Download presentation
Presentation is loading. Please wait.

1
OTOSCLEROSIS SDL 22 3/14/2014

2
Learning Objectives Upon completion of this module the student will: 1. Define and describe otosclerosis. 2. Discuss epidemiology of otosclerosis. 3. Discuss the roles of hereditary factors and the measles infection in the causation of otosclerosis. 4. Describe by which molecular mechanisms the otic capsule avoids bone remodeling under normal conditions. 5. Describe the molecular mechanisms that trigger the otic capsule bone remodeling in otosclerosis. 6. Describe clinical symptoms and interpret the audiometry findings in otosclerosis. 7. Describe the significance of the Schwartze sign 8. Describe the histopathological phases of otospongiosis and otosclerosis

3
Otosclerosis Otosclerosis is a genetically mediated metabolic bone disorder of the temporal bone. ossification of the annular ligament and the surrounding bone (i.e. otic capsule, the bone that surrounds the inner ear) footplate of stapes becomes ankylosed in the oval window niche A conductive hearing loss is the clinical result.
 footplate of stapes becomes ankylosed in the oval window niche A conductive hearing loss is the clinical result..")
4
Otosclerosis Epidemiology Estimated to occur histologically in 10% of Caucasians and produces clinical hearing loss in 1%. Single most common cause of hearing impairment in Caucasians. The female to male ratio of clinical OS is 2:1. The onset of disease is mainly between 15 and 40 years of age. The disease is bilateral in most (70–80%) cases
 cases.")
5
Etiology Not well understood; potentially genetic or viral. Genetic: Most studies on families with OS support a pattern of autosomal dominant transmission with incomplete penetrance. Genetic linkage shows the presence of two otosclerosis loci, OTSC1 and OTSC2, respectively, but the responsible genes are unknown. Viral: measles proteins and RNA are found in active OS otosclerosis OS incidence has fallen after introduction of the measles vaccine

6
Pathogenesis Otosclerosis is a process of bone remodeling affecting the otic capsule, which typically does not occur here. For bone remodeling to occur, RANK, RANK-L, and OPG are required. RANK binds to RANK-L causing Osteoclasts to form. OPG blocks this from happening by binding to RANK-L. Osteoprotegerin (OPG) is produced in extremely high concentration within the inner ear by stromal cells of the spiral ligament, and secreted into the perilymph. This inner ear OPG may contribute to inhibition of otic capsule remodeling by diffusing into the surrounding otic capsule bone. Over expression of OPG minimizes bone resorption, causing excessive bone formation, or osteopetrosis.
 is produced in extremely high concentration within the inner ear by stromal cells of the spiral ligament, and secreted into the perilymph. This inner ear OPG may contribute to inhibition of otic capsule remodeling by diffusing into the surrounding otic capsule bone. Over expression of OPG minimizes bone resorption, causing excessive bone formation, or osteopetrosis..")
7
Pathology The characteristic lesion in otosclerosis is a replacement of normal bone with dense sclerotic bone. 2 Phases: 1) Otospongiotic Phase: characterized by bone resorption around existing vessels Resultant hypervascularization, or a red blush seen on the medial wall of the middle ear behind the tympanic membrane, is the Schwartze sign. The result is a disorganized spongiotic bone, increased population of osteocytes, and enlarged marrow spaces containing vessels and other connective tissue.
 Otospongiotic Phase: characterized by bone resorption around existing vessels Resultant hypervascularization, or a red blush seen on the medial wall of the middle ear behind the tympanic membrane, is the Schwartze sign. The result is a disorganized spongiotic bone, increased population of osteocytes, and enlarged marrow spaces containing vessels and other connective tissue..")
8
Otosponiotic Phase

9
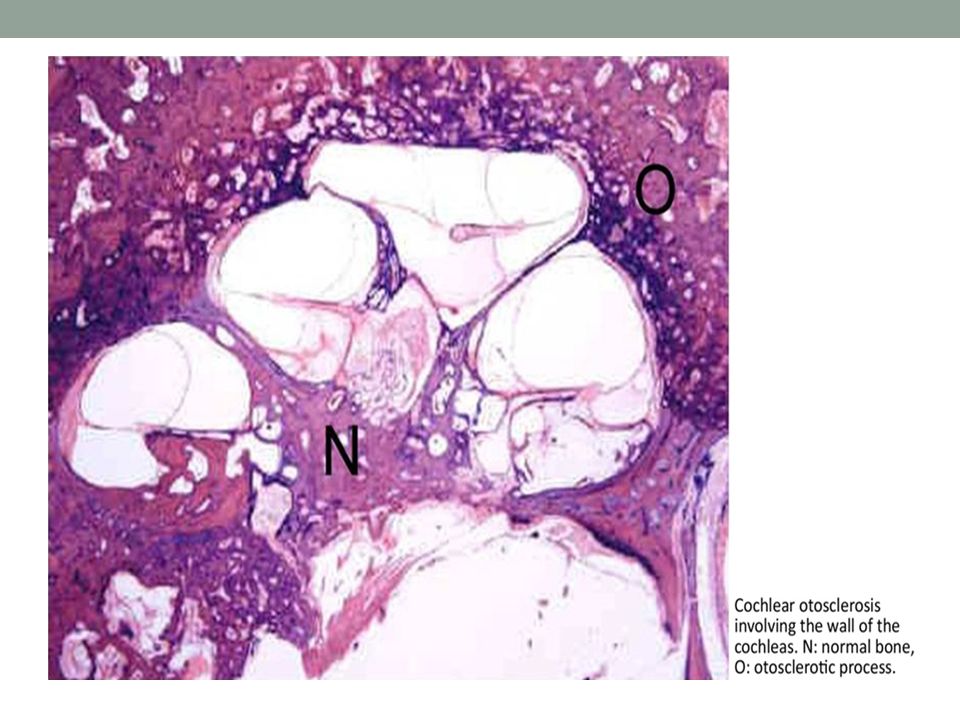
Pathology 2) Otosclerotic Phase: spaces of the resorbed bone are later replaced by dense sclerotic bone with few blood vessels, a few recognizable haversian systems and few cells Both stages of otosclerosis normally coexist in any single temporal bone
 Otosclerotic Phase: spaces of the resorbed bone are later replaced by dense sclerotic bone with few blood vessels, a few recognizable haversian systems and few cells Both stages of otosclerosis normally coexist in any single temporal bone")
10
Otosclerotic Phase

