Download presentation
Presentation is loading. Please wait.

2
Dr / Essam M. Hafez Lecturer consultant of clinical toxicology M.D, clinical toxicology 12 June 20161

3
Alcohols are hydrocarbons that contain a hydroxyl group Alcohols are hydrocarbons that contain a hydroxyl group A compound with two hydroxyl groups is called a diol or a glycol A compound with two hydroxyl groups is called a diol or a glycol Toxic alcohols commonly refer to methanol, ethylene glycol and isopropyl alcohol Toxic alcohols commonly refer to methanol, ethylene glycol and isopropyl alcohol 12 June 20162

4
Secondary alcohol as isopropyl alcohol C 3 H 7 OH (H – C – OH) H H H (H – C – C – C - H) H H H HO H (H – C – C - OH) H H H H methanolmethanol methanol Primary alcohol as methanol CH 3 OH ethanol and ethanol C 2 H 5 OH Ethanol
 H H H (H – C – C – C - H) H H H HO H (H – C – C - OH) H H H H methanolmethanol methanol Primary alcohol as methanol CH 3 OH ethanol and ethanol C 2 H 5 OH Ethanol")
5
Ethylene glycol as ethanol attached with other hydroxyl group CH 2 OHCH 2 OH Ethylene glycol as ethanol attached with other hydroxyl group CH 2 OHCH 2 OH OH – C – C - OH H H H H tert butyl alcohol Tertiary alcohol as tert butyl alcohol (CH 3 ) 3 COH
 3 COH")
6
Ethanol (ethyl alcohol) beverages Ingredient of Food extract Ingredient of Food extract Cough and cold Medication Mouth washes Mouth washes It is available as Methanol ( methyl alcohol) It is widely used as an industrial marine solvent and paint remover photocopying fluid and wind shield-washing fluid
 beverages Ingredient of Food extract Ingredient of Food extract Cough and cold Medication Mouth washes Mouth washes It is available as Methanol ( methyl alcohol) It is widely used as an industrial marine solvent and paint remover photocopying fluid and wind shield-washing fluid")
7
Ethylene glycol Is used in many manufacturing process and as antifreeze Isopropanol (isopropyl alcohol) Used as disinfectantdisinfectant solventsolvent mouth washes skin lotion
 Used as disinfectantdisinfectant solventsolvent mouth washes skin lotion")
8
Alcohol is absorbed directly into the blood stream through the lining of the mouth and the tissue that lines the stomach and small intestine. Food, water, and fruit juice help to slow this absorption. Carbonated beverages speed the absorption of alcohol, which means that the drinker feels the effects sooner. Alcohol is absorbed directly into the blood stream through the lining of the mouth and the tissue that lines the stomach and small intestine. Food, water, and fruit juice help to slow this absorption. Carbonated beverages speed the absorption of alcohol, which means that the drinker feels the effects sooner.

9
Once alcohol (or ethanol, the chemical in alcoholic beverages) is in your bloodstream, it is carried to the brain and all the organs of your body within 90 seconds. The affects of alcohol vary according to the individual’s sex, body size, amount of body fat, the amount of alcohol consumed, the situation, and the amount of food in the stomach.

10
The liver is the largest glandular organ in the body. It is responsible for filtering 95% of ingested alcohol out of the body. An important fact to remember is that the body will eliminate 7-10 gm/h. So the more you drink, the longer the alcohol will remain in the body.

11
When the amount of alcohol consumed exceeds the liver’s ability to break down the alcohol, the concentration of alcohol in the bloodstream (the proportion of alcohol to blood in the body) increases. Increased blood alcohol concentrations (higher proportions of alcohol to blood) impair thought processes and coordination, and slow automatic functions such as breathing. Excessive blood alcohol concentration can lead to coma or possibly death.
 impair thought processes and coordination, and slow automatic functions such as breathing. Excessive blood alcohol concentration can lead to coma or possibly death..")
12
Methanol Ethylene Glycol Glycoxylate (lactic acidosis) Glycolic Acid (metabolic acidosis) Oxalate (cerebral & renal damage, hypocalcaemia) Formic Acid (metabolic acidosis) Acetaldehyde (hangover, flushing) Formaldehyde (blindness, cerebral oedema) Acetic Acid Alcohol Dehydrogenase Aldehyde Dehydrogenase Lactate dehydrogenase or glycolic acid oxidase Lactate dehydrogenase or aldehyde oxidase CO 2 + H 2 0
 Glycolic Acid (metabolic acidosis) Oxalate (cerebral & renal damage, hypocalcaemia) Formic Acid (metabolic acidosis) Acetaldehyde (hangover, flushing) Formaldehyde (blindness, cerebral oedema) Acetic Acid Alcohol Dehydrogenase Aldehyde Dehydrogenase Lactate dehydrogenase or glycolic acid oxidase Lactate dehydrogenase or aldehyde oxidase CO 2 + H 2 0")
13
Although effects will vary from person to person, the following are some short-term effects that may be experienced after moderate to light drinking: Distorted vision, hearing, and coordination Distorted vision, hearing, and coordination Altered perceptions and emotions Altered perceptions and emotions Anxiety Anxiety Slowed Breathing Slowed Breathing Mental confusion Mental confusion Memory loss Memory loss Increased aggression Increased aggression

