Download presentation
Presentation is loading. Please wait.

1
Bijoy Telivala, MD 904-438-4545 Bijoy.Telivala@csnf.us
Advances in Immunotherapy Bijoy Telivala, MD

2
Introduction One of the first reported events was when Dr Coley in the late 19th century reported insertion of dead bacteria cells lead to shrinkage of sarcoma cell Since then immunotherapy has been the “ holy grail “ in the fight against cancer Over the last few years there has been a greater understanding of how to harness the immune system to combat cancer Disclosures: none

3
Tumor Immunology CD4 and CD8 T cells usually initiate distinction between self and non self antigens Natural Killer cells do not require antigen presentation by MHC for cytotoxic activity Macrophages play an important role in phagocytosis

4
Tumor synapse

5
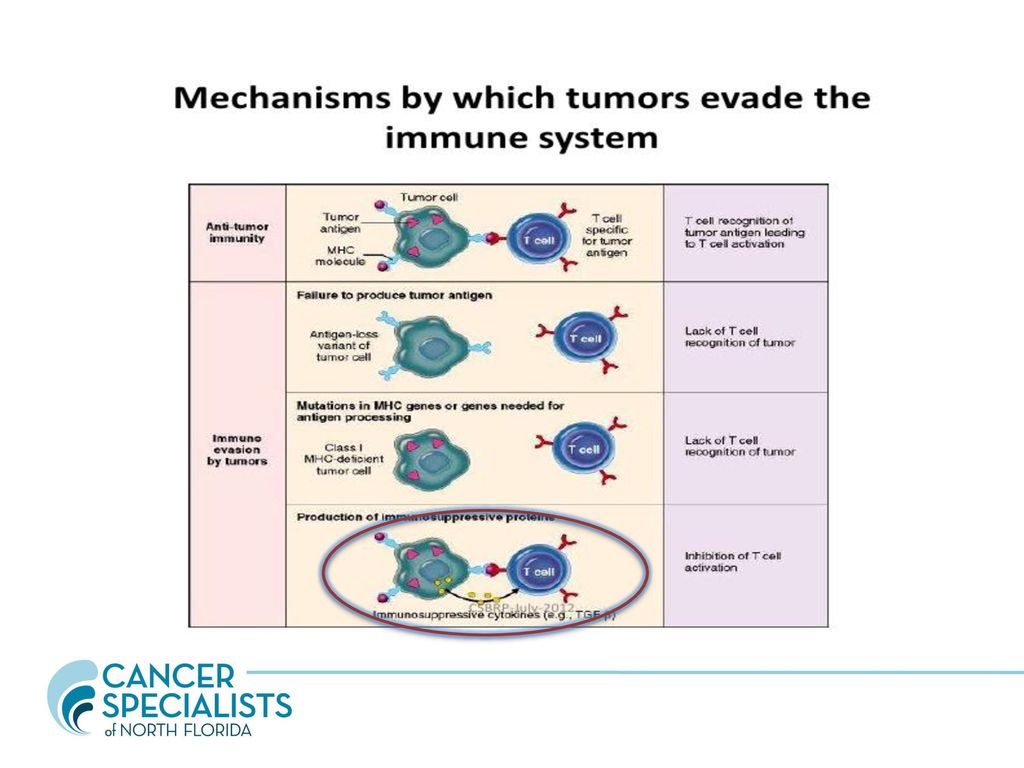
Tumor Evasion of Immune Surveillance
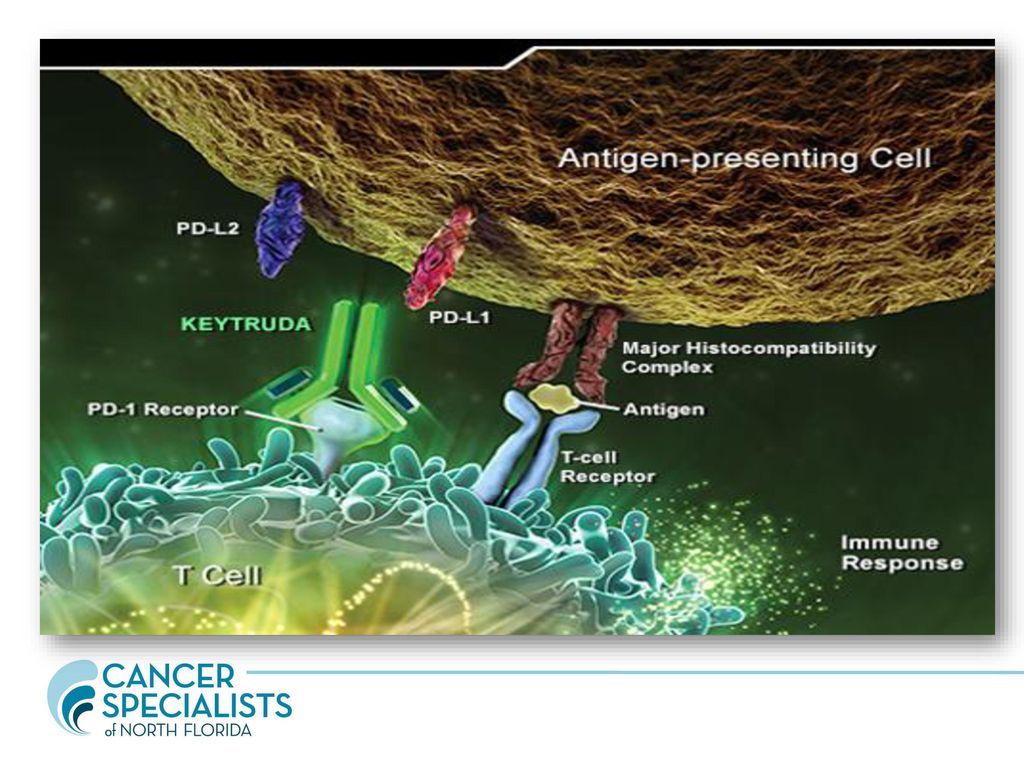
Loss of MHC 1 expression by tumor Tumor can promote immune tolerant micro environment which leads to production of cytokines which can suppress production of CD 4 and CD 8 T cells Tumors can upregulate the expression immune check point inhibitors like PD-1 or PDL1 which can promote peripheral T cell exhaustion

