Download presentation
Presentation is loading. Please wait.

1
Farhan Hanif,MD Maternal Fetal Medicine
Doppler in Obstetrics Farhan Hanif,MD Maternal Fetal Medicine 1

2
Doppler assessment of the placental and fetal circulation is important tool screening for adverse pregnany outcomes

3
3

5
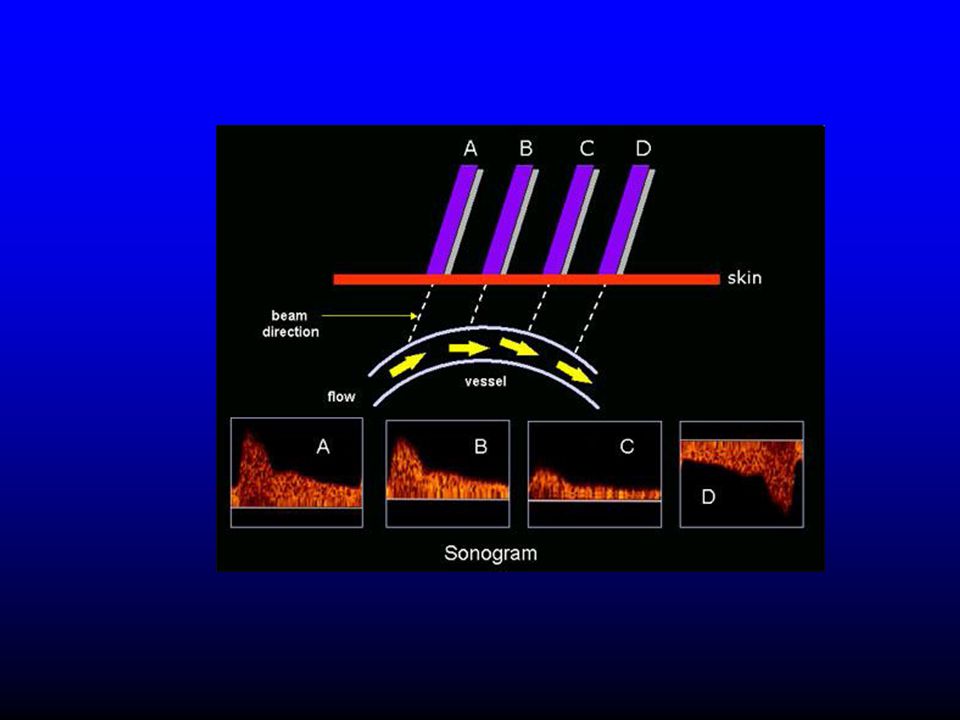
Angle Dependence 5

7
7

8
Doppler in IUGR EFW<10th %ile EFW <2SD above the mean
AC <5th %ile ACOG defines IUGR as EFW <10thile 8

9
Compensatory Mechanisms
Fetal Hypoxemia- placental insufficiency UA Blood flow Redistribution Brain, heart, adrenal Gland MCA PI AF Lung, kidney, bowel Echogenic Bowel 9

10
Decompensation Pressure in Rt Atrium / Dilatation of DV
Myocardial dysfunction Pressure in Rt Atrium / Dilatation of DV Abnormal Venous Doppler 10

11
Fetal Hypoxemia / Acidosis
Abnormalities in Central Control of FHR “ANS” or Direct Myocardial Depression Variability Baseline Deceleration 11

12
12

13
Abnormal Umbilical vein
Umbilical artery Abnormal Umbilical vein 13

14
Abnormal Umbilical vein Abnormal Umbilical artery
14

15
15

16
B = “Brain sparing effect”
MCA waveforms A = Normal Normal Brain Sparing B = “Brain sparing effect” 16

17
MCA Doppler In Anemia In Anemic fetuses, the PSV will inrease.
Obtaining PSV at 0 degrees angle is important in anemic fetuses. Increase False positive rate after 34 weeks