14
Alcohol Dependence Alcohol Dependence Liver disease Liver disease Heart disease and stroke Heart disease and stroke Brain cell death Brain cell death Stomach ailments Stomach ailments Sexual impotence Sexual impotence Central Nervous System damage Central Nervous System damage Death Death

16
The legal system uses a more scientific method for determining when a person is drunk, Blood Alcohol Concentration (BAC,) the percentage of alcohol in the blood (or proportion of alcohol to blood in the body) as someone drinks. The legal system uses a more scientific method for determining when a person is drunk, Blood Alcohol Concentration (BAC,) the percentage of alcohol in the blood (or proportion of alcohol to blood in the body) as someone drinks. In most states, a BAC of.08% is considered legally drunk, which means that for every 1000 milliliters of blood, the body contains 8/10ths of a milliliter of alcohol. In most states, a BAC of.08% is considered legally drunk, which means that for every 1000 milliliters of blood, the body contains 8/10ths of a milliliter of alcohol.
 the percentage of alcohol in the blood (or proportion of alcohol to blood in the body) as someone drinks. In most states, a BAC of.08% is considered legally drunk, which means that for every 1000 milliliters of blood, the body contains 8/10ths of a milliliter of alcohol. In most states, a BAC of.08% is considered legally drunk, which means that for every 1000 milliliters of blood, the body contains 8/10ths of a milliliter of alcohol..")
17
1. BAC =.02 = Drinkers begin to feel moderate effects. 2. BAC =.04 = Most people begin to feel relaxed, mildly euphoric, sociable, and talkative. 3. BAC =.05 = Judgment, attention, and control are somewhat impaired. Ability to drive safely begins to be limited. Sensory- motor and finer performance are impaired. People are less able to make rational decisions about their capabilities (for example, about driving.) 4. BAC =.08 = This is legal level for intoxication in some states. There is a definite impairment of muscle coordination and driving skills. 5. BAC =.10 = This is legally drunk in most states. There is a clear deterioration of reaction time and control.
 4. BAC =.08 = This is legal level for intoxication in some states. There is a definite impairment of muscle coordination and driving skills. 5. BAC =.10 = This is legally drunk in most states. There is a clear deterioration of reaction time and control..")
18
Methanol Methanol Ethylene glycol Ethylene glycol Poisoning: Poisoning: Non accidental / suicide attempt Non accidental / suicide attempt Accidental Accidental Children Children Alcoholics Alcoholics

19
Methanol CH 3 OH Ethylene Glycol CH 2 OH-CHO Formaldehyde HCHO Glyoxalate CH 2 OH-CHO Formate HCOO - Glycolate CH 2 OH-COO - CO 2 + H 2 O Oxalate COO - -COO - + Ca 2+ Alcohols Metabolic acidosis Blindness Coma Coma & seizures Renal failure Myocarditis Hypocalcaemia Alcohol dehydrogenase Aldehyde dehydrogenase folate Acids

21
Also known as “ wood alcohol ” Also known as “ wood alcohol ” Used in industrial production, windshield wiper fluid, model airplane fuel and as a cleaning solvent Used in industrial production, windshield wiper fluid, model airplane fuel and as a cleaning solvent Sold as a mixture of ethanol and methanol in hardware stores in many countries Sold as a mixture of ethanol and methanol in hardware stores in many countries Approximately 1000 – 2000 cases of methanol intoxication per year Approximately 1000 – 2000 cases of methanol intoxication per year

22
Methanol itself is non-toxic Methanol itself is non-toxic Formaldehyde inhibits retinal oxidative phosphorylation but is rapidly metabolized to formic acid Formaldehyde inhibits retinal oxidative phosphorylation but is rapidly metabolized to formic acid Formic acid damages the optic disk leading to the characteristic visual impairments Formic acid damages the optic disk leading to the characteristic visual impairments Intoxication can occur with as little as 30 cc of ingestion Intoxication can occur with as little as 30 cc of ingestion

23
Often coingested with ethanol which makes diagnosis difficult and requires high index of suspicion Formic acid causes high anion gap metabolic acidosis and CNS depression causes a respiratory acidosis Methanol causes an elevated osmolar gap Methanol levels can be slow to obtain and not available in many labs. Levels > 20 mg/dL are associated with symptomatic presentations. Levels > 150 mg/dL are almost always fatal

24
Visual impairment common and often can lead to permanent blindness Visual impairment common and often can lead to permanent blindness Photophobia and abdominal pain are other common symptoms Photophobia and abdominal pain are other common symptoms Other signs of CNS depression including depressed respiratory rate, obtundation, and coma Other signs of CNS depression including depressed respiratory rate, obtundation, and coma Slow hepatic metabolizing can delay toxic effects for up to 24 hours after ingestion Slow hepatic metabolizing can delay toxic effects for up to 24 hours after ingestion

