS (Doppler MG 50 mm Hg(40)) - intervention to prevent or ameliorate symptoms Mild AS (Doppler MG 25 mm Hg) could be followed up These criteria continue to guide contemporary management along with other criteria such as symptoms, exercise capacity, ventricular hypertrophy, wall stress, and evidence of arrhythmia.
) - intervention to prevent or ameliorate symptoms. Mild AS (Doppler MG 25 mm Hg) could be followed up. These criteria continue to guide contemporary management along with other criteria such as symptoms, exercise capacity, ventricular hypertrophy, wall stress, and evidence of arrhythmia.")
96
COMPLEX CONDITIONS RV failure in children
There is no systematic clinical evidence for anticongestive therapy Furosemide- relieve the clinical symptoms RV dysfunction - betablocker therapy did not improve ventricular function Suggest a different pathophysiological process in RV failure and thus a requirement for novel treatment strategies

97
RV functioning as systemic ventricle
If symptomatic ventricular dysfunction occurs ISHLT Guidelines recommend diuretics, digitalis, and ACE inhibition, based solely on expert consensus

98
Fontan procedure Systemic and pulmonary circulations are separated and SV is pumping to the systemic circulation A large cross-sectional study of 546 Fontan survivors aged 6 to 18 years found normal ejection fraction in 73% of subjects but abnormal diastolic function in 72%. Diastolic function was significantly worse in the group with RV compared with LV or mixed ventricular morphology. Overt heart failure after the Fontan operation is relatively infrequent in the pediatric population but increases in the adult Identifying and treating underlying causes of HF such as conduction or rhythm abnormalities or residual structural lesions is initial strategy.

99
Single ventricle No compelling data to guide medical treatment ISHLT guidelines recommend diuretics, digitalis, and ACE inhibition but not beta blockade, based on expert consensus.

100
CARDIOMYOPATHIES Primary or acquired DCM
ISHLT Guidelines reflect only data from studies in adults in recommending both digitalis and diuretics only for symptomatic LV dysfunction in children Torasemide, a newer loop diuretic with potassium-sparing properties, significantly improved New York University Pediatric Heart Failure Index, decreased BNP levels, and improved fractional shortening Senzaki etal Efficacy and safety of Torasemide in children with heart failure. Arch Dis Child Mar 12

101
ISHLT Guidelines recommend ACE inhibition for moderate or severe degrees of LV dysfunction regardless of symptoms ARB therapy if ACE inhibitor is indicated but not tolerated

103
Although the carvedilol trial did not demonstrate efficacy based on the primary end point improvement in FS and clinical outcome seen in DCM patients who received carvedilol has led to the empirical use of carvedilol in this group of patients. long-term responses to BB therapy have not been studied in children Close monitoring of potential adverse effects is essential

106
Systemic exposure to carvedilol amongst paediatric heart failure patients and has indicated that higher doses relative to body weight are required to provide exposure comparable to adults Paediatric carvedilol doses 1mg/kg/day for adolescents 2mg/kg/day for children aged to 11 years 3mg/kg/day for infants (aged 28 days to 23 months) Carvedilol used in many of the studies have been lower than these recommendations
 Carvedilol used in many of the studies have been lower than these recommendations.")
107
Treatment of primary diastolic heart failure in children with hypertrophic or restrictive cardiomyopathy are limited to the judicious use of diuretics to decrease the degree of pulmonary congestion.

108
Inotropes in acute cardiac failure
Routine use of in children cannot be recommended Used in treatment of exacerbating conditions and as a bridging therapy pending transplantation Dopamine as it possesses both the cardiac and renal effects is more useful

109
Practice guidelines for pediatric heart failure, developed by the International Society for Heart and Lung Transplantation (ISHLT) None of the 49 recommendations is level A evidence 7 are level B evidence Remainder are level C (expert consensus).
.")
111
NUTRITION AND EXERCISE IN PEDIATRIC HEART FAILURE
Important as medical therapy, particularly in infants Increase the caloric density of feeds as soon as a diagnosis Sodium restriction is not recommended in infants and young children. Sodium restriction can result in impaired body and brain growth

112
There is evidence that regular physical activity can result in sustained improvements in physical functioning even in children with complex congenital heart disease. Significant, sustained improvements in exercise function, behavior, self-esteem and emotional state.

113
SURGICAL AND DEVICE THERAPY

114
Pacemaker and implantable defibrillator therapy
Biventricular pacing Ventricular assist devices Heart transplantation

115
THANK U

Similar presentations

















 Class IV: symptoms at rest Class III: symptoms on less-than-ordinary exertion Class.>")





 F.R.C.P.(E) F.R.C.P.(LONDON) F.A.C.C. DESIGNED AT A.V. DEPTT F.J.M.C. BY RABIA KAZMI.>")



 is the clinical state of systemic and pulmonary congestion resulting from inability of the heart to pump.>")