Download presentation
Presentation is loading. Please wait.

1
Fetal Dopplers- A Review
Kemoria Granberry DO

3
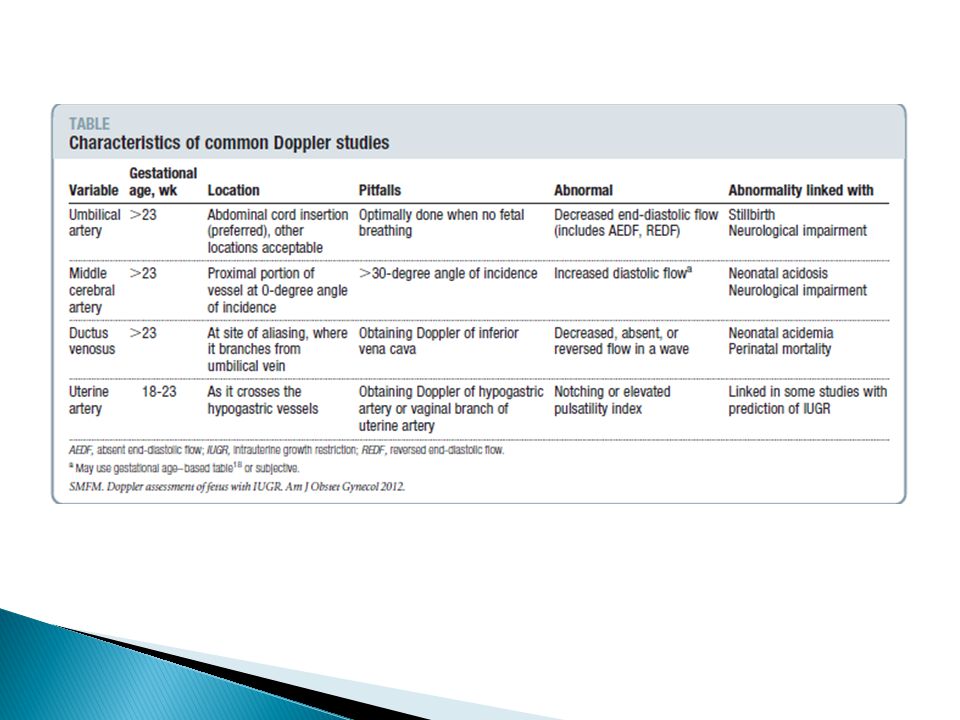
Types of Dopplers Arterial Venous Umbilical Middle Cerebral Uterine
Ductus venosus

4
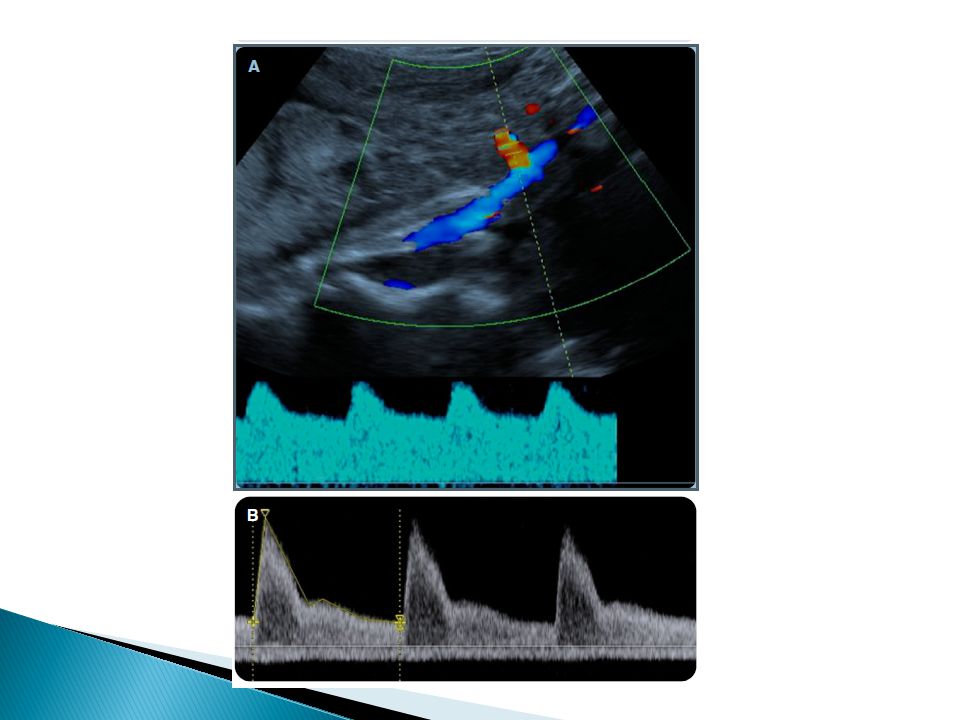
Umbilical Artery Fetal-placental unit Progression Measurements
DecreasedAbsentReversed Measurements S/D(Systolic to Diastolic) Ratio PI (Pulsatility Index) Uniformity Waveforms vary along length of cord Absence of fetal breathing Uniform waveforms Direct assessment of the fetal placental unit Remember the umbilical artery is derivative of common iliac without any somatic branch will give pretty accurate measure of placental perfusion Question: If someone has absent end diastolic flow, how is the S/D ration calculated? YOU CANT, USE THE PULSATILITY INDEX INSTEAD!! Close to placental insertion site downstream resistance to high velocity Close to abdominal insertion site
 Ratio. PI (Pulsatility Index) Uniformity. Waveforms vary along length of cord. Absence of fetal breathing. Uniform waveforms. Direct assessment of the fetal placental unit. Remember the umbilical artery is derivative of common iliac without any somatic branch will give pretty accurate measure of placental perfusion. Question: If someone has absent end diastolic flow, how is the S/D ration calculated YOU CANT, USE THE PULSATILITY INDEX INSTEAD!! Close to placental insertion site downstream resistance to high velocity. Close to abdominal insertion site")
5
Characteristics of Umbilical Artery waveform