25
Initially may have no acid-base disorder due to long latent period while methanol is metabolized Initially may have no acid-base disorder due to long latent period while methanol is metabolized Later, typically develop a high anion gap metabolic acidosis - due to formic acid Later, typically develop a high anion gap metabolic acidosis - due to formic acid May also develop a respiratory acidosis secondary to CNS depression (with depression of respiratory centre and/or airway obstruction) May also develop a respiratory acidosis secondary to CNS depression (with depression of respiratory centre and/or airway obstruction) May occasionally present with normal anion gap acidosis if smaller ingestion May occasionally present with normal anion gap acidosis if smaller ingestion If patient is an alcoholic, there may other types of acidosis present as well If patient is an alcoholic, there may other types of acidosis present as well eg alcoholic ketoacidosis, starvation ketoacidosis, lactic acidosis, respiratory acidosis due aspiration, respiratory alkalosis due chronic liver disease eg alcoholic ketoacidosis, starvation ketoacidosis, lactic acidosis, respiratory acidosis due aspiration, respiratory alkalosis due chronic liver disease
 May also develop a respiratory acidosis secondary to CNS depression (with depression of respiratory centre and/or airway obstruction) May occasionally present with normal anion gap acidosis if smaller ingestion May occasionally present with normal anion gap acidosis if smaller ingestion If patient is an alcoholic, there may other types of acidosis present as well If patient is an alcoholic, there may other types of acidosis present as well eg alcoholic ketoacidosis, starvation ketoacidosis, lactic acidosis, respiratory acidosis due aspiration, respiratory alkalosis due chronic liver disease eg alcoholic ketoacidosis, starvation ketoacidosis, lactic acidosis, respiratory acidosis due aspiration, respiratory alkalosis due chronic liver disease")
26
Peripapillary edema, not shown Hyperemia of the optic disks and reduced papillary response to light,

27
putaminal necrosis = rigidity, tremor, masked faces, and monotonous speech; direct toxicity of formic acid on the brain and decreased cerebral flow

28
Mortality rates of 8-36% overall Mortality rates of 8-36% overall Mortality of 50-80% if pH < 7.1 on presentation Mortality of 50-80% if pH < 7.1 on presentation Visual defects persist in 20-25% of surivivors Visual defects persist in 20-25% of surivivors

29
Colorless, odorless, sweet tasting solvent Colorless, odorless, sweet tasting solvent Used in antifreeze, heat transfer fluids and runway deicers Used in antifreeze, heat transfer fluids and runway deicers Itself is non toxic Itself is non toxic Approximately 5800 cases of poisonings yearly Approximately 5800 cases of poisonings yearly Metabolized to glycolic acid and oxalic acid (excreted in urine) Metabolized to glycolic acid and oxalic acid (excreted in urine) Ingestion of as little as 30 cc can be fatal Ingestion of as little as 30 cc can be fatal Mortality rate of 1-22% Mortality rate of 1-22%
 Metabolized to glycolic acid and oxalic acid (excreted in urine) Ingestion of as little as 30 cc can be fatal Ingestion of as little as 30 cc can be fatal Mortality rate of 1-22% Mortality rate of 1-22%")
30
Can present with intoxication like symptoms without odor Can present with intoxication like symptoms without odor Anion gap metabolic acidosis with elevated osmolal gap Anion gap metabolic acidosis with elevated osmolal gap Hypocalcemia from deposition of calcium oxalate in tissues Hypocalcemia from deposition of calcium oxalate in tissues Within 12 hours of ingestion nausea, vomiting, hypocalcemia and CNS depression can occur Within 12 hours of ingestion nausea, vomiting, hypocalcemia and CNS depression can occur This is followed by tachycardia and tachypnea from 12- 24 hours of ingestion This is followed by tachycardia and tachypnea from 12- 24 hours of ingestion Renal failure typically occurs around 24 hours post ingestion Renal failure typically occurs around 24 hours post ingestion

31
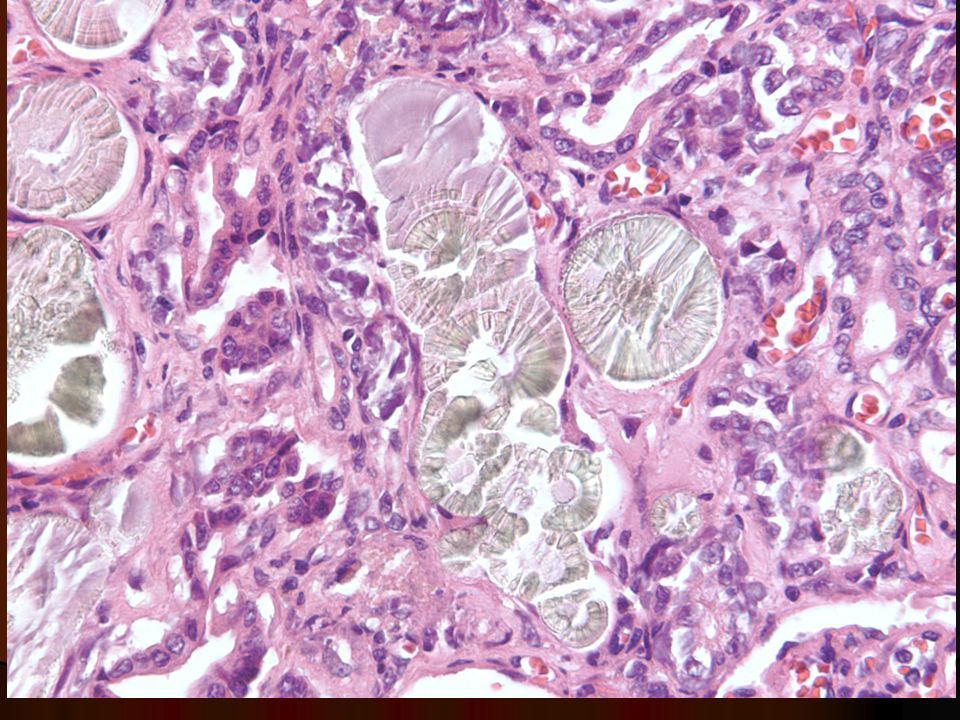
Clinical history Clinical history Elevated osmolal gap Elevated osmolal gap Anion gap acidosis with or without the presence of lactic acid Anion gap acidosis with or without the presence of lactic acid Calcium oxalate crystals in the urine which present 4 hours after ingestion Calcium oxalate crystals in the urine which present 4 hours after ingestion Crystals are initially envelope shaped dihydrate crystals and later are needle shaped monohydrate crystals Crystals are initially envelope shaped dihydrate crystals and later are needle shaped monohydrate crystals Urine can be tested with UV light to test for sodium flourescein Urine can be tested with UV light to test for sodium flourescein Confirmation with serum ethylene glycol level Confirmation with serum ethylene glycol level

