Download presentation
Presentation is loading. Please wait.

1
Fetal Growth in pregnancies affected by substance misuse

2
Objectives Examine association of substance abuse with fetal growth problems Identify commonly used illicit substances and their effect on fetal growth Fetal surveillance in pregnancies with substance misuse Interventions to improve fetal outcome

3
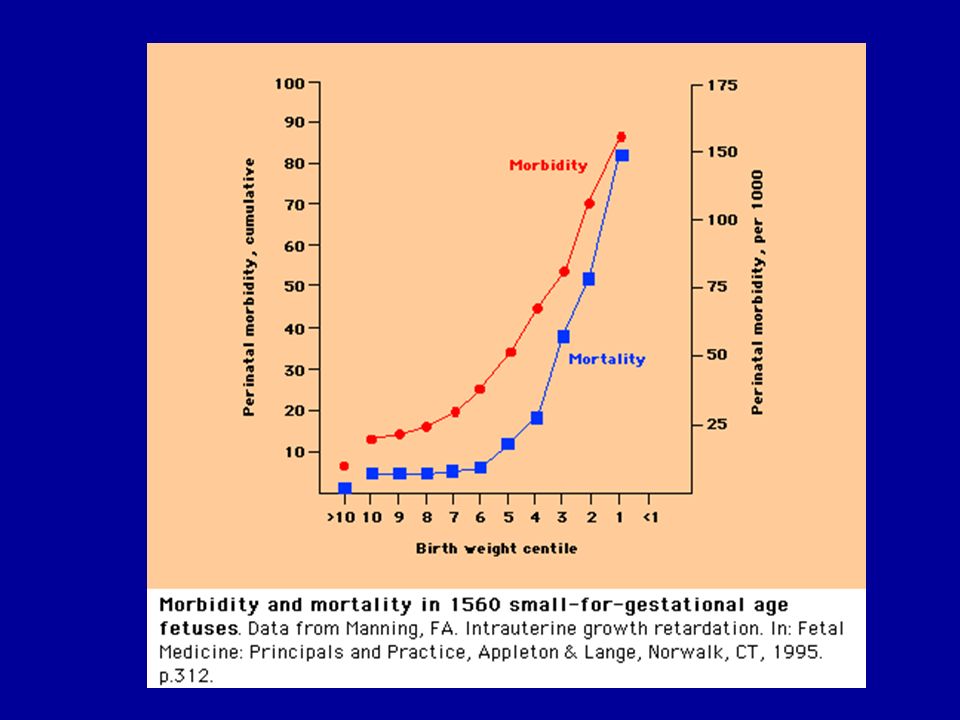
Small babies contribute disproportionately to perinatal morbidity and mortality The main contributor to this association is FGR rather than SFD The increased morbidity and mortality is a result of intrauterine hypoxia, acidaemia, prematurity (often iatrogenic) and neonatal complications
 and neonatal complications")
5
Does substance misuse affect fetal growth?

6
Scottish drug misuse statistics report normal birth weight in >75% of women who report substance misuse

7
Smoking: Both active and passive smoking are associated with a significant weight deficit (460 g and 200 g respectively) Marijuana: 79 g Heroin: 489 g Methadone: 279 g Combined Methadone and Heroin: 557 g Reported weight deficit
 Marijuana: 79 g Heroin: 489 g Methadone: 279 g Combined Methadone and Heroin: 557 g Reported weight deficit")
8
Substance misuse may be associated with FGR, but are illicit drugs?

9
Substance misuse IS associated with FGR, but are illicit drugs? It remains difficult to prove an independent effect on fetal growth for most common substances.