18
18

19
19

20
AGA IUGR a IUGR D S 20

21
Role of Ductus Venosus Baschat et al ultrasound obstet gynecol 2004 21

22
Temporal Sequence of Cardiovascular changes in IUGR fetuses
22

23
Ferrazi et al. US Obstet Gynecol 2002; 19: 140-6
23

24
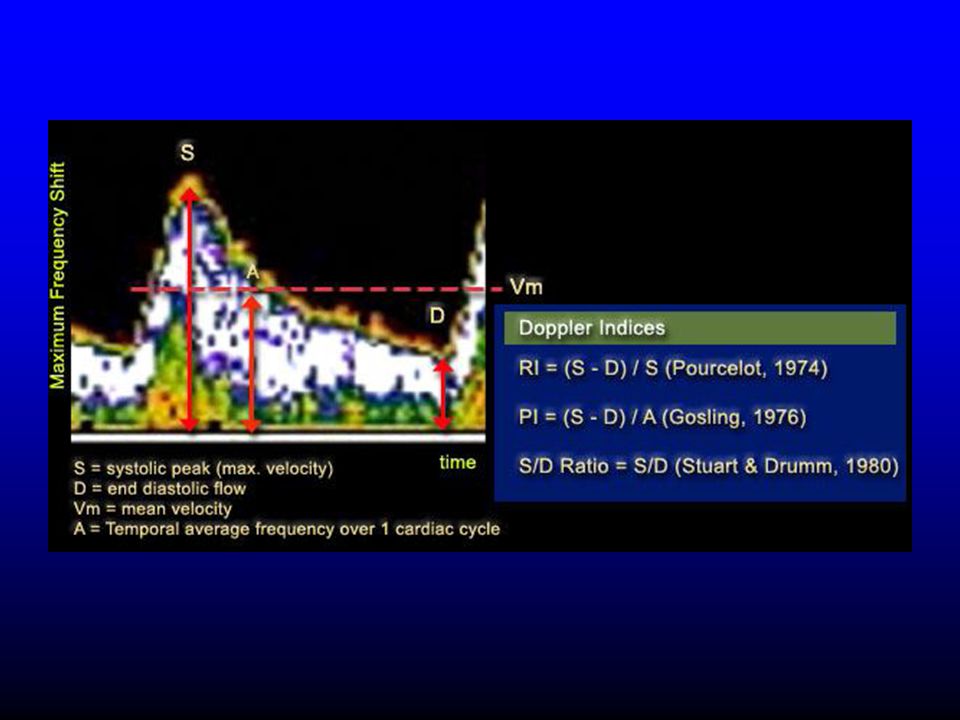
Doppler Indices and outcomes
In complicated pregnancies abnormal Doppler indices are powerful predictors of adverse perinatal outcome; Low Apgar score Nonreassuring fetal status Low pH Presence of thick meconium Admission to NICU (late and severe variable decelerations, absent variability, fetal scalp pH or umbilical cord arterial 24

25
Doppler Indices and outcomes
Reduce perinatal death and unnecessary induction of labor in the preterm growth restricted fetus. A meta-analysis use of Doppler ultrasonography reduced the odds of perinatal death by 38 percent (95% CI 15-55) Alfirevic Z et al Am J Obstet Gynecol 1995 25
 Alfirevic Z et al Am J Obstet Gynecol")
26
Umbilical Artery Absence or reversal of end-diastolic flow in the umbilical artery is suggestive of poor fetal condition, whereas normal or slightly decreased umbilical Doppler flow is rarely associated with significant morbidity and provides strong evidence of fetal well-being when delivery is delayed to achieve further fetal maturity Ott WJ J Ultrasound Med 2000 26

27
Repeat Doppler in 1-2 weeks
IUGR Doppler UA and MCA If Normal Repeat Doppler in 1-2 weeks If normal Serial Growth Scan 4 weeks interval Doppler UA and MCA every 1-2 weeks Evaluate MCA at term ?APFS Consider Delivery at 39 weeks 27

28
Abnormal Doppler UA and MCA
Present DV Normal Absent/Reverse EDF Ab/Reverse Present DV EDF Growth Scan 2-4 wks Weekly UA, MCA,+/-DV Admit Steroids NST q shift and daily BPP Admit Steroids Continuous monitoring May follow as outpatient BMZ,APFS Deliver at 32-34wks Abnormal APFS ?Timing of Delivery Consider Delivery at weeks 28