36
Colorless liquid with bitter taste Colorless liquid with bitter taste Used in rubbing alcohol, nail-polish remover, glues, and in industrial solvents Used in rubbing alcohol, nail-polish remover, glues, and in industrial solvents Toxic dose of 2-4 mL/kg (approximately 200 mL of rubbing alcohol for an adult) Toxic dose of 2-4 mL/kg (approximately 200 mL of rubbing alcohol for an adult) 11,216 exposures to isopropanol occurred in 1998 11,216 exposures to isopropanol occurred in 1998 Metabolized in liver by alcohol dehydogenase to acetone Metabolized in liver by alcohol dehydogenase to acetone 20-50% excreted unchanged in the urine 20-50% excreted unchanged in the urine
 Toxic dose of 2-4 mL/kg (approximately 200 mL of rubbing alcohol for an adult) 11,216 exposures to isopropanol occurred in ,216 exposures to isopropanol occurred in 1998 Metabolized in liver by alcohol dehydogenase to acetone Metabolized in liver by alcohol dehydogenase to acetone 20-50% excreted unchanged in the urine 20-50% excreted unchanged in the urine")
37
Presents with symptoms of intoxication, respiratory depression, nausea, vomiting, gastritis Presents with symptoms of intoxication, respiratory depression, nausea, vomiting, gastritis Fruity breath from acetone production is characteristic of ingestion Fruity breath from acetone production is characteristic of ingestion Symptoms occur within 1 hour of ingestion Symptoms occur within 1 hour of ingestion Metabolically presents with ketosis without acidosis Metabolically presents with ketosis without acidosis An elevated osmolal gap will be present An elevated osmolal gap will be present Hypoglycemia common due to inhibition of gluconeogenesis Hypoglycemia common due to inhibition of gluconeogenesis Ethanol drip and fomepizole have no role no toxic metabolites are formed Ethanol drip and fomepizole have no role no toxic metabolites are formed Hemodialysis indicated for isopropanol levels > 400 mg/dL or with significant CNS depression or renal failure Hemodialysis indicated for isopropanol levels > 400 mg/dL or with significant CNS depression or renal failure Severe overdose can result in coma or death, but mortality occurring in < 0.05% of all exposure Severe overdose can result in coma or death, but mortality occurring in < 0.05% of all exposure

38
Plasma concentration Plasma concentration Metabolic acidosis Metabolic acidosis The Gaps: The Gaps: High anion gap High anion gap High osmolar gap High osmolar gap ‘ Lactate gap ’ ‘ Lactate gap ’ Calcium level Calcium level Urine: Urine: Urinalysis: oxaluria (Calcium oxalate crystals) Urinalysis: oxaluria (Calcium oxalate crystals) Wood ’ s lamp Wood ’ s lamp
 Urinalysis: oxaluria (Calcium oxalate crystals) Wood ’ s lamp Wood ’ s lamp")
39
Exposure to ingested alcohol estimated by measuring osmolar gap Exposure to ingested alcohol estimated by measuring osmolar gap Indicates appreciable quantities of low molecular weight substances Indicates appreciable quantities of low molecular weight substances Measured osmolality - Calculated osmolality Measured osmolality - Calculated osmolality Calculated = 1.86 x (Na, K) + glucose + urea (mmol/L) Calculated = 1.86 x (Na, K) + glucose + urea (mmol/L) Calculated = (1.86 x [Na]) + [glucose] + [urea] + 9 Calculated = (1.86 x [Na]) + [glucose] + [urea] + 9 Measured: determined by freezing point depression Measured: determined by freezing point depression
![Exposure to ingested alcohol estimated by measuring osmolar gap Exposure to ingested alcohol estimated by measuring osmolar gap Indicates appreciable quantities of low molecular weight substances Indicates appreciable quantities of low molecular weight substances Measured osmolality - Calculated osmolality Measured osmolality - Calculated osmolality Calculated = 1.86 x (Na, K) + glucose + urea (mmol/L) Calculated = 1.86 x (Na, K) + glucose + urea (mmol/L) Calculated = (1.86 x [Na]) + [glucose] + [urea] + 9 Calculated = (1.86 x [Na]) + [glucose] + [urea] + 9 Measured: determined by freezing point depression Measured: determined by freezing point depression](http://images.slideplayer.com/35/10490644/slides/slide_39.jpg "Exposure to ingested alcohol estimated by measuring osmolar gap Exposure to ingested alcohol estimated by measuring osmolar gap Indicates appreciable quantities of low molecular weight substances Indicates appreciable quantities of low molecular weight substances Measured osmolality - Calculated osmolality Measured osmolality - Calculated osmolality Calculated = 1.86 x (Na, K) + glucose + urea (mmol/L) Calculated = 1.86 x (Na, K) + glucose + urea (mmol/L) Calculated = (1.86 x [Na]) + [glucose] + [urea] + 9 Calculated = (1.86 x [Na]) + [glucose] + [urea] + 9 Measured: determined by freezing point depression Measured: determined by freezing point depression")
40
Ethylene glycol ingestion Ethylene glycol ingestion Methanol ingestion Methanol ingestion Formaldehyde ingestion Formaldehyde ingestion Paraldehyde ingestion Paraldehyde ingestion DKA DKA Alcoholic ketoacidosis Alcoholic ketoacidosis Lactic acidosis Lactic acidosis