8
Classes of Drugs PD-1 Inhibitors Opdivo Keytruda Avelumab
PDL-1 Inhibitors Tecentriq CTLA 4 Antibodies Yervoy Chimeric Antigen Receptors ( CAR-T ) are genetically modified T cells using the patients own T cells.
 are genetically modified T cells using the patients own T cells.")
9
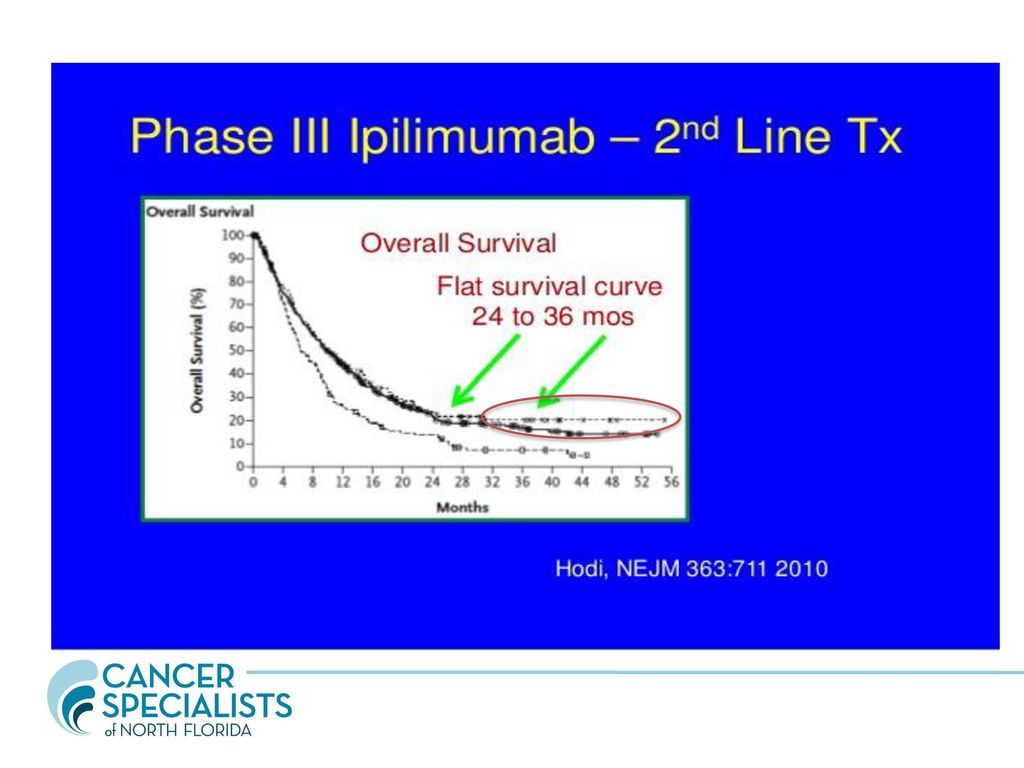
Yervoy First developed immunotherapy
Currently approved as a single agent or in combination with Opdivo to treat advanced/ metastatic melanoma Also approved as adjuvant treatment for high risk/Stage 3 melanoma especially those with Lymph node involvement Works by blocking CTLA-4 ( Cytotoxic T lymphocyte Antigen 4 )
")
10
Yervoy

