Download presentation
Presentation is loading. Please wait.

1
Sunrise teaching Elaine McKinley

2
7 year old with unilateral lower motor neurone facial paralysis
Problem: 7 year old with unilateral lower motor neurone facial paralysis

3
Facial Nerve Cranial Nerve VII Efferent and afferent fibres
Motor: Controls muscles of facial expression and innervates Stapedius muscle Sensory: conveys taste of the anterior two-thirds of the tongue Parasympathetic: Salivary and lacrimal glands

4
Muscles of facial expression
Function Occipitofrontalis Raises eyebrows, wrinkles forehead horizontally Corrugator Supercilii Wrinkles forehead vertically Orbicularis Oculi Closes eye Orbicularis Oris Draws lips together Zygomaticus Major Elevates angle of the mouth (laughing) Buccinator Permits smiling; blowing / pursing of the lips
 Buccinator. Permits smiling; blowing / pursing of the lips.")
5
History Onset Progression Duration Unilateral/Bilateral
Associated symptoms Any hx of head trauma / surgery Immunisation hx (polio, rabies, tetanus & influenza) Recurrence PMHx
 Recurrence. PMHx.")
6
Symptoms Change in the appearance of the face
Difficulty closing one eye Difficulty making expressions, grimacing Difficulty with fine movements of the face Facial droop Difficulty eating (items fall out of the weak corner of the mouth) Face feels pulled to one side Face feels stiff Headache Impairment of taste Pain behind the ear Increased loudness of sound in one ear / Sensitivity to sound (hyperacusis)
 Face feels pulled to one side. Face feels stiff. Headache. Impairment of taste. Pain behind the ear. Increased loudness of sound in one ear / Sensitivity to sound (hyperacusis)")
7
Examination General systematic clinical examination
Full neurological examination, including focused cranial nerve examination Examination of the neck must be performed to illicit a parotid neoplasm or cervical lymphadenopathy

8
Cranial Nerves I - VI

9
Cranial Nerves VII - XII

10
Signs of Facial Nerve Paralysis
Facial asymmetry Eyebrow droop Inability to wrinkle forehead Drooping of corner of mouth Inability to close eye and uncontrolled tearing Unable to put hold lips tightly together

11
House-Brackmann scoring of facial function

12
Causes of Facial Nerve Palsy
Idiopathic Bell’s palsy (40-70%) Melkersson–Rosenthal syndrome (recurrent alternating facial palsy, furrowed tongue, faciolabial oedema)
 Melkersson–Rosenthal syndrome (recurrent alternating facial palsy, furrowed tongue, faciolabial oedema)")
13
Causes of Facial Nerve Palsy
2. Infection (13-36%) Otitis media Mumps Mastoiditis Infectious mononucleosis (glandular fever) Herpes zoster cephalicus (Ramsay–Hunt syndrome) Malaria Chickenpox Tuberculosis Encephalitis Lyme disease HIV Meningitis Poliomyelitis (type I)
 Otitis media. Mumps. Mastoiditis. Infectious mononucleosis (glandular fever) Herpes zoster cephalicus (Ramsay–Hunt syndrome) Malaria. Chickenpox. Tuberculosis. Encephalitis. Lyme disease. HIV. Meningitis. Poliomyelitis (type I)")
14
Causes of Facial Nerve Palsy
3. Trauma (19-21%) Skull base fractures Facial injuries Penetrating trauma to middle ear Barotrauma (altitude paralysis/scuba diving)
 Skull base fractures. Facial injuries. Penetrating trauma to middle ear. Barotrauma (altitude paralysis/scuba diving)")
15
Causes of Facial Nerve Palsy
4. Metabolic Diabetes mellitus Hypertension Acute porphyria

16
Causes of Facial Nerve Palsy
5. Neoplastic (2-3%) Cholesteatoma Leukaemia Haemophilia Fibrous dysplasia Parotid tumours Facial nerve tumour Cerebello-pontine angle tumours
 Cholesteatoma. Leukaemia. Haemophilia. Fibrous dysplasia. Parotid tumours. Facial nerve tumour. Cerebello-pontine angle tumours.")
17
Causes of Facial Nerve Palsy
6. Toxic Tetanus Diphtheria Thalidomide Carbon monoxide

18
Causes of Facial Nerve Palsy
7. Iatrogenic Postimmunisation Antitetanus serum Vaccine for rabies Parotid surgery Mastoid surgery Forceps delivery

19
Causes of Facial Nerve Palsy
8. Autoimmune syndrome Thrombotic thrombocytopaenic purpura Kawasaki disease Guillian barre/Miller–Fisher syndrome