41
Alerts you to the diagnosis before the acidosis develops Alerts you to the diagnosis before the acidosis develops Osmolar gap: presence of alcohols Osmolar gap: presence of alcohols Anion gap: presence of acid metabolites Anion gap: presence of acid metabolites Early: high OG, normal AG Early: high OG, normal AG Late: normal OG, high AG Late: normal OG, high AG

42
Gap > 10 mmol/L significant Gap > 10 mmol/L significant Can estimate serum level of toxic alcohol by conversion factor. Can estimate serum level of toxic alcohol by conversion factor. Ethylene glycol 6.2 Ethylene glycol 6.2 Methanol 3.2 Methanol 3.2 ethanol 4.6 ethanol 4.6 Need to subtract ethanol contribution Need to subtract ethanol contribution (To convert ethanol levels in mg/dl to mmol/l divide by 4.6.) (To convert ethanol levels in mg/dl to mmol/l divide by 4.6.)
 (To convert ethanol levels in mg/dl to mmol/l divide by 4.6.).")
43
([Na + ] + [K + ]) - ([Cl - ] + [HCO 3 - ]) ([Na + ] + [K + ]) - ([Cl - ] + [HCO 3 - ]) Measures the difference between conc of unmeasured anions & cations Measures the difference between conc of unmeasured anions & cations Normal 12-18mmol/L Normal 12-18mmol/L High anion gap: High anion gap: Ketoacidosis Ketoacidosis Lactic acidosis Lactic acidosis Renal failure Renal failure Poisoning: paracetamol,methanol, ethylene glycol, salicyclates,paraldehyde, formaldehyde,toluene Poisoning: paracetamol,methanol, ethylene glycol, salicyclates,paraldehyde, formaldehyde,toluene
![([Na + ] + [K + ]) - ([Cl - ] + [HCO 3 - ]) ([Na + ] + [K + ]) - ([Cl - ] + [HCO 3 - ]) Measures the difference between conc of unmeasured anions & cations Measures the difference between conc of unmeasured anions & cations Normal 12-18mmol/L Normal 12-18mmol/L High anion gap: High anion gap: Ketoacidosis Ketoacidosis Lactic acidosis Lactic acidosis Renal failure Renal failure Poisoning: paracetamol,methanol, ethylene glycol, salicyclates,paraldehyde, formaldehyde,toluene Poisoning: paracetamol,methanol, ethylene glycol, salicyclates,paraldehyde, formaldehyde,toluene](http://images.slideplayer.com/35/10490644/slides/slide_43.jpg "([Na + ] + [K + ]) - ([Cl - ] + [HCO 3 - ]) ([Na + ] + [K + ]) - ([Cl - ] + [HCO 3 - ]) Measures the difference between conc of unmeasured anions & cations Measures the difference between conc of unmeasured anions & cations Normal 12-18mmol/L Normal 12-18mmol/L High anion gap: High anion gap: Ketoacidosis Ketoacidosis Lactic acidosis Lactic acidosis Renal failure Renal failure Poisoning: paracetamol,methanol, ethylene glycol, salicyclates,paraldehyde, formaldehyde,toluene Poisoning: paracetamol,methanol, ethylene glycol, salicyclates,paraldehyde, formaldehyde,toluene")
44
Anion Gap Anion Gap A: Alcohol A: Alcohol T: Toluene T: Toluene M: Methanol M: Methanol U: Uraemia U: Uraemia D: DKA D: DKA P: Paraldehyde P: Paraldehyde I: Iron, Isoniazid I: Iron, Isoniazid L: Lactic acidosis L: Lactic acidosis E: Ethylene glycol E: Ethylene glycol S: Salicylates S: Salicylates Osmolar gap Osmolar gap M: Methanol M: Methanol E: Ethanol E: Ethanol D: Diuretics D: Diuretics I: Isopropanol I: Isopropanol E: Ethylene glycol E: Ethylene glycol

45
False positive elevation in point of care analysers: Radiometer analyser. False positive elevation in point of care analysers: Radiometer analyser. Most lactate analysers use lactate oxidase. Most lactate analysers use lactate oxidase. This cross reacts with EG metabolites. This cross reacts with EG metabolites. Useful in late presentation. Useful in late presentation. Could indicate when dialysis can stop. Could indicate when dialysis can stop. Canadian medical association journal, April 10th 2007