11
Yervoy- Toxicity Not a benign drug
Significant diarrhea, pneumonitis and skin toxicities Can also cause auto immune hepatitis and nephritis Can see delayed toxicities

12
Yervoy- Summary Hardly used as a single agent except for adjuvant melanoma In metastatic melanoma it has been essentially replaced by PD1/PDL1 inhibitors Biggest advantage is that a small number ( % ) of patients are thought to be cured or in a very deep remission Cost is around $ 100,000 for entire treatment
 of patients are thought to be cured or in a very deep remission. Cost is around $ 100,000 for entire treatment.")
14
PD1/PDL1 Inhibitors Biggest excitement in oncology in the last decade
Has made dramatic improvements in survival and patient quality of life They will form back bone of majority of treatment regimens in the future

15
Opdivo- FDA Indications
Metastatic melanoma as a single agent or in combination with Yervoy Metastatic Non small cell lung cancer Relapsed Hodgkins Lymphoma Relapsed Head & neck cancer Relapsed/Metastatic Bladder cancer Metastatic Kidney cancer

16
Keytruda- FDA Indications
Metastatic melanoma Metastatic head & neck cancer Metastatic Non small cell lung cancer. First Immunotherapy to be approved in combination with chemotherapy in front line metastatic lung cancer Hodgkins Lymphoma

17
Tecentriq- FDA Indications
Metastatic Bladder Cancer Metastatic Non small cell lung cancer

18
Avelumab- FDA Indications
New kid on the block Only drug to be approved for Merkel cell carcinoma Metastatic bladder cancer

19
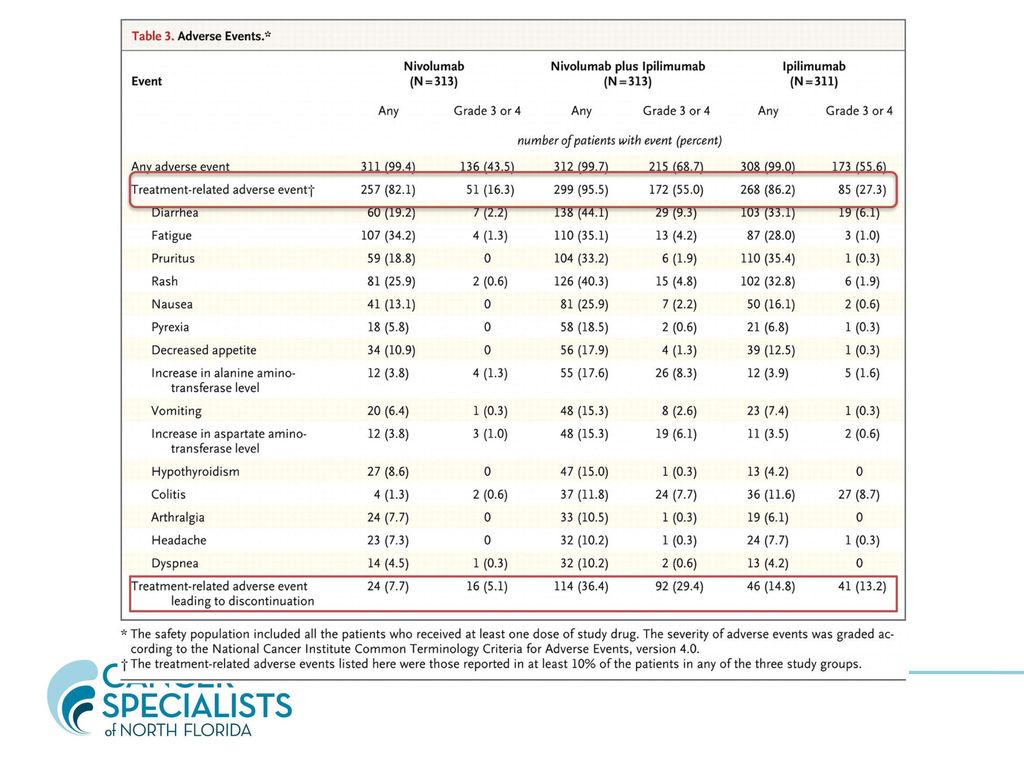
Opdivo Plus Yervoy Approved in combination for metastatic melanoma
Clinical trial ( Checkmate -067) compared Yervoy vs Opdivo vs the combination Overall survival at 2 years was higher ( 64 % for combination vs 45 % for Yervoy) However toxicities especially GI were much higher Probably a good combination but only for the right patient Combination is being evaluated in lung ca/kidney ca
 compared Yervoy vs Opdivo vs the combination. Overall survival at 2 years was higher ( 64 % for combination vs 45 % for Yervoy) However toxicities especially GI were much higher. Probably a good combination but only for the right patient. Combination is being evaluated in lung ca/kidney ca.")
20
Opdivo Plus yervoy