10
Do illicit drugs affect fetal growth? Studies are fraught with difficulties Not possible to conduct trials Data largely from epidemiological studies and animal models Lots of confounding variables Socioeconomic factors/poverty Domestic violence Legal drugs Smoking/alcohol Multiple illicit drugs Nutrition Associated health issues LBW often 2 o to prematurity

11
How can illicit drugs affect fetal growth? Normal small Abnormal small Infected small Starved small Wrong small

12
Inhibits presynaptic uptake of sympathomimetic neurotransmitters including norepinephrine, serotonin and dopamine Hypertension, tachycardia and myocardial ischaemia Rapid transfer across the placenta to the fetus by simple diffusion; may cause significant vasoconstriction of fetal blood vessels. Indirect fetal effects of cocaine result from maternal vasoconstriction. Since uterine blood flow is not autoregulated, decreased blood flow may lead to uteroplacental insufficiency, acidosis and fetal hypoxia It is associated with villous haemorrhage even in the absence of abruption Cocaine

13
Indirect acting sympathomimetic drugs, that produce powerful central nervous system stimulation with peripheral α and β-adrenergic receptor actions Result in euphoria, increased cortical alertness, decreased fatigue and appetite suppression. Clinically indistinguishable from effects caused by cocaine. Hypertension, arrhythmias, tachycardia, dilated pupils, hyperreflexia, proteinuria, and confusion have all been reported. Adverse pregnancy outcome with prenatal exposure to amphetamines: Congenital malformation, FGR, IUD and cerebral haemorrhage have been reported. Targets noradrenalin and serotonin transporters in the placenta Amphetamines

14
THC crosses the placenta freely and has a direct effect on the fetus FGR occurs largely in mice No obvious effect on placenta Confounded by the fact that it is usually smoked with tobacco Marijuana (THC)
")
15
Smoking increases resistance in the umbilical artery, and may reduce intervillous blood flow Nicotine impairs placental nutrient transfer Carbon monoxide impairs oxygen delivery to the fetus by displacing oxygen from maternal haemoglobin, and diminishes oxygen carrying capacity of fetal blood Smoking

16
Intravenous opioid abuse in pregnancy may affect the fetus indirectly (e.g. maternal malnutrition or infection) or directly (e.g. transplacental opioid transfer). FGR and fetal distress are described consequences of opiate addiction. Increased permeability of placenta, particularly where Heroin combined with Methadone. Opiates
 or directly (e.g. transplacental opioid transfer). FGR and fetal distress are described consequences of opiate addiction. Increased permeability of placenta, particularly where Heroin combined with Methadone. Opiates.")
17
Benzodiazepines- some effect on growth described but no clear mechanism, more concerns about teratogenicity MDMA- no data on growth to date Volatile substances- prematurity Other

18
Antenatal surveillance Given the association between substance misuse in pregnancy and low birth weight, antenatal fetal surveillance should follow principles of high risk pregnancy care Serial ultrasound & Doppler assessment of the fetus should be offered This will allow: Early diagnosis of at risk/small fetuses Utilising intensive surveillance where required Avoiding unnecessary intervention where fetal assessment is normal Planning timing/mode of delivery

19
Antenatal surveillance Considerations One size doesn’t fit all- some patients will be higher risk than others Patients misusing vasoactive substances may have significant placental disease- expected timelines of deterioration may not apply Compliance- pragmatic approach to timetable, may need to be opportunistic; accurate dating may be difficult Complacency- remember other causes for FGR Anomalies- some drugs used in first trimester may be teratogenic/vascular disruption etc

20
Antenatal surveillance Example fetal growth surveillance plan for a high risk pregnancy: Routine dating USS in first trimester (± nuchal translucency) AFP in second trimester (additional risk factor) Detailed USS at 20 weeks + uterine artery Doppler Serial growth scans at 28-32-36 weeks gestation, looking at centile position AND velocity of AC/EFW, also including HC (risk of microcephaly), AFI, UMA If any abnormal findings, need to adapt frequency/perform additional assessments
 AFP in second trimester (additional risk factor) Detailed USS at 20 weeks + uterine artery Doppler Serial growth scans at weeks gestation, looking at centile position AND velocity of AC/EFW, also including HC (risk of microcephaly), AFI, UMA If any abnormal findings, need to adapt frequency/perform additional assessments")
21
Diagnosis 1.Abdominal palpation: -detects as few as 30% of SFD’s 2.SFH measurement: -sensitivity 27%, specificity 88% 3.Ultrasound anthropometry: -abdominal circumference and estimated fetal weight predict SFD (AC 95%, EFW 90%) -10 th centile best predictive threshold -charts should be customised -velocity should be used in addition to size 4.Amniotic fluid volume: -poor predictive value in diagnosis, but useful surveillance tool
 -10 th centile best predictive threshold -charts should be customised -velocity should be used in addition to size 4.Amniotic fluid volume: -poor predictive value in diagnosis, but useful surveillance tool")
22
What surveillance is best?