46
Early suspicion & treatment essential Delays lead to Renal failure Death

47
Ethylene glycol level > 20mg/dL Ethylene glycol level > 20mg/dL Definite history of ingestion & osmolal gap >10mosm/L Definite history of ingestion & osmolal gap >10mosm/L Suspicion of intoxication plus at least 2 of: Suspicion of intoxication plus at least 2 of: pH<7.3 pH<7.3 HCO 3 <20mmol/L HCO 3 <20mmol/L Osmol gap >10 Osmol gap >10 Oxaluria Oxaluria

49
1. Supportive care: ABC 2. Antidotes: Block mechanism Ethanol (competitive ADH substrate) Ethanol (competitive ADH substrate) Fomepizole (ADH inhibitor) Fomepizole (ADH inhibitor) 3. Haemodialysis: Remove agent Remove the toxic alcohol & its metabolites Remove the toxic alcohol & its metabolites Correct acidosis Correct acidosis ARF ARF Methanol: Shortens hospitalisation Methanol: Shortens hospitalisation 4. NaHCO 3 IVI Correct metabolic acidosis (pH<7.2) Correct metabolic acidosis (pH<7.2) Increase renal excretion of glycolate & formate Increase renal excretion of glycolate & formate Inhibit precipitation of calcium oxalate Inhibit precipitation of calcium oxalate
 Ethanol (competitive ADH substrate) Fomepizole (ADH inhibitor) Fomepizole (ADH inhibitor) 3. Haemodialysis: Remove agent Remove the toxic alcohol & its metabolites Remove the toxic alcohol & its metabolites Correct acidosis Correct acidosis ARF ARF Methanol: Shortens hospitalisation Methanol: Shortens hospitalisation 4. NaHCO 3 IVI Correct metabolic acidosis (pH<7.2) Correct metabolic acidosis (pH<7.2) Increase renal excretion of glycolate & formate Increase renal excretion of glycolate & formate Inhibit precipitation of calcium oxalate Inhibit precipitation of calcium oxalate.")
50
Ethanol: Ethanol: ethanol is a strong competitive inhibitor of methanol at the alcohol dehydrogenase enzyme ethanol is a strong competitive inhibitor of methanol at the alcohol dehydrogenase enzyme 4- Methyl-Pyrazole: (4-MP= fomepizole) 4- Methyl-Pyrazole: (4-MP= fomepizole) Action: alcohol dehydrogenase inhibitor. Action: alcohol dehydrogenase inhibitor. Folic acid and folinic acid:( Leucoverin) converts formic acid to CO2 and water i.e. it enhance methanol elimination. converts formic acid to CO2 and water i.e. it enhance methanol elimination. 12 June 201649
 converts formic acid to CO2 and water i.e. it enhance methanol elimination. converts formic acid to CO2 and water i.e. it enhance methanol elimination. 12 June")
51
Ethanol is a competitive inhibitor of ADH. It ’ s affinity for ADH is 10-20 times greater than that of methanol. Ethanol slows the rate of methanol ’ s conversion to formaldehyde and formic acid, allowing the body time to excrete methanol in the breath and urine. Ethanol is a competitive inhibitor of ADH. It ’ s affinity for ADH is 10-20 times greater than that of methanol. Ethanol slows the rate of methanol ’ s conversion to formaldehyde and formic acid, allowing the body time to excrete methanol in the breath and urine. MethanolFormaldehyde Formic Acid Ethanol - - ADH

52
Competitively inhibits ADH, thus reducing toxic metabolite production. Competitively inhibits ADH, thus reducing toxic metabolite production. Requires PO or IVI administration Requires PO or IVI administration Requires intoxicating doses Requires intoxicating doses Accepted target 100-125mg/dL Accepted target 100-125mg/dL Risks with Rx Risks with Rx Intoxicated: require close monitoring Intoxicated: require close monitoring Hypoglycaemia Hypoglycaemia Potential hepatotoxicity Potential hepatotoxicity Kinetics unpredictable; requires monitoring &adjustment Kinetics unpredictable; requires monitoring &adjustment

53
4-methylpyrazole (4MP) 4-methylpyrazole (4MP) Potent inhibitor of ADH Potent inhibitor of ADH Has an affinity for ADH x 500-1000 of ethanol Has an affinity for ADH x 500-1000 of ethanol Limited toxicity Limited toxicity Safely used in France since 1981(1) Safely used in France since 1981(1) 2 US multi centre prospective trials confirmed efficacy(2,3) 2 US multi centre prospective trials confirmed efficacy(2,3) 1.Megarbane B, Borron SW, Trout H et al. treatment of acute methanol poisoning with fomepizole. Intensive Care Med. 2001. 27:1370-1378 2.Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of ethylene glycol poisoning. NEJM. 1999. 340:832-838 3.Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of methanol poisoning. NEJM. 2001. 344:424-429

54
12 June 201653 CH 3 OH CH 2 O CHOOH CO 2 + H 2 O Methanol Formaldehyde Formic Acid Folate AD H X Fompepizole Ethanol