23
Side Effects of PD1 Inhibitors
Pneumonitis Diarrhea Skin toxicities Endocrine abnormalities including hypothyroidism and hypo pitutarism Rarely it can cause renal and liver failure

24
CAR- T Therapy In clinical development
Not routinely available except in few select centers Involves engineering patients own immune cells to recognize and attack the tumors Uses adoptive cell transfer

25
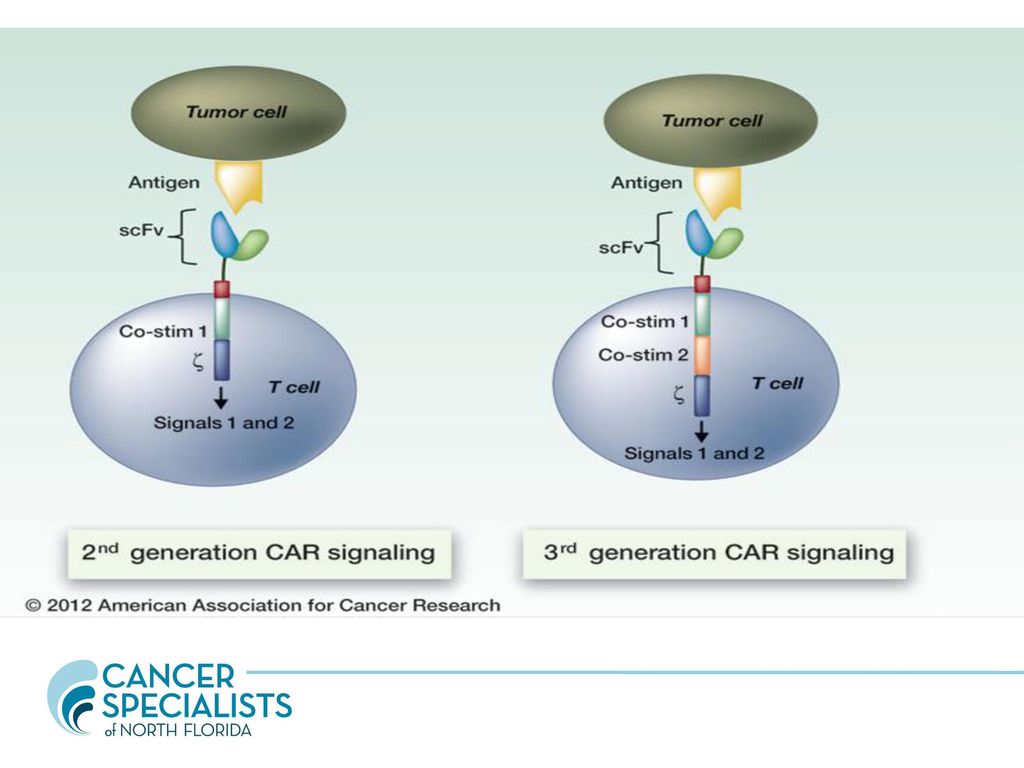
Car- T Therapy Adoptive cell transfer is like giving patients a living drug After collection from body T cells are genetically modified to produce specific receptors called chimeric antigen receptors (CAR) More than a billion CAR T cells are grown in the lab T cells are then infused into the body and then if if all goes as planned, the T cells multiply in the patient’s body and, with guidance from their engineered receptor, recognize and kill cancer cells that harbor the antigen on their surfaces In clinical trials for ALL and some Lymphoma patients
 More than a billion CAR T cells are grown in the lab. T cells are then infused into the body and then if if all goes as planned, the T cells multiply in the patient’s body and, with guidance from their engineered receptor, recognize and kill cancer cells that harbor the antigen on their surfaces. In clinical trials for ALL and some Lymphoma patients.")
27
CAR- T Therapy Side Effects
Cytokine storm Fever Nausea Skin reaction Hypotension Needs close monitoring and early recognition

