Download presentation
Presentation is loading. Please wait.

1
Health Equity Nashville Public Health Learning Collaborative July 31, 2013

2
Disclosures The following educational planners, speakers, moderators and/or panelists of this CME activity have no relevant financial relationships with commercial interests to disclose: Mohamed Kanu, Ph.D. Leah Alexander, Ph.D. William Cooper, M.D.

3
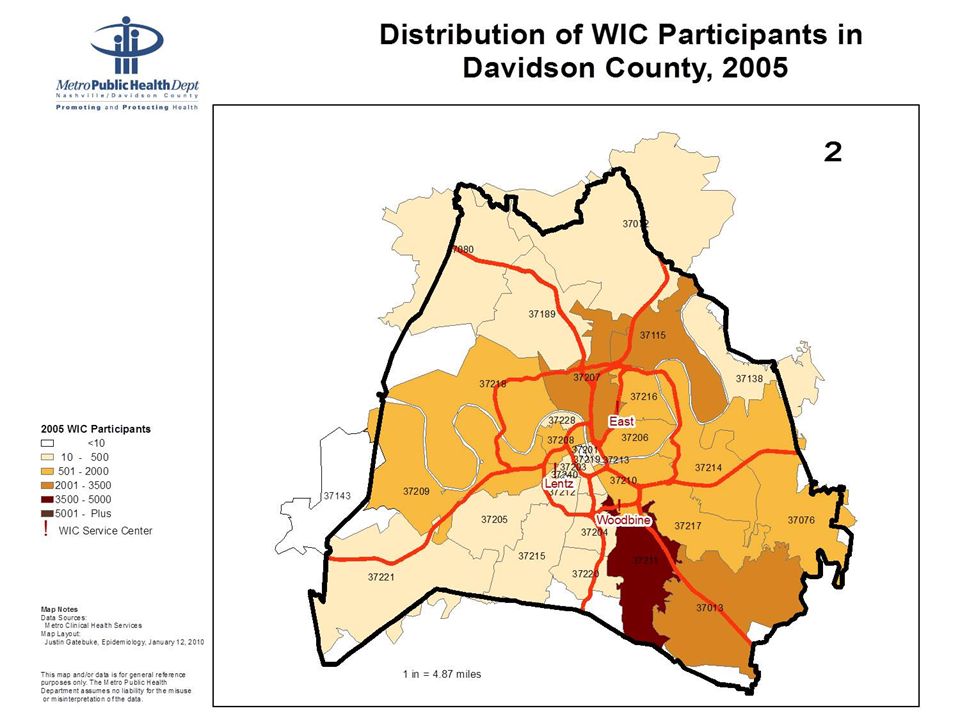
Food Insecurity and Nutritional Risk in South Nashville A Case Study in Health Equity

4
Changing Population 1995-2010 –Increase in WIC participants in S. Nashville –Shift in demographics Fewer African-American participants Greater number of Latino participants –Challenges in providing services to families most in need

10
Challenge: Services and Need Transportation –Distance to available services –Public transportation limited Culture and language Federal WIC program regulations –Site facilities –Services Community resistance to expanding services for persons living in poverty

11
Health Equity What are the issues of health equity illustrated by this case? What are some possible solutions? What are the challenges?

12
Objectives Upon completion, participants will be able to: Define health equity. Explain the relationship between health equity, health disparities and the determinants of health. Identify historical, social, political factors impacting health equity. Discuss strategies for achieving health equity.

13
What do you know about Health Equity? Let’s take a quiz………

14
A.3 times B.4 times C.5 times D.7 times Children living in poverty are how many times more likely to have poor health, compared with children living in high-income households?

15
ANSWER: D. 7 Times Children are most vulnerable. Not only are they susceptible to sub- standard housing, poor food, bad schools, unsafe streets and chronic stress, but the impacts of childhood poverty are cumulative, leading to a pile-up of risk that influences adult health and can even affect the next generation.

16
A.Japanese B.Bangladeshis C.Cubans D.Algerians living in Paris E.All of the above African American males in Harlem have a shorter life expectancy from age five than which of the following groups?

17
ANSWER: E. All of the above The biggest killers of African American males in many poor, segregated urban neighborhoods are not violence nor drugs nor AIDS, but heart disease, stroke and other chronic diseases that cut men down in middle age.

18
A.About the same B.2 times as many C.4 times as many D.6 times as many On average, how many more supermarkets are there in predominantly white neighborhoods compared to predominantly Black and Latino neighborhoods?

19
ANSWER: C. 4 times Predominantly Black and Latino neighborhoods have more fast-food franchises and liquor stores, yet often lack stores that offer fresh, affordable fruits and vegetables.