6
Middle Cerebral Artery
Why the MCA? Progression Increased EDFV Decreased PI Measurement Peak Systolic Velocity Pulsatility Index Cerebro-placental ratio PEAK SYSTOLIC VELOCITY Why the MCA? -80% of cerebral blood flow -most accesable of cerebral vessels Pathology in chronic fetal hypoxemia, there is centrally sparing effects that causes preferential blood flow to brain and adrenals, with decreased peripheral blood flow

7
Characteristics of MCA waveform

8
Ductus Venosus Physiologic status of right ventricle Progression
Decreased Absent Reversed flow in a wave Measurement Uniformity?

9
Characteristics of DV waveform
-biphasic

10
Uterine Artery Progressive decrease in impedence throughout pregnancy
Abnormal trophblastic invasion Measurement Notch PI May reflect abnormal trophoblastic invasion if abnormal waveform

12
Q1: Should doppler ultrasound assessment be performed in low risk and/or high risk pregnancies as screening test for IUGR? Why is this an important question to ask? - If dopplers have been shown to predict fetal acidemia/stillbirth early detection may improve outcomes…ie BTMZ, early delivery, increased frequency of antenatal testing

13
Q1 Umbilical dopplers Uterine dopplers No Goffinet et al Chien et al
Meta analysis 1997 4 trials; n 11,275 Trials to date underpowered to determine utility of screening Uterine dopplers Chien et al Meta analysis 28 trials ; n=3000 Abnormal result more likely to predict IUGR (liklihood ratio) Cnossen et al 61 trials; n= 41000 Abnormal results corelated more with high risk pregnancies, though liklihood ratio remain high in low risk pregnancies as well Conclusions while these may be good tools they currently not standard of care because of lack of strong evidence, subjectivity of results (uterine art), age of surveillence.
 Cnossen et al. 61 trials; n= Abnormal results corelated more with high risk pregnancies, though liklihood ratio remain high in low risk pregnancies as well. Conclusions while these may be good tools they currently not standard of care because of lack of strong evidence, subjectivity of results (uterine art), age of surveillence.")
14
Q2: What are the benefits and limitations of doppler studies of each vessel when IUGR is suspected?

15
Q2 Umbilical Doppler Middle Cerebral Dopplers Venous Dopplers
Significant reductions in IOL, CS, perinatal deaths No validated interventions Middle Cerebral Dopplers May identify IUGR fetuses at risk for CS for NRFHT and neonatal acidosis May identify IUGR fetuses at risk for long term neurodevelopment delay in presence of normal umbilical dopplers Venous Dopplers Identifies severely compromised IUGR fetus No validated interventions shown that improve outcomes

17
Q3: What is the usual progression of doppler abnormalities in fetuses with suspected IUGR? Is this progression consistant/reliable?

18
Q3. Early – Brain sparing Late – Heart Sparing
Inc impedence in UA Dec impedence in MCA MCA normalization Late – Heart Sparing Inc flow through DV improve left ventricular output Increased Absent Reversed DV Increased central venous pressure Umbilical venous pulsations Validated in preterm idiopathic IUGR fetuses Changes can be variable, but there are some fairly predictable changes noted in setting hypoxemia Early – Brain sparing -preferenctial shunting of blood away from splanchnic circulation and to fetal heart/brains,/adrenal -think of MCA normalization similar to normalization of ABG in status asthmaticus when organism losing ability to adapt AS PLACENTAL DISEASE WORSENS AND MORE PLACENTAL VESSELS BECOME OBLITERATED LATE CHANGES OCCURS Late – Heart sparing -blood shunted via ductus venosus to left ventricle at the expense of fetal liver -the increased right ventricle afterload improves left ventricular outflow….but eventually cardiac compliance plus inc end diastolic pressure leads to ominous chnages in DV

19
Q4: What dopplers study regimen should be initiated for suspected IUGR
Q4: What dopplers study regimen should be initiated for suspected IUGR? What other antepartum testing may be helpful in this setting?

20
Q4. Initiate Frequency Other testing Viability
Suspected IUGR – differentiate hypoxic growth restricted fetus from non hypoxic small fetus Frequency Weekly, q 2-4 weeks, 3-4x’s a week Determined by severity of doppler abnormality Other testing Twice weekly NST with weekly AFI Weekly BPPs GOAL – REDUCE PERINATAL MORBIDITY/MORTALITY AND LIMIT UNNECCESSARY INTERVENTIONS Remember that few things actually improve perinatal outcomes BTMZ, latency abx, and ANT..including dopplers

21
What interventions are available and should be considered based on abnormal fetal doppler velocimetry studies?

22
Q5. Interventions BTMZ Hospitalization Timing of delivery ANT

Similar presentations