20
Causes of Facial Nerve Palsy
9. Neurological Millard-Gubler syndrome (abducens palsy with contralateral haemiplegia due to lesion in the base of pons involving corticospinal tract) Opercular syndrome (cortical lesion in facial motor area)
 Opercular syndrome (cortical lesion in facial motor area)")
21
Causes of Facial Nerve Palsy
10. Congenital (8-14%) Dystrophia myotonica Moebius syndrome (facial diplegia associated with other cranial nerve deficits)
 Dystrophia myotonica. Moebius syndrome (facial diplegia associated with other cranial nerve deficits)")
22
Investigations Hearing test Consider MRI progressing > 3 weeks
lack of improvement after 6 months recurrent facial palsy single facial segment involvement high suspicion of an underlying neurological disorder

23
In the absence of other causes in the history or examination – presumed diagnosis is
Bell’s Palsy

24
Treatment Eye care Steroid +/- antiviral Surgical intervention
Artificial tears Moisturising eye ointment at night Protective eye wear Steroid +/- antiviral Surgical intervention

25
Prognosis of Bell’s Palsy
Good prognosis Most have recovery between 3 wks – 3mths If not recovering/progressively worse ? Underlying cause

26
Reviewing the evidence for treating Bell’s Palsy
Michael McGowan

27
WARNING Trying to read everything on these slides will cause your brain to melt.

28
Where to search?

30
No guideline but there is a CKS

31
Bell's palsy is an acute, unilateral, idiopathic, facial nerve paralysis. The paralysis also affects the eyelids, causing an impairment of blinking. The cause of Bell's palsy remains unclear, but it has been associated with the herpes virus. The annual incidence of Bell's palsy in the UK is 1 in 5000 people. It occurs most commonly between 15 and 60 years of age. When making a diagnosis of Bell’s palsy: It should be noted that maximum facial weakness develops within 2 days. Earache, pain behind the ear, aural fullness, or facial pain may precede the palsy. Severe pain might indicate Ramsay Hunt syndrome. This is caused by herpes zoster and is associated with a painful rash and herpetic vesicles. Confirmation that the paralysis is caused by a unilateral, lower motor neuron lesion is required. The muscles controlling facial expression are affected on one side of the face only. This may result in drooping of the brow and corner of the mouth, weakness of the frontalis (forehead muscle), or inability to close the eye. It should be confirmed that only the facial nerve is affected. Other features such as loss of taste of the anterior two-thirds of the tongue (on the same side as the facial weakness) may occur. Serious underlying pathology such as Lyme disease and parotid tumour should be excluded.
, or inability to close the eye. It should be confirmed that only the facial nerve is affected. Other features such as loss of taste of the anterior two-thirds of the tongue (on the same side as the facial weakness) may occur. Serious underlying pathology such as Lyme disease and parotid tumour should be excluded.")
32
To manage Bell’s palsy:
The person should be reassured that the prognosis is good: most people with Bell's palsy make a full recovery within 9 months. The person should be advised to keep the affected eye lubricated by using lubricating eye drops during the day and ointment at night. The eye should be taped closed at bedtime using microporous tape, if the ability to close the eye at night is impaired. For people presenting within 72 hours of the onset of symptoms, prescription of prednisolone should be considered. There are no data supporting the use of prednisolone in people presenting after 72 hours. Antiviral treatment is not recommended, either alone or in combination with prednisolone. If there is doubt regarding the diagnosis, or there is recurrent or bilateral Bell's palsy, an urgent referral to neurology or to an ear, nose, and throat (ENT) specialist should be arranged. If the cornea remains exposed after attempting to close the eyelid, an urgent referral to ophthalmology should be arranged.
 specialist should be arranged. If the cornea remains exposed after attempting to close the eyelid, an urgent referral to ophthalmology should be arranged.")
33
If the paralysis shows no sign of improvement after one month, or there is suspicion of a serious underlying diagnosis (e.g. cholesteatoma, parotid tumour, malignant otitis externa), an urgent referral to ENT should be arranged. If there is residual paralysis after 6–9 months, referral to a plastic surgeon with a special interest in facial reconstructive surgery should be considered.