20
A.Whether or not you smoke B.What you eat C.Whether or not you are wealthy D.Whether or not you have health insurance E.How often you exercise On average, which of the following conditions is the strongest predictor of your health?

21
ANSWER: C. Whether or not you are wealthy The wealthier you are, on average, the better your health, from the bottom all the way to the top. Genes, diet, exercise and other behaviors are important. But a poor smoker still stands a greater chance of getting ill than a rich smoker.

22
How did you do?

24
Health Disparities “A difference in rates of illness, disease, or conditions among different populations.” – UW, Robert Wood Johnson & NACCHO

25
Health Equity “Achieving the highest level of health for all people. It entails focused societal efforts to address avoidable inequalities by equalizing the conditions for health for all groups, especially for those who have experienced socioeconomic disadvantage or historical injustices.” Healthy People 2020

26
Health Equity “Achieved when every person has the opportunity to achieve his or her full health potential. No one is disadvantaged from achieving this potential because of social position or other socially determined circumstances.” Centers for Disease Control & Prevention/World Health Organization

27
Health Inequities “Differences in health which are not only unnecessary and avoidable but, in addition, are considered unfair and unjust.” –Margaret Whitehead Department of Public Health University of Liverpool

28
Health Inequity Several definitions for the concept Essential elements across all definitions…. Health inequities are unjust, unnatural, and avoidable differences in health status, distribution of disease, and mortality rates across population groups The are beyond control of the individuals, meaning they are systemic problems. While individual choices influence health, these patterns across populations are not a result of an individuals’ choices alone They are sustained over time and generations.

29
Push to Achieve Health Equity Driven by values of social justice (the equitable distribution of resources) Focuses on outcomes (achieving equity) rather that problems (ending disparities) Focuses on structural and institutional changes to address the conditions that produce illness and disease -DRA Project 2009
 Focuses on outcomes (achieving equity) rather that problems (ending disparities) Focuses on structural and institutional changes to address the conditions that produce illness and disease -DRA Project 2009")
30
Principles of Health Equity Health equity is a cross-cutting broad issue associated with fundamental social values and well-being Health equity is connected to all aspects of public health work and the most basic influences on the health of populations Working to achieve health equity requires multidisciplinary approaches and a more holistic, comprehensive view of health and coordinated strategies (Troutman, 2009)
")
31
What does Health Inequity look like in our community? Think of some other examples….

32
Local Health Inequities: Consider Census Tracts…. Address is the most powerful predictor of health status In Davidson County Prevalence of chronic disease varies by census tract Some tracts where the average person in “normal” weight compared to others where the average person is overweight or obese Some tracts have less that 15% of residents with hypertension compared to others with 49% Premature mortality varies by neighborhood Most health problems in areas with high poverty rates High Poverty = community assets

33
Redlining practices by banks and home insurance agents Displacement caused by highway construction and other urban renewal projects Middle class and white flight to the suburbs Discriminatory mortgage underwriting by the FHA/VA Disinvestment and concentrated poverty in urban centers Local Health Inequities: Historical Issues impacting our community Tax policies and subsidies that benefit the wealthy Industrial and toxic waste facilities in high poverty neighborhoods Unstable and changing labor markets

35
Health Disparities vs. Health Inequities Health Disparities –Variations or differences in health status among groups of people. Can refer to any difference in health with no implication that the differences are unjust. Health Inequalities –Differences in population health status and mortality rates that are unjust, systemic, patterned, unfair

36
What links the two concepts? Social Determinants of Health –Income & income inequality –Education –Race/ethnicity/gender & related discrimination –Built Environment –Stress –Social support –Early child experiences –Employment –Housing –Transportation –Food Environment –Social standing

38
Brennan Ramirez LK, Baker EA, Metzler M. Promoting Health Equity: A Resource to Help Communities Address Social Determinants of Health. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2008. Achieving Health Equity…What we can do? “Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and health care disparities.” – Healthy People 2020 H EALTH E QUITY

39
1.Health is more than health care. 2.Health is tied to the distribution of resources. 3.Racism imposes an added burden. 4.The choices we make are shaped by the choices we have. 5.High demand + low control = chronic stress. 6.Chronic stress can be deadly. 7.Inequality – economic and political – is bad for our health. 8.Social policy is health policy. 9.Health inequities are not natural. 10.We all pay the price for poor health. –Unnatural Causes 10 Things to Remember about Health

40
Of all the forms of inequality, injustice in health care is the most shocking and inhumane. Martin Luther King Jr.

Similar presentations















 Networking Forum May 15,>")






 April 12, 2015.>")