29
Absent or Reversed Flow in the Ductus Venosus
EGA <30weeks >30weeks Deliver Continuous Monitoring Daily BPP Daily Doppler Evaluate AoA, Valves Deliver for Abnormal BPP,FHT ?Reversed AoA,E:A Ratio 29

30
Doppler in AGA Fetuses Routine screening with dopplers in AGA fetuses is controversial However, abnormal UA identifies the fetuses at risk in uncomplicated pregnancies as DM Ch HTN SLE Maternal autoimmune Twins Postterm Most sensitive 30

31
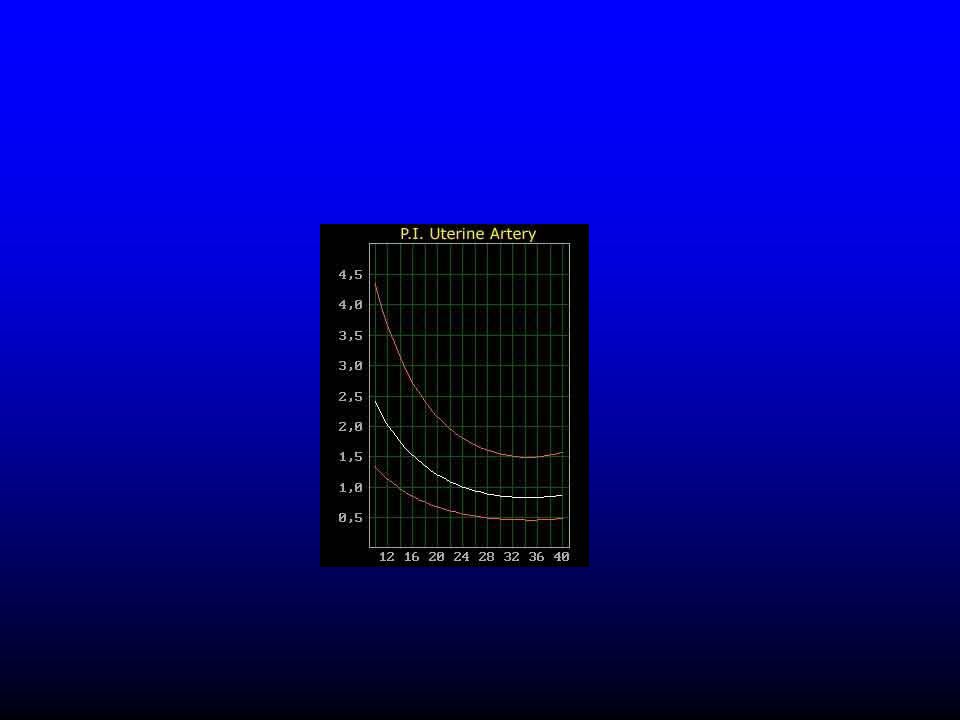
Uterine Artery Doppler

32
Uterine Artery Doppler
First trimester Early 2nd Trimester Late 2nd trimester

34
Prediction of PE Outcome Sensitivity Specificity NPV PE 78 95 99
IUGR <10 23 96 IUGR <3 36 92

35
Prevention Study n Condition Outcome McParland et al 100 PE
ASA 2%, P 19% Bower et al 60 Severe PE ASA 13%, P 38% Morris et al 102 ASA 8%, P 14% (NS)
")
36
Uterine Artery in 1st trimester
7797 women with singleton pregnancies at 11 to 13 weeks. In 34 women , at < 34 weeks. At a 5% FPR; The sensitivity percent The specificity was 94.3 percent

37
Doppler in first Trimester
Increases the sensitivity of first trimester screening and decreases the false postivie rate DV reversed flow in DV in first trimester is a risk factor for CHD even in the presence of normal NT Can be used as a part of risk calculation for stillbirth CAN be used as a tool to

Similar presentations


: Part 3 – Antepartum>")
