23
Umbilical artery Doppler should be the primary surveillance tool A recent meta-analysis of18 studies (10,000 women) demonstrated that in high-risk pregnancy including FGR the use of Doppler ultrasound is associated with: a reduction in perinatal deaths fewer inductions of labour fewer caesarean sections no difference in operative vaginal deliveries no difference in Apgar scores <7 at five minutes. Alfrevic et al (2010)
.")
24
Surveillance if Umbilical Artery Doppler is normal There is no benefit in twice weekly Doppler Twice weekly Doppler results in earlier intervention without clear benefit in terms of morbidity/mortality Biophysical profile is of no proven benefit CTG is not associated with better fetal outcome

25
Surveillance if Umbilical Artery End Diastolic Flow is absent or reversed Optimal surveillance strategy is not clear Interval between first occurrence of AEDF and abnormal CTG/BPP ranges from 1-26 days Admit and administer antenatal steroids Additional Doppler assessment BPP has good negative predictive value Daily CTG Consider delivery if gestation >34/40

26
Umbilical artery (UMA): End-diastolic flow velocity (normal, reduced, absent, reversed) reflects increases in placental resistance Essential in surveillance of the growth restricted fetus Doppler parameters
: End-diastolic flow velocity (normal, reduced, absent, reversed) reflects increases in placental resistance Essential in surveillance of the growth restricted fetus Doppler parameters")
27
Middle Cerebral Artery (MCA): Represents downstream resistance in cerebral microcirculation MCA resistance is normally high throughout gestation, with increasing flow in the third trimester Increased diastolic flow signifies onset of circulatory changes in response to placental disease
: Represents downstream resistance in cerebral microcirculation MCA resistance is normally high throughout gestation, with increasing flow in the third trimester Increased diastolic flow signifies onset of circulatory changes in response to placental disease")
28
Venous Dopplers Information about the ‘pump’ Candidate vessels include IVC, UVC, and hepatic veins The ductus venosus is probably the vein of choice Waveform deterioration precedes, and strongly predicts, changes in BPS requiring delivery

30
Timing and mode of delivery

31
Delivery When umbilical artery Doppler is normal, delay delivery until at least 37 weeks (in the presence of satisfactory additional assessment) With AREDF consider delivery if gestation >34/40 even in the presence of normal additional assessment With AREDF, deliver before 34/40 if CTG abnormal, BPP abnormal, or other Doppler parameters are abnormal (MCA, umbilical vein) Mode of delivery will depend on gestation, presentation, fetal condition and maternal factors Caution with postmaturity
 With AREDF consider delivery if gestation >34/40 even in the presence of normal additional assessment With AREDF, deliver before 34/40 if CTG abnormal, BPP abnormal, or other Doppler parameters are abnormal (MCA, umbilical vein) Mode of delivery will depend on gestation, presentation, fetal condition and maternal factors Caution with postmaturity")
32
Interventions to improve outcome Poor evidence on effectiveness of antenatal support and treatment programmes from UK and US studies- largely comparable outcomes for all study groups (see NICE guidance). However, small numbers and methodological problems. One larger US study of approx 7000 women demonstrated improved outcomes in terms of gestation and weight at delivery with antenatal support and treatment. On balance, women are likely to have better continuity of care and access health care more readily with dedicated services.

33
Summary Whilst there is insufficient evidence that illicit drugs have a direct impact on fetal growth, women misusing substances often have multiple and complex social and medical risk factors for FGR Pregnancies associated with substance misuse are known to have a greater risk of perinatal morbidity and mortality Aside from an enhanced package of antenatal care, intensified fetal surveillance should be offered, including serial fetal growth assessments in the second and third trimester Where a growth deficit is identified, Doppler should be the primary surveillance tool Mode and timing of delivery will largely depend on fetal condition, gestation and maternal factors More data are needed to assess whether enhanced antenatal care results in improved fetal growth

Similar presentations



>")
