11
Lesion Location In 80-90% of patients, lesions are limited to the anterior oval window and affect its pathology by calcification of the annular ligament or by involving the stapes. Both processes result in characteristic conductive hearing loss. In 8% of patients, the process involves the cochlea and parts of the labyrinth (labyrinthine otosclerosis), resulting in sensorineural hearing loss. Approximately 2% of patients display both labyrinthine and ossicular chain involvement.
, resulting in sensorineural hearing loss. Approximately 2% of patients display both labyrinthine and ossicular chain involvement..")
13
Clinical Presentation Symptom onset usually occurs by the early third decade of life. Hearing loss and tinnitus (perception of an absent sound) are the principal symptoms of otosclerosis. Hearing loss is progressive, but rate is variable. Dizziness, which is varies in intensity from mild to severe rotary vertigo.
 are the principal symptoms of otosclerosis. Hearing loss is progressive, but rate is variable. Dizziness, which is varies in intensity from mild to severe rotary vertigo..")
14
Physical Examination Normal eardrums with a clear middle ear space 10% of patients demonstrate a Schwartze sign, characterized by a reddish-blue hue over the promontory and oval window niche areas, secondary to rich vascular supply associated with immature bone. Pure tone audiometry reveals signs of conductive hearing loss.

15
Pure Tone Audiometry Pure-tone audiometry is a test used to measure hearing sensitivity. This measure involves the peripheral and central auditory systems. Pure-tone thresholds (PTTs) indicate the softest sound audible to an individual at least 50% of the time. 3 Parts 1. Measurement of air-conduction thresholds. 2. Measurement of bone-conduction thresholds. 3. Audiogram interpretation.
 indicate the softest sound audible to an individual at least 50% of the time. 3 Parts 1. Measurement of air-conduction thresholds. 2. Measurement of bone-conduction thresholds. 3. Audiogram interpretation..")
16
Measurement of air-conduction thresholds The patient enters a special soundproof metal room and puts the headphones on. He is instructed to raise his hand when hears a tone. Tones are played at six different pitches, representing the range of human hearing. Each time the patient raises his hand, the volume is dropped 10 decibels (dB) until the patient can no longer hear it. The test is repeated in the other ear.
 until the patient can no longer hear it. The test is repeated in the other ear..")
17
Measurement of Bone-Conduction Thresholds The patient removes the headphones and puts on a headband with a small plastic rectangle that fits behind the ear and conducts sound directly to the bone. This type of testing bypasses the outer and middle ear. The tones are repeated.

18
Audiogram Interpretation Represents a person’s hearing loss Covers a range from 250 to 8000Hz (Normal speaking tone) Patient’s hearing is plotted against a normal curve on a graph, which is in decibels. Audiograms are set out with frequency (pitch) in hertz (Hz) on the horizontal axis, and decibels (loudness) on the vertical axis.
 in hertz (Hz) on the horizontal axis, and decibels (loudness) on the vertical axis..")
19
Conductive Hearing Loss If the patient has normal bone-conduction thresholds but poorer air-conduction thresholds (by at least 10 dB) he has conductive hearing loss. Sometimes hearing is better for the higher frequencies than it is for the lower ones. Conductive hearing loss happens when there is a problem conducting sound waves through the outer ear, tympanic membrane or middle ear ossicles.

20
Conductive Hearing Loss Chart

21
Sensorineural Loss If the patient shows both poor air-conduction and poor bone-conduction thresholds he has sensorineural loss. There is no "air-bone gap" that is characteristic of conductive hearing disturbances. The causes of sensorineural hearing loss lie in the inner ear, cranial nerve VIII or central processing centers of the brain. Many people with sensorineural losses experience a loss only in the high frequency region (4,000 to 8,000Hz). Experience difficulty in understanding speech in a noisy environment.
. Experience difficulty in understanding speech in a noisy environment..")
22
Mixed Hearing Loss Both air and bone conduction thresholds are depressed but bone conduction thresholds are better than air conduction thresholds. The difference between the two thresholds is referred to as the air-bone gap and represents the amount of the conductive component present.

23
Mixed Hearing Loss Audiogram

24
CT Scan May show bone changes consistent with otosclerosis in the area of the round or oval window and/or within other portions of the labyrinthine capsule and cochlea. Does not always detect a small area of otosclerosis, so a negative scan does not rule out this possibility.

Similar presentations















>")