55
12 June 201654 Fomepizole …

56
Loading dose 15mg/kg Loading dose 15mg/kg Then 10mg/kg every 12 hours until alcohol level <0.2g/L (BD dosing) Then 10mg/kg every 12 hours until alcohol level <0.2g/L (BD dosing) Subsequent doses tapered Subsequent doses tapered
 Then 10mg/kg every 12 hours until alcohol level <0.2g/L (BD dosing) Subsequent doses tapered Subsequent doses tapered")
57
Expensive (esp if used empirically) Expensive (esp if used empirically) CI: allergy, pregnancy CI: allergy, pregnancy Headache 12% Headache 12% Nausea 11% Nausea 11% Dizziness 7% Dizziness 7% Injection site irritation Injection site irritation Usual: rash, vertigo, fever, transient LFT derangement, eosinophilia Usual: rash, vertigo, fever, transient LFT derangement, eosinophilia
 Expensive (esp if used empirically) CI: allergy, pregnancy CI: allergy, pregnancy Headache 12% Headache 12% Nausea 11% Nausea 11% Dizziness 7% Dizziness 7% Injection site irritation Injection site irritation Usual: rash, vertigo, fever, transient LFT derangement, eosinophilia Usual: rash, vertigo, fever, transient LFT derangement, eosinophilia")
58
Ethanol: - Oral or IV - CNS depression - Difficult titration - Frequent levels - Hypoglycemia Fomepizole: - IV - No CNS depression - Easy dosing - No levels to monitor - More predictable pharmacokinetcs pharmacokinetcs - No Hypoglycemia - Cost 12 June 201657

59
Fomepizole Due to efficacy & safety profile Due to efficacy & safety profile Recommended as 1st line antidote in confirmed ethylene glycol / methanol poisoning Recommended as 1st line antidote in confirmed ethylene glycol / methanol poisoning Also recommend initial fomepizole dose Also recommend initial fomepizole dose Suspicion of toxic alcohol ingestion Suspicion of toxic alcohol ingestion In presence of metabolic acidosis with elevated anion gap unexplained by equivalent increase in serum lactate In presence of metabolic acidosis with elevated anion gap unexplained by equivalent increase in serum lactate

60
Considered integral part of treatment Considered integral part of treatment Expediate removal of alcohol & toxic metabolites Expediate removal of alcohol & toxic metabolites Reduces necessary duration of antidotal treatment Reduces necessary duration of antidotal treatment Both ethylene glycol & methanol effectively cleared by HD Both ethylene glycol & methanol effectively cleared by HD End point : End point : alcohol conc <0.2g/L alcohol conc <0.2g/L Resolution acid base balance Resolution acid base balance Resolution anion gap Resolution anion gap ?Resolution of lactate gap ?Resolution of lactate gap

61
NEJM 1999, Brent et al Started after initial loading dose if: Started after initial loading dose if: pH <7.1 pH <7.1 pH decrease of >0.05 despite IV HCO 3. pH decrease of >0.05 despite IV HCO 3. pH <7.3 despite IV HCO 3. pH <7.3 despite IV HCO 3. decrease >5mmol/L HCO 3 despite IV HCO 3. decrease >5mmol/L HCO 3 despite IV HCO 3. Creatinine >265 mol/L, or increase >88 mol/L. Creatinine >265 mol/L, or increase >88 mol/L. Initial ethylene glycol conc >50mg/dL (8.1mmol/L) Initial ethylene glycol conc >50mg/dL (8.1mmol/L)
 Initial ethylene glycol conc >50mg/dL (8.1mmol/L).")
62
Fomepizole should be administered to slow down conversion of methanol to formic acid Fomepizole should be administered to slow down conversion of methanol to formic acid Ethanol (when fomepizole is unavailable) administered via central line to competitively inhibit metabolism of methanol (required serum ethanol concentration of at least 100 mg/dL) Ethanol (when fomepizole is unavailable) administered via central line to competitively inhibit metabolism of methanol (required serum ethanol concentration of at least 100 mg/dL) Hemodialysis effectively removes methanol Hemodialysis effectively removes methanol During dialysis, ethanol and fomepizole is also removed which can increase the levels of formic acid unless adjusted for During dialysis, ethanol and fomepizole is also removed which can increase the levels of formic acid unless adjusted for Folic acid supplement to enhance the metabolism of formic acid Folic acid supplement to enhance the metabolism of formic acid American Academy of Clinical Toxicology recommends dialysis for severe metabolic acidosis, presence of visual symptoms, serum methanol concentration > 50 mg/dL, or severe electrolyte disturbances American Academy of Clinical Toxicology recommends dialysis for severe metabolic acidosis, presence of visual symptoms, serum methanol concentration > 50 mg/dL, or severe electrolyte disturbances Confirmed history of ingestion of more than 30 cc (0.4 mg/kg body weight) also used as an indication for dialysis Confirmed history of ingestion of more than 30 cc (0.4 mg/kg body weight) also used as an indication for dialysis
 administered via central line to competitively inhibit metabolism of methanol (required serum ethanol concentration of at least 100 mg/dL) Ethanol (when fomepizole is unavailable) administered via central line to competitively inhibit metabolism of methanol (required serum ethanol concentration of at least 100 mg/dL) Hemodialysis effectively removes methanol Hemodialysis effectively removes methanol During dialysis, ethanol and fomepizole is also removed which can increase the levels of formic acid unless adjusted for During dialysis, ethanol and fomepizole is also removed which can increase the levels of formic acid unless adjusted for Folic acid supplement to enhance the metabolism of formic acid Folic acid supplement to enhance the metabolism of formic acid American Academy of Clinical Toxicology recommends dialysis for severe metabolic acidosis, presence of visual symptoms, serum methanol concentration > 50 mg/dL, or severe electrolyte disturbances American Academy of Clinical Toxicology recommends dialysis for severe metabolic acidosis, presence of visual symptoms, serum methanol concentration > 50 mg/dL, or severe electrolyte disturbances Confirmed history of ingestion of more than 30 cc (0.4 mg/kg body weight) also used as an indication for dialysis Confirmed history of ingestion of more than 30 cc (0.4 mg/kg body weight) also used as an indication for dialysis")
63
Activated charcoal ineffective Activated charcoal ineffective Gastric lavage only effective within 1 hour of ingestion Gastric lavage only effective within 1 hour of ingestion Ethanol infusion if fomepizole not available (loading dose of 0.6 g ethanol/kg followed by constant infusion to target levels 100-200 mg/dL) Ethanol infusion if fomepizole not available (loading dose of 0.6 g ethanol/kg followed by constant infusion to target levels 100-200 mg/dL) Fomepizole now used to competively inhibit metabolism Fomepizole now used to competively inhibit metabolism Bicarbonate to correct acidosis Bicarbonate to correct acidosis Volume expansion increases excretion of ethylene glycol and may prevent crystal induced renal failure Volume expansion increases excretion of ethylene glycol and may prevent crystal induced renal failure Hemodialysis effectively removes ethylene glycol with mean clearance rate of 145-230 ml/min Hemodialysis effectively removes ethylene glycol with mean clearance rate of 145-230 ml/min
 Ethanol infusion if fomepizole not available (loading dose of 0.6 g ethanol/kg followed by constant infusion to target levels mg/dL) Fomepizole now used to competively inhibit metabolism Fomepizole now used to competively inhibit metabolism Bicarbonate to correct acidosis Bicarbonate to correct acidosis Volume expansion increases excretion of ethylene glycol and may prevent crystal induced renal failure Volume expansion increases excretion of ethylene glycol and may prevent crystal induced renal failure Hemodialysis effectively removes ethylene glycol with mean clearance rate of ml/min Hemodialysis effectively removes ethylene glycol with mean clearance rate of ml/min")
64
General rule: actively investigate for toxic ingestion if pt has high anion gap acidosis in absence of ketoacidosis, lactic acidosis or renal failure. General rule: actively investigate for toxic ingestion if pt has high anion gap acidosis in absence of ketoacidosis, lactic acidosis or renal failure. Treatment can be life saving if early. Treatment can be life saving if early. High index suspicion esp if pt appears intoxicated +/- neuro symptoms High index suspicion esp if pt appears intoxicated +/- neuro symptoms Always check osmolar gap Always check osmolar gap > 10 suspect EG, methanol, ethanol > 10 suspect EG, methanol, ethanol Don’t be put off by a normal AG or OG as both can occur even in life threatening ingestion. Don’t be put off by a normal AG or OG as both can occur even in life threatening ingestion.