34
So where do these recommendations come from?
To manage Bell’s palsy: The person should be reassured that the prognosis is good: most people with Bell's palsy make a full recovery within 9 months. The person should be advised to keep the affected eye lubricated by using lubricating eye drops during the day and ointment at night. The eye should be taped closed at bedtime using microporous tape, if the ability to close the eye at night is impaired. For people presenting within 72 hours of the onset of symptoms, prescription of prednisolone should be considered. There are no data supporting the use of prednisolone in people presenting after 72 hours. Antiviral treatment is not recommended, either alone or in combination with prednisolone. If there is doubt regarding the diagnosis, or there is recurrent or bilateral Bell's palsy, an urgent referral to neurology or to an ear, nose, and throat (ENT) specialist should be arranged. If the cornea remains exposed after attempting to close the eyelid, an urgent referral to ophthalmology should be arranged. So where do these recommendations come from?
 specialist should be arranged. If the cornea remains exposed after attempting to close the eyelid, an urgent referral to ophthalmology should be arranged. So where do these recommendations come from")
35
Steroids are well known to work.

36
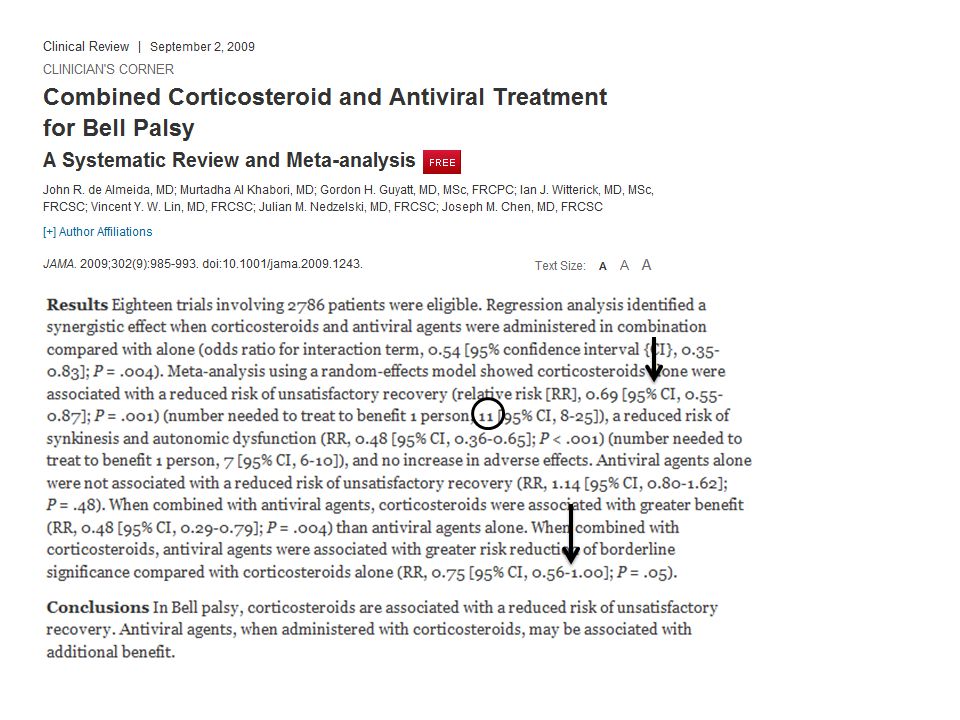
But what about using antivirals?

37
Read the abstract of this SR and talk about your conclusion

39
Significant

40
Not significant (just)
")
41
Steroids work Antivirals alone do not Might help in combination but there isn’t evidence to support this

42
Applying this evidence to children?

43
Applying this evidence to children?
Open to all sorts of bias, no randomisation Mirrors the adult recommendations Small numbers Outcome more or less the same

44
Probably alright to do so

45
Summary Outcome is good Supportive treatment a must
Improved by starting steroids within 72h Might be improved by using antivirals in combination Definitely not improved by using antivirals alone

46
And finally a point of interest…
If the paralysis shows no sign of improvement after one month, or there is suspicion of a serious underlying diagnosis (e.g. cholesteatoma, parotid tumour, malignant otitis externa), an urgent referral to ENT should be arranged. If there is residual paralysis after 6–9 months, referral to a plastic surgeon with a special interest in facial reconstructive surgery should be considered. And finally a point of interest…
, an urgent referral to ENT should be arranged. If there is residual paralysis after 6–9 months, referral to a plastic surgeon with a special interest in facial reconstructive surgery should be considered. And finally a point of interest…")
47
…In this guidline…

48
…were the evidence is appraised…

49
…Acupuncturists do better trials than ENT surgeons?

50
The End Questions for Elaine?

Similar presentations

 Lawrence Pike.>")

 in Drake et al.>")
 – herpes simplex virus Murakami (1996) 11/14.>")