28
Take Home Points for PCP
Immunotherapy is the 4th pillar in treating cancer patients More patients are going to be on immunotherapy in the future Side effects are unique and very different from traditional chemotherapy Steroids help with side effects but should be used judiciously

29
Take Home Points for PCP
We are only scratching the surface of immunotherapy Different cancers respond differently to immunotherapy Melanoma have the best responses while others like prostate cancer have minimal responses Enrollment in clinical trials is very important

30
Clinical Trials at CSNF
We have over 8 open immunotherapy clinical trials and have participated in many more Disease sites : Breast cancer Multiple Myeloma Non small cell Lung cancer Kidney cancer Bladder cancer Small cell Lung Cancer

31
Questions ???

Similar presentations
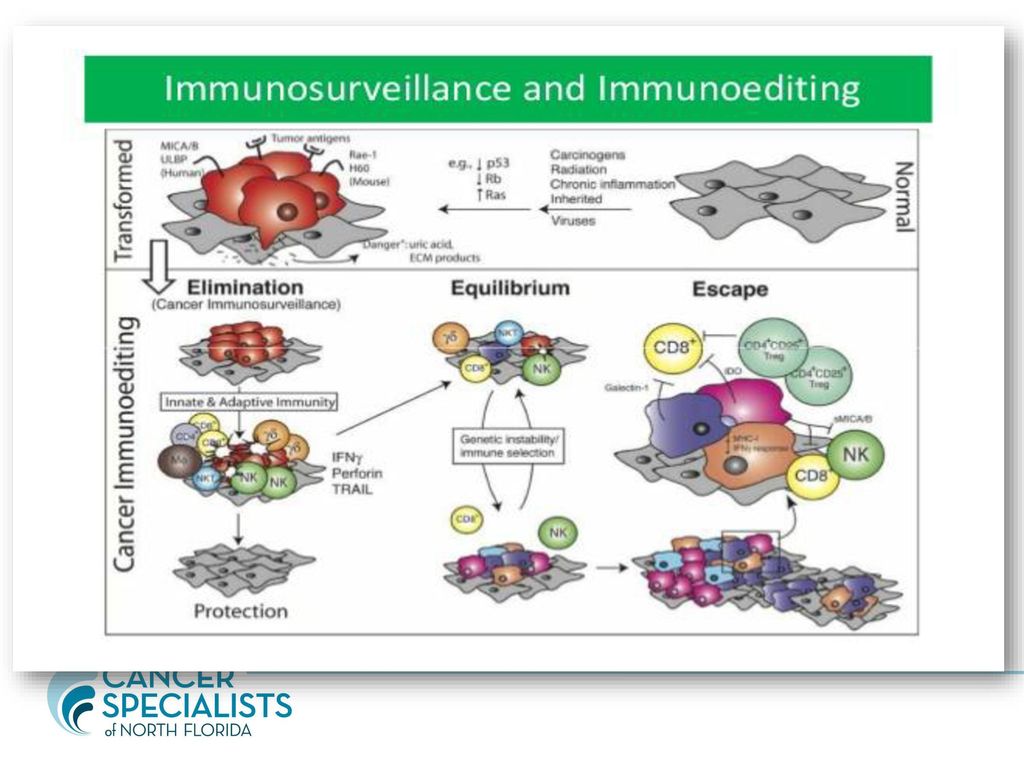



: Cancer Immunosurveillance & Immunoediting Masoud H. Manjili Department of Microbiology & Immunology Goodwin Research Building-286.>")