65
Elevated osmolal gap can be suggestive of toxic alcohol ingestions Elevated osmolal gap can be suggestive of toxic alcohol ingestions Serum levels of toxic alcohols are often too slow to aide in guiding therapy Serum levels of toxic alcohols are often too slow to aide in guiding therapy Fomepizole is a safe and effective adjunct to hemodialysis to limit toxicity associated with methanol and ethylene glycol ingestion Fomepizole is a safe and effective adjunct to hemodialysis to limit toxicity associated with methanol and ethylene glycol ingestion

66
Megarbane B, Borron S.W, Baud F.J. Current recommendations for treatment of severe toxic alcohol poisonings.Intensive Care Med (2005) 31:189-195 Megarbane B, Borron S.W, Baud F.J. Current recommendations for treatment of severe toxic alcohol poisonings.Intensive Care Med (2005) 31:189-195 Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of ethylene glycol poisoning. NEJM (1999) 340; (11):832-838 Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of ethylene glycol poisoning. NEJM (1999) 340; (11):832-838 Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of methanol poisoning. NEJM (2001); 344:424-429 Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of methanol poisoning. NEJM (2001); 344:424-429 Brindley P.G, Butler M.S, Cembrowski G, Brindley D.N. Falsely elevated point of care lactate measurement after ingestion of ethylene glycol. Canadian Medical Association Journal (2007) 176;(8):1097-1099 Brindley P.G, Butler M.S, Cembrowski G, Brindley D.N. Falsely elevated point of care lactate measurement after ingestion of ethylene glycol. Canadian Medical Association Journal (2007) 176;(8):1097-1099
 31: Megarbane B, Borron S.W, Baud F.J. Current recommendations for treatment of severe toxic alcohol poisonings.Intensive Care Med (2005) 31: Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of ethylene glycol poisoning. NEJM (1999) 340; (11): Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of ethylene glycol poisoning. NEJM (1999) 340; (11): Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of methanol poisoning. NEJM (2001); 344: Brent J, McMartin K, Phillips S et al. Fomepizole for the treatment of methanol poisoning. NEJM (2001); 344: Brindley P.G, Butler M.S, Cembrowski G, Brindley D.N. Falsely elevated point of care lactate measurement after ingestion of ethylene glycol. Canadian Medical Association Journal (2007) 176;(8): Brindley P.G, Butler M.S, Cembrowski G, Brindley D.N. Falsely elevated point of care lactate measurement after ingestion of ethylene glycol. Canadian Medical Association Journal (2007) 176;(8):")
Similar presentations







>")

, the active ingredient in alcohol, is produced by yeast cells acting on carbohydrates in fruits and grains. Ethyl.>")












 concentration. More H + = more acidic = lower.>")



>